
Development of a Novel Design and Subsequent Fabrication of an Automated Touchless Hand Sanitizer Dispenser to Reduce the Spread of Contagious Diseases

 ,
,  , , ,
, , ,  and
and
Abstract
:1. Introduction
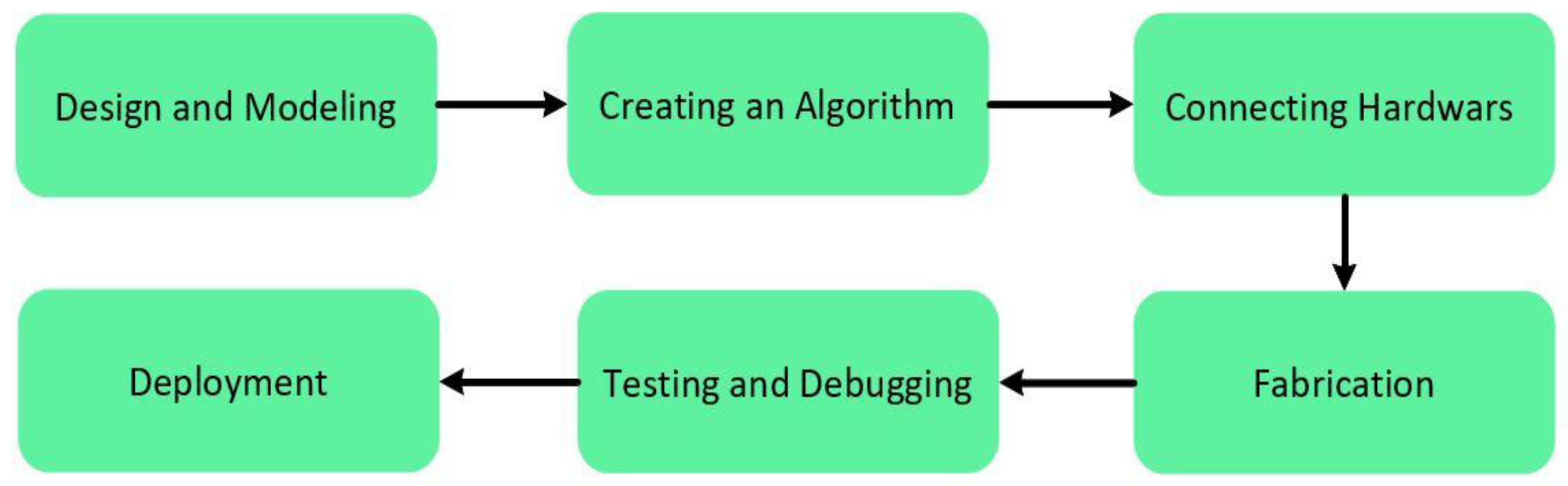
2. Materials and Methods
2.1. Design and Modeling
Theoretical Aspect
2.2. Control System and Connection
2.2.1. L298 Controller Connection
- The absolute maximum for any single IO pin is 40 mA (basically, it is the threshold at which Atmel can no longer guarantee that the chip will not be damaged);
- The total current from all the IO pins together is 200 mA max;
- The 5 V output pin is good for ~400 mA on USB, ~900 mA when using an external power adapter;
- The 900 mA is for an adapter that provides ~7 V. As the adapter voltage increases, the heat regulator has to deal with also increased values, so the maximum current will drop as the voltage increases. This is called thermal limiting.
- The pump will not run due to the low power supply;
- If the pump runs, the temperature of the voltage regulators will rise instantly and due to thermal limiting, the whole system will shut down temporarily;
- The motor pump will draw out the maximum threshold current and as a result, the chip can be damaged.
2.2.2. LDR Connection
2.2.3. Sanitizer Level Indicator
2.3. Creating an Algorithm
Programming, Coding, and Debugging
2.4. Fabrication Process
Preparation of Hand Sanitizer
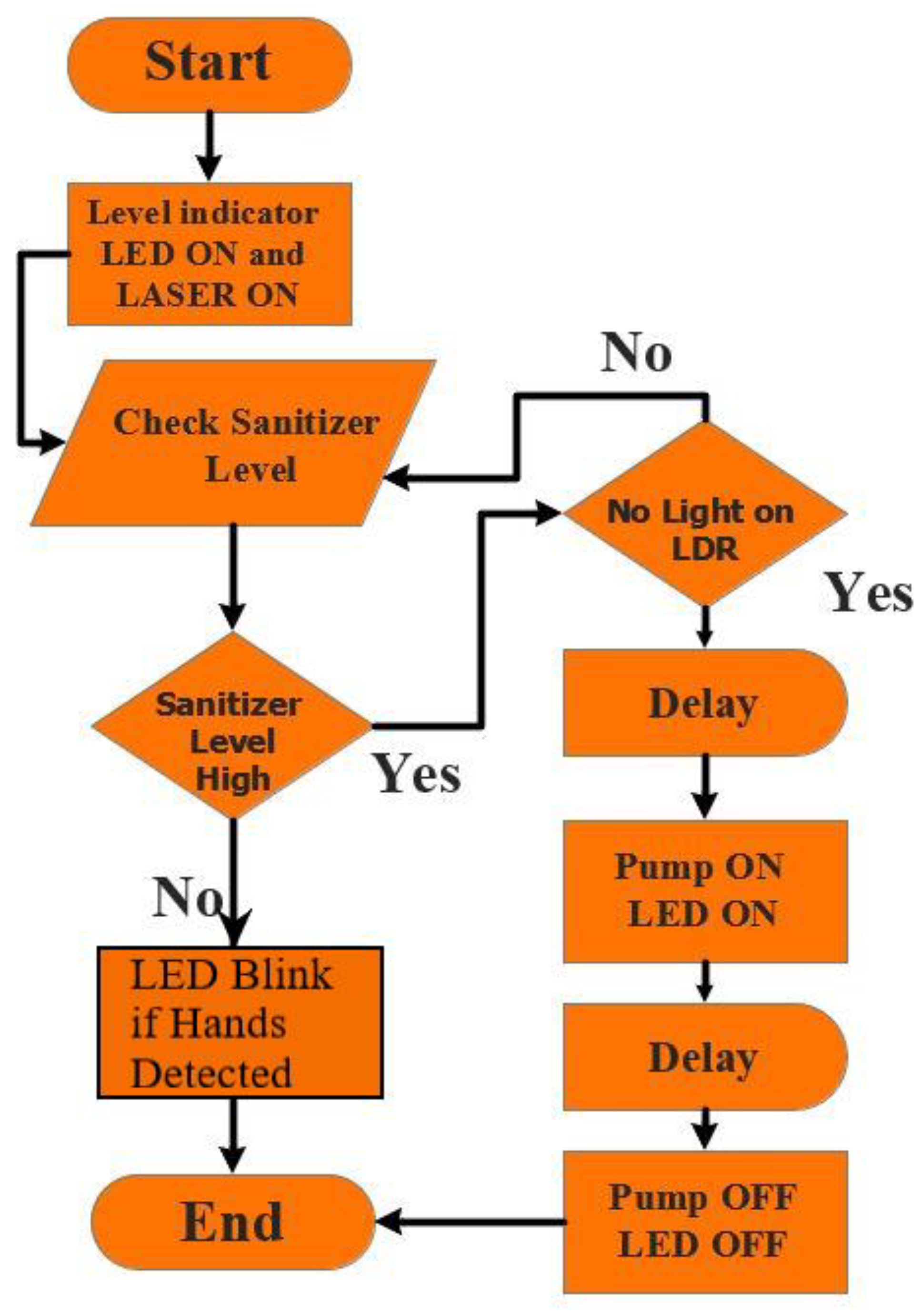
3. Working Principle of the Dispenser
4. Results and Discussion
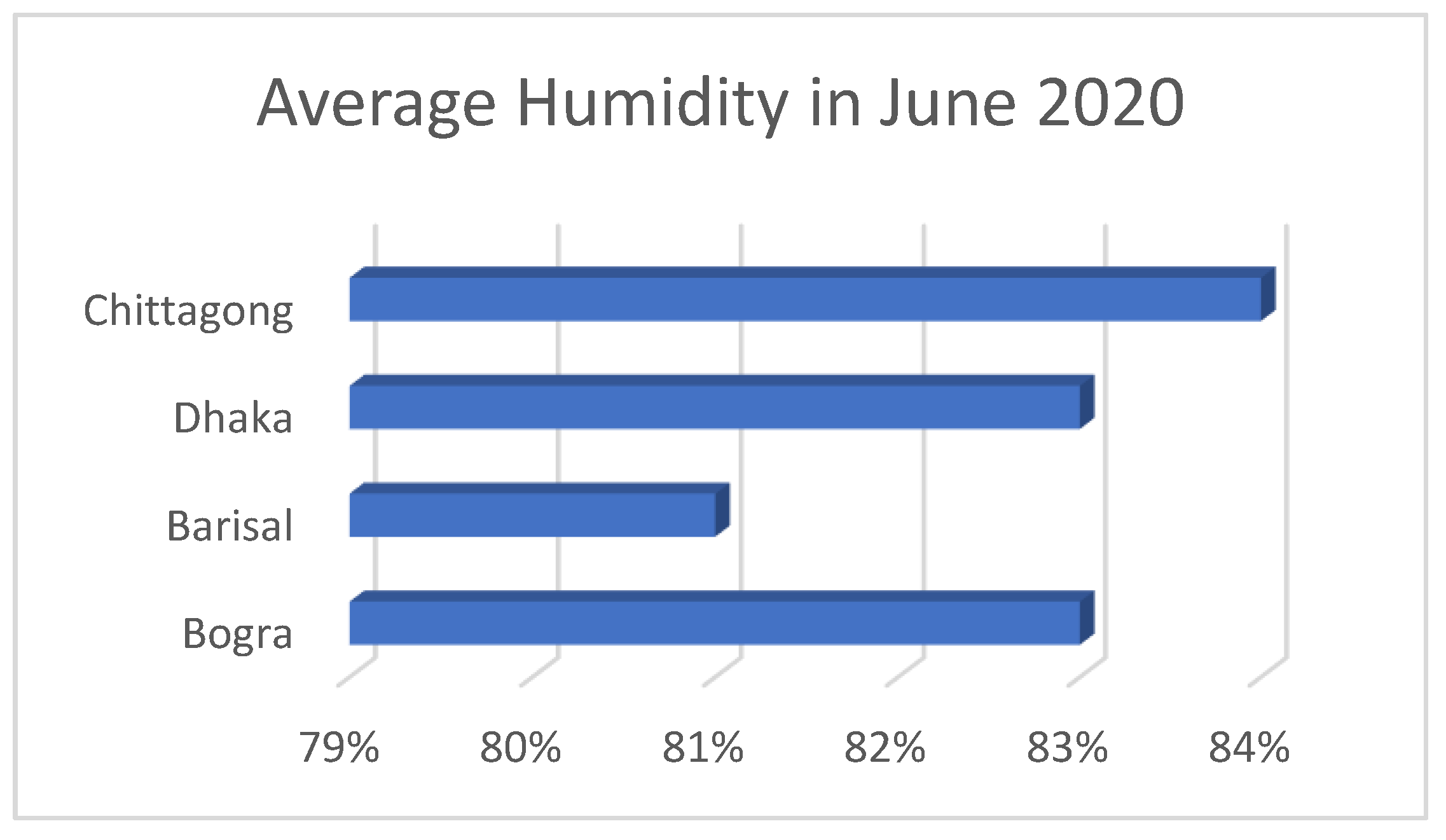
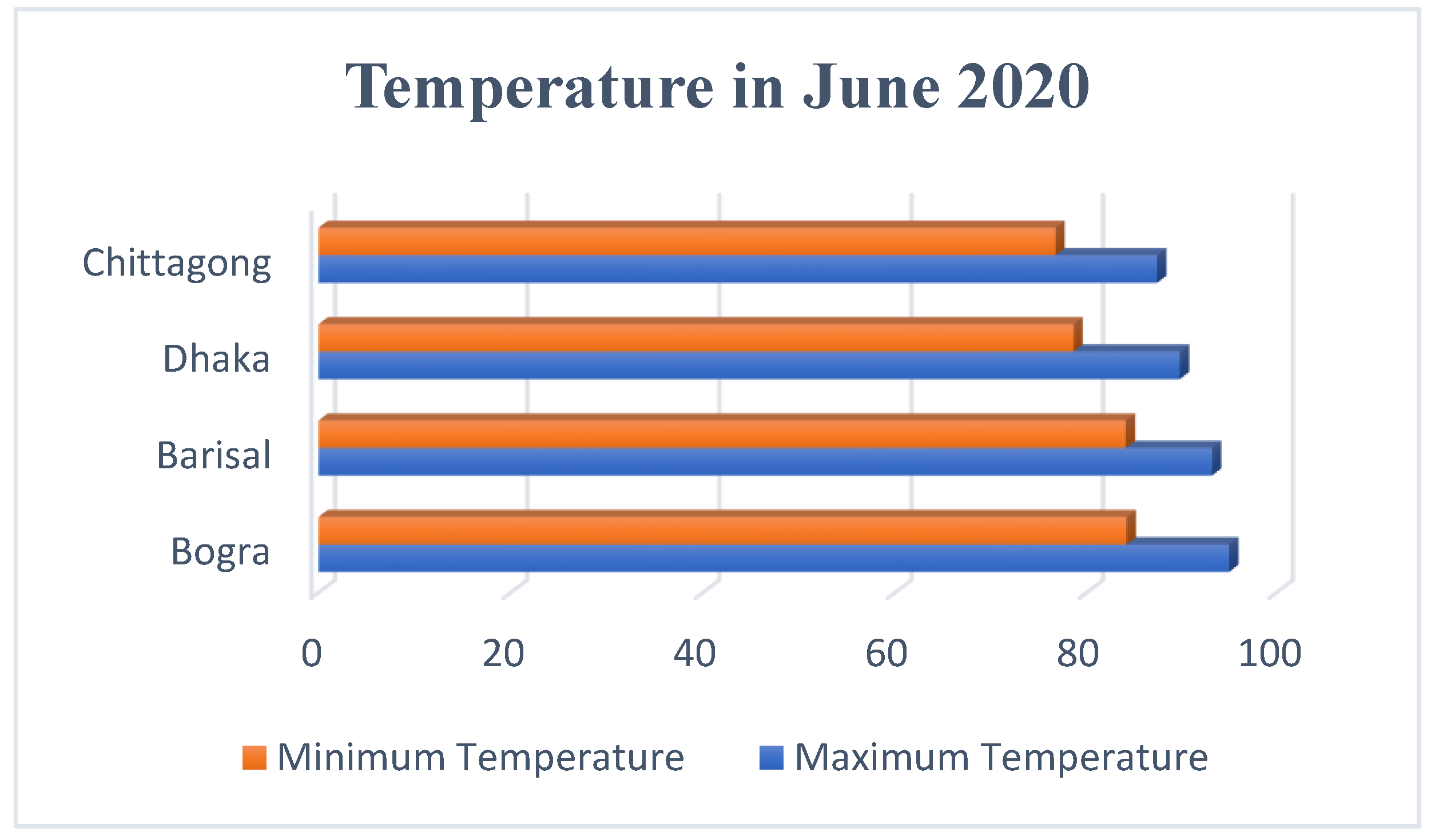
Deployment and Performance Analysis of the Device
5. Conclusions
- Superior performances for indoor use;
- Consumes low power; while in standby mode it consumes only 0.05 mA, and during the operating cycle it consumes about 12 V and 0.5 A;
- Cheap readymade components like Arduino Uno, L298 motor driver, 5 V laser, 5 mm LDR are used. As a result, this device can be made at a low cost with a price range from about USD 20 to 25;
- LDR sensor is more efficient to be used for proximity sensing than ultrasonic sensor in the case of the outdoor use of this dispenser.
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Nomenclature
| V | Fluid velocity (m/s) |
| P | Fluid pressure (N/m2) |
| g | Gravitational acceleration (m/s2) |
| γ | Specific weight (N/m3) |
| Z | Potential energy per unit weight (J/kg) |
| Q | Volumetric flow rate (m3/s) |
| r | Radius (m) |
| ΔH | The head imparted to liquid by the pump (m) |
| H | Height (m) |
| V0 | Voltage at A0 pin of Arduino (Volt) |
| R1 | 10 kΩ resistance |
| R2 | Resistance value of LDR (kΩ) |
References
- World Health Organization. WHO Guidelines on Hand Hygiene in Health Care. First Global Patient Safety Challenge Clean Care Is Safer Care. World Alliance for Patient Safety; WHO: Geneva, Switzerland, 2009. [Google Scholar]
- Pittet, D.; Allegranzi, B.; Boyce, J. World Health Organization world alliance for patient safety first global patient safety challenge core group of experts. The World Health Organization guidelines on hand hygiene in health care and their consensus recommendations. Infect. Control Hosp. Epidemiol. 2009, 30, 611–622. [Google Scholar] [CrossRef] [PubMed]
- White, C.; Kolble, R.; Carlson, R.; Lipson, N.; Dolan, M.; Ali, Y.; Cline, M. The effect of hand hygiene on illness rate among students in university residence halls. Am. J. Infect. Control 2003, 31, 364–370. [Google Scholar] [CrossRef]
- Ehrenkranz, N.J.; Alfonso, B.C. Failure of bland soap handwash to prevent hand transfer of patient bacteria to urethral catheters. Infect. Control Hosp. Epidemiol. 1991, 12, 654–662. [Google Scholar] [CrossRef] [PubMed]
- Fournier, A.K.; Berry, T.D. Effects of response cost and socially-assisted interventions on hand-hygiene behavior of university students. Behav. Soc. Issues 2012, 21, 152–164. [Google Scholar] [CrossRef] [Green Version]
- Eiref, S.D.; Leitman, I.M.; Riley, W. Hand sanitizer dispensers and associated hospital-acquired infections: Friend or fomite? Surg. Infect. 2012, 13, 137–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Würtz, R.; Moye, G.; Jovanovic, B. Handwashing machines, handwashing compliance, and potential for cross-contamination. Am. J. Infect. Control 1994, 22, 228–230. [Google Scholar] [CrossRef]
- Bal, M.; Abrishambaf, R. A system for monitoring hand hygiene compliance based-on Internet-of-Things. In Proceedings of the IEEE International Conference on Industrial Technology (ICIT), Toronto, ON, Canada, 22–25 March 2017; pp. 1348–1353. [Google Scholar]
- Rabeek, S.M.; Norman, A.; Je, M.; Raja, M.K.; Peh, R.F.; Dempsey, M.K. A reliable handwash detector for automated hand hygiene documentation and reminder system in hospitals. In The 15th International Conference on Biomedical Engineering 2014; Springer: Cham, Switzerland, 2014; pp. 892–895. [Google Scholar]
- Zivich, P.N.; Huang, W.; Walsh, A.; Dutta, P.; Eisenberg, M.; Aiello, A.E. Measuring office workplace interactions and hand hygiene behaviors through electronic sensors: A feasibility study. PLoS ONE 2021, 16, e0243358. [Google Scholar] [CrossRef]
- Karn, A.; Kanchi, R.; Deo, S.S.; Acres, E. Design and development of an automated monitored hand hygiene system to curb infection spread in institutional settings during COVID-19 Pandemic. In Proceedings of the International Conference on Advances in the Field of Health, Safety, Fire, Environment & Allied Sciences (HSFEA 2020), Dehradun, India, 18–19 December 2020. [Google Scholar]
- Patra, R.; Bhattacharya, M.; Mukherjee, S. IoT-based computational frameworks in disease prediction and healthcare management: Strategies, challenges, and potential. In IoT in Healthcare and Ambient Assisted Living; Marques, G., Bhoi, A.K., de Albuquerque, V.H.C., Hareesha, K.S., Eds.; Springer: Singapore, 2021; pp. 17–41. [Google Scholar]
- Nair, S.; Scurtu, I.C.; Hudișteanu, S.V. 10. Integrated health monitoring & disinfecting system for organizations and societies. In Proceedings of the International Conference Building Services and Energy Efficiency, Iasi, Romania, 2–3 July 2020; pp. 104–119. [Google Scholar]
- Hong, T.S.; Bush, E.C.; Hauenstein, M.F.; Lafontant, A.; Li, C.; Wanderer, J.P.; Ehrenfeld, J.M. A hand hygiene compliance check system: Brief communication on a system to improve hand hygiene compliance in hospitals and reduce infection. J. Med. Syst. 2015, 39, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, B.; De, T. An Internet of Things Assisted Smart Hand Sanitizer with Health Monitoring System Help to Reduce Rapid Spread of COVID-19. Available online: https://easychair.org/publications/preprint/nLwv (accessed on 19 March 2021).
- Baslyman, M.; Rezaee, R.; Amyot, D.; Mouttham, A.; Chreyh, R.; Geiger, G. Towards an RTLS-based hand hygiene notification system. Procedia Comput. Sci. 2014, 37, 261–265. [Google Scholar] [CrossRef] [Green Version]
- Rojo, M.G.; Sy, J.B.; Calibara, E.R.; Comendador, A.V.; Degife, W.; Sisay, A. Non-contact temperature reader with sanitizer dispenser (NCTRSD). Int. J. Sci. Res. Publ. 2020, 10, 583–593. [Google Scholar] [CrossRef]
- Srihari, M.M. Self-activating sanitizer with battery imposed system for cleansing hands. In Proceedings of the 2nd International Conference on Inventive Research in Computing Applications (ICIRCA), Coimbatore, India, 15–17 July 2020; pp. 1102–1105. [Google Scholar]
- Lee, J.; Lee, J.-Y.; Cho, S.-M.; Yoon, K.-C.; Kim, Y.J.; Kim, K.G. Design of automatic hand sanitizer system compatible with various containers. Healthc. Inform. Res. 2020, 26, 243–247. [Google Scholar] [CrossRef] [PubMed]
- Eddy, Y.; Mohammed, M.N.; Daoodd, I.I.; Bahrain, S.H.; Al-Zubaidi, S.; Al-Sanjary, O.I.; Sairah, A.K. 2019 Novel Coronavirus Disease (Covid-19): Smart contactless hand sanitizer-dispensing system using IoT based robotics technology. Rev. Argent. Clin. Psicol. 2020, 29, 215–220. [Google Scholar] [CrossRef]
- Çengel, Y.A.; Cimbala, J.M. Fluid Mechanics: Fundamentals and Applications; McGraw-Hill Education: New York, NY, USA, 2018. [Google Scholar]
- Atmel. 8-bit AVR Microcontrollers. ATmega328/P. 2016. [Google Scholar]
- Pittet, D.; Hugonnet, S.; Harbarth, S.; Mourouga, P.; Sauvan, V.; Touveneau, S.; Perneger, T.V. Effectiveness of a hospital-wide programme to improve compliance with hand hygiene. Lancet 2000, 356, 1307–1312. [Google Scholar] [CrossRef]
- Larson, E.L.; Eke, P.I.; Laughon, B.E. Efficacy of alcohol-based hand rinses under frequent-use conditions. Antimicrob. Agents Chemother. 1986, 30, 542–544. [Google Scholar] [CrossRef] [Green Version]
- Larson, E.L.; Aiello, A.E.; Bastyr, J.; Lyle, C.; Stahl, J.; Cronquist, A.; Lai, L.; Della-Latta, P. Assessment of two hand hygiene regimens for intensive care unit personnel. Crit. Care Med. 2001, 29, 944–951. [Google Scholar] [CrossRef] [PubMed]
- Widmer, A.F. Replace hand washing with use of a waterless alcohol hand rub? Clin. Infect. Dis. 2000, 31, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Maury, E.; Alzieu, M.; Baudel, J.L.; Haram, N.; Barbut, F.; Guidet, B.; Offenstadt, G. Availability of an alcohol solution can improve hand disinfection compliance in an intensive care unit. Am. J. Respir. Crit. Care Med. 2000, 162, 324–327. [Google Scholar] [CrossRef] [PubMed]
- Bischoff, W.E.; Reynolds, T.M.; Sessler, C.N.; Edmond, M.B.; Wenzel, R.P. Handwashing compliance by health care workers: The impact of introducing an accessible, alcohol-based hand antiseptic. Arch. Intern. Med. 2000, 160, 1017–1021. [Google Scholar] [CrossRef] [PubMed]
- Adarsh, S.; Kaleemuddin, S.M.; Bose, D.; Ramachandran, K.I. Performance comparison of Infrared and Ultrasonic sensors for obstacles of different materials in vehicle/robot navigation applications. IOP Conf. Ser. Mater. Sci. Eng. 2016, 149, 012141. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Major Components | Manufacturer/Brand | Advantages | Price (USD) |
|---|---|---|---|
| R3 Board ATmega328P with USB Cable for Arduino-Compatible | Kuman |
| 10.690 |
| MCIGICM Photoresistor Photo Light Sensitive Resistor, Light Dependent Resistor 5 mm | MCIGICM |
| 0.133 |
| HiLetgo® L298N Motor Drive Controller Board Module Dual H Bridge DC Stepper For Arduino | HiLetgo® |
| 2.470 |
| Uxcell Female DC Power Jack Socket Connector | Uxcell |
| 1.018 |
| HiLetgo 5V 650 nm 5 mW Red Dot Laser Head Red Laser Diode Laser Tube with Leads Head Outer Diameter 6mm | HiLetgo® |
| 0.599 |
| EDGELEC 100 K ohm Resistor 1/4 w (0.25 Watt) ± 1% Tolerance Metal Film Fixed Resistor | EDGELEC |
| 0.057 |
| JOVNO 12V 1A Power Supply Adapter 100–240 V AC to DC 12volt 12 W 1amp 800 mA 500 mA Power Converter Transformer with 5.5 × 2.5 mm Tip | JOVNO |
| 3.990 |
| Zlolia 12 V Waterproof LED Strip Light 5 M 300LEDs | Zlolia |
| 0.010 |
| Mini DC Brushless Water Pump JT-600C-12 16 mm Internal Thread | Zjchao |
| 6.280 |
| Physical Quantity or Measurand | Parameters | Units (cm) |
|---|---|---|
| Basement | Length (l) × width (w) | 20 × 20 |
| Sidewall | Length, l1, l2 | 27, 32 |
| Laser detection chamber | Height, hc | 13 |
| Formulation | Required Ingredients (Starting % of Ingredient) | Concentrations in Final Product, % (v/v), (Final % of Ingredient) | Required Volume of Ingredients for 10-L Preparation, mL |
|---|---|---|---|
| 1 | (i). Ethanol 96% | 80 | 8333 |
| (ii). Hydrogen peroxide 3% | 0.125 | 417 | |
| (iii). Glycerol 98 | 1.45 | 145 | |
| (iv). Sterile distilled water or boiled cold water | --- | 1105 | |
| 2 | (i). Isopropanol 99.8% | 75 | 7515 |
| (ii). Hydrogen peroxide 3% | 0.125 | 417 | |
| (iii). Glycerol 98% | 1.45 | 145 | |
| (iv). Sterile distilled water or boiled cold water | --- | 1923 |
| Deployed Locations | Address | GPS Coordinates | Number of Machines | Placement Environment | Observed Working Condition |
|---|---|---|---|---|---|
| Shaheed Ziaur Rahman Medical College | Bogra City Bypass, Bogura 5800 | 24°49′40.6″ N 89°21′10.8″ E | 1 | Indoor | Working |
| Mohammad Ali Hospital | 01 Sherpur Rd, Bogura 5800 | 24°50′08.2″ N 89°22′27.0″ E | 1 | Indoor | Working |
| Choumatha Markaj Jame Masjid | C & B Rd, Bhanga-Barisal Hwy, Barishal 8200 | 22°42′02.9″ N 90°21′11.4″ E | 1 | Outdoor | Malfunctioned |
| Chittagong Medical College Hospital | 57 K.B. Fazlul Kader Rd, Chattogram 4203 | 22°21′33.7″ N 91°49′50.6″ E | 8 | Four Indoor Four Outdoor | Working One unit minor malfunction |
| Nagar Bhaban | Batali Hill, Tiger Pass, Chattogram | 22°20′39.9″ N 91°48′51.3″ E | 2 | Indoor | Working |
| GEC Circle Bus Stop | GEC More, Chattogram | 22°21′32.7″ N 91°49′16.5″ E | 1 | Outdoor | Minor malfunction |
| Askar Ali Jame Masjid | Gundip, Anowara, Chattogram | 22°20’22.1″ N 91°84’33.1″ E | 1 | Outdoor | Working |
| Sadar Thana Bogura | Bogura | 24°51’01.6″ N 89°22’22.1″ E | 1 | Indoor | Working |
| Satmatha Traffic Police Box | Park Rd, Bogra | 24°50′50.8″ N 89°22′21.3″ E | 1 | Outdoor | Malfunctioned |
| Chatori Choumohoni Bazar | Gundip, Anowara, Chattogram | 22°23′27.4″ N 91°87′18.1″ E | 1 | Indoor | Working |
| Bangladesh Awami League Central Office | 23 Bangabandhu Ave, Dhaka | 23°43′36.3″ N 90°24′40.4″ E | 2 | Indoor | Working |
| Name | Price in (USD) | Sensor | Power Consumption/Cycle (W) P = VI |
|---|---|---|---|
| Bremmer Hand Sanitizer Dispenser Wall Mounted (1000 mL) | 73.0583 Approx. | Infrared sensor | 4 AA dry cell batteries. (1.5 V–0.5 Amp) 3 W |
| Zurio Automatic Hand Sanitizer Dispenser Wall Mount (450 mL) | 59.99 | Infrared sensor | 12 V–0.5 A 6 W |
| JS LifeStyle Automatic Hand Sanitizer Dispenser (1000 mL) | 29.99 | Infrared sensor | 3 AA battery (1.5 V–0.5 A) 2.25 W |
| Luxtonusa Automatic Hand Sanitizer Dispenser (500 mL) | 179.95 | Motion activated sensor | 4 C-sized battery (1.5 V–3.8 A) 22.8 W |
| CasaTimo Automatic Touchless Hand Sanitizer Dispenser (450 mL) | 35.99 | Motion activated sensor | 4 AA dry cell batteries. (1.5 V–0.5 Amp) 3 W |
| Safeline 360 Automatic Sanitizer/soap Dispenser (1000 mL) | 59 | Infrared sensor | 4 AA dry cell batteries. (1.5 V–0.5 Amp) 3 W |
| Guukar Automatic Soap Dispenser Hand Sanitizer (500 mL) | 41.99 | Infrared sensor | 4 AA dry cell batteries. (1.5 V–0.5 Amp) 3 W |
| Kent Auto Hand Sanitizer Dispenser (12,000 mL) | 161.846 Approx. | Infrared sensor | Input: 230 V AC 24 V DC–1.5 A Total rated Consumption: 40 W |
| SaniQuick Touch Free Soap and Sanitizer Dispenser (3200 mL) | 155.102 Approx. | Ultrasonic sensor | Input: 220 V AC |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Das, A.; Barua, A.; Mohimin, M.A.; Abedin, J.; Khandaker, M.U.; Al-mugren, K.S. Development of a Novel Design and Subsequent Fabrication of an Automated Touchless Hand Sanitizer Dispenser to Reduce the Spread of Contagious Diseases. Healthcare 2021, 9, 445. https://doi.org/10.3390/healthcare9040445
Das A, Barua A, Mohimin MA, Abedin J, Khandaker MU, Al-mugren KS. Development of a Novel Design and Subsequent Fabrication of an Automated Touchless Hand Sanitizer Dispenser to Reduce the Spread of Contagious Diseases. Healthcare. 2021; 9(4):445. https://doi.org/10.3390/healthcare9040445
Chicago/Turabian StyleDas, Arnab, Adittya Barua, Md. Ajwad Mohimin, Jainal Abedin, Mayeen Uddin Khandaker, and Kholoud S. Al-mugren. 2021. "Development of a Novel Design and Subsequent Fabrication of an Automated Touchless Hand Sanitizer Dispenser to Reduce the Spread of Contagious Diseases" Healthcare 9, no. 4: 445. https://doi.org/10.3390/healthcare9040445