
Economic Evaluation of Emotional and Personal Support in the Health Care of Women with Disabilities


Abstract
:1. Introduction
2. Materials and Methods
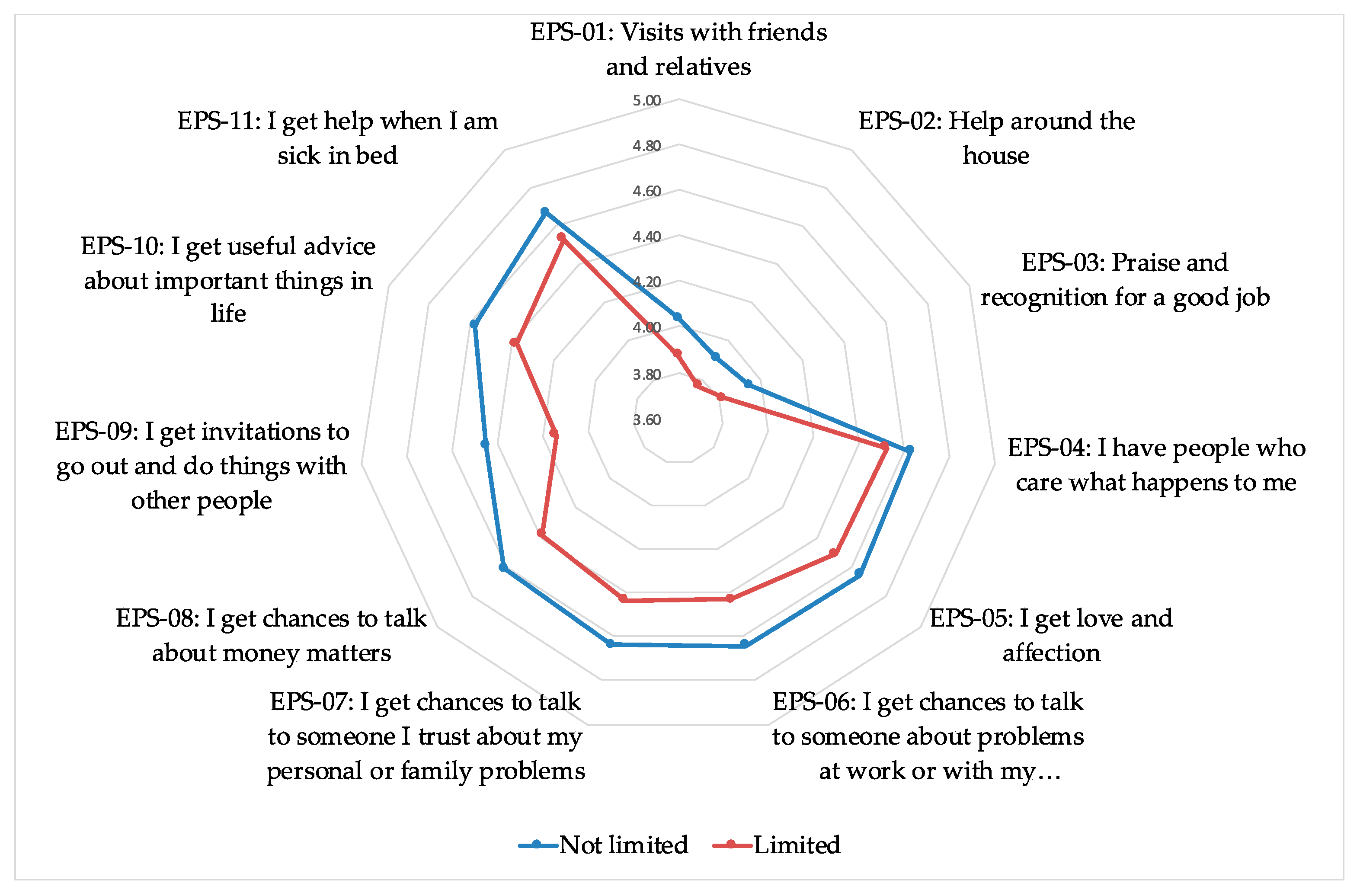
- EPS-01: Visits with friends and relatives.
- EPS-02: Help around the house.
- EPS-03: Praise and recognition for a good job.
- EPS-04: I have people who care what happens to me.
- EPS-05: I get love and affection.
- EPS-06: I get chances to talk to someone about problems at work or with my housework.
- EPS-07: I get chances to talk to someone I trust about my personal or family problems.
- EPS-08: I get chances to talk about money matters.
- EPS-09: I get invitations to go out and do things with other people.
- EPS-10: I get useful advice about important things in life.
- EPS-11: I get help when I am sick in bed.
- Number of times the respondent has consulted a general practitioner or family doctor in the past four weeks.
- Number of times the respondent has consulted a specialist in the last four weeks.
- Number of times respondent has been hospitalized in the past twelve months, excluding childbirth or caesarean sections.
- Admission to a day hospital over the past twelve months for intervention, treatment, or to have a test done.
- Use of any emergency service in the past twelve months.
- Use of other services over the past 12 months: Physiotherapist over the past twelve months (dichotomous variable).
- Use of other services over the past 12 months: Psychologist, Psychotherapist or Psychiatrist (dichotomous variable).
- Use of other services over the past 12 months: Nurse or Midwife (dichotomous variable).
- Diagnostic tests carried out in the past 12 months: X-ray (dichotomous variable).
- Diagnostic tests carried out in the past 12 months: CAT scan (dichotomous variable).
- Diagnostic tests carried out in the past 12 months: Ultrasound (dichotomous variable).
- Diagnostic tests carried out in the past 12 months: MRI (dichotomous variable).
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Council of Europe: Committee of Ministers, Recommendation Rec(2006)5 of the Committee of Ministers to Member States on the Council of Europe Action Plan to Promote the Rights and Full Participation of People with Disabilities in Society: Improving the Quality of Life of People with Disabilities in Europe 2006–2015, 5 April 2006, Rec(2006)5. Available online: https://www.refworld.org/docid/4a54bc3f1a.html (accessed on 28 January 2021).
- European Commission. Communication from the Commission to the European Parliament, the Council, the European Economic and Social Committee and the Committee of the Regions Establishing a European Pillar of Social Rights (COM/2017/0250 Final); Publication Office of European Union, Directorate-General for Employment, Social Affairs and Inclusion: Brussels, Belgium, 2017; Available online: https://doi.org/10.2792/506887 (accessed on 28 January 2021).
- Pérez, L.C. Discapacidad y Atención Sanitaria; CERMI: Madrid, Spain, 2006; Available online: https://www.cermi.es/es/colecciones/volumen-28-discapacidad-y-asistencia-sanitaria (accessed on 2 February 2021).
- Aday, L.A.; Andersen, R.M. The national profile of access to medical care: Where do we stand? Am. J. Public Health 1984, 74, 1331–1339. [Google Scholar] [CrossRef] [Green Version]
- Whitehead, M. The concepts and principles of equity and health. Int. J. Health Serv. 1992, 22, 429–455. [Google Scholar] [CrossRef] [PubMed]
- Graham, H. Building an interdisciplinary science of health inequalities: The example of lifecourse research. Soc. Sci. Med. 2002, 55, 2005–2016. [Google Scholar] [CrossRef]
- Okoro, C.A.; Zhao, G.; Fox, J.B.; Eke, P.I.; Greenlund, K.J.; Town, M. Surveillance for Health Care Access and Health Services Use, Adults Aged 18–64 Years-Behavioral Risk Factor Surveillance System, United States, 2014. MMWR Surveill. Summar. 2017, 66, 1–42. [Google Scholar] [CrossRef] [PubMed]
- Bertakis, K.D.; Azari, R.; Helms, L.J.; Callahan, E.J.; Robbins, J.A. Gender differences in the utilization of health care services. J. Fam. Pract. 2000, 49, 147–152. [Google Scholar] [PubMed]
- Redondo-Sendino, A.; Guallar-Castillón, P.; Banegas, J.R.; Rodríguez-Artalejo, F. Gender differences in the utilization of health care services among the older adult population of Spain. BMC Public Health 2006, 6, 155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rohlfs, I.; Borrell, C.; Anitua, C.; Artazcoz, L.; Colomer, C.; Escribá, V.; García-Calvente, M.; Llacer, A.; Mazarrasa, L.; Pasarín, M.I.; et al. La importancia de la perspectiva de género en las encuestas de salud. Gac. Sanit. 2000, 14, 146–155. [Google Scholar] [CrossRef] [Green Version]
- Kruk, M.E.; Gage, A.D.; Arsenault, C.; Jordan, K.; Leslie, H.H.; Roder-DeWan, S.; Adeyi, O.; Barker, P.; Daelmans, B.; Doubova, S.V.; et al. High-quality health systems in the Sustainable Development Goals era: Time for a revolution. Lancet Glob. Health Commun. 2018, 6, 1196–1252. [Google Scholar] [CrossRef] [Green Version]
- Dejong, G.; Batavia, A.I.; Griss, R. America’s neglected health minority: Working age persons with disabilities. Milbank Q. 1989, 67 (Suppl. 2), 311–351. [Google Scholar] [CrossRef]
- European Commission. Study on the Situation of Women with Disabilities in Light of the UN Convention for the Rights of Persons with Disabilities; Final Report for the DG Employment, Social Affairs and Equal Opportunities of the European Commission; ECOTEC: Birmingham, UK, 2009. [Google Scholar]
- Iezzoni, L.I.; McCarthy, E.P.; Davis, R.B.; Siebens, H. Mobility impairments and use of screening and preventive services. Am. J. Public Health 2000, 90, 955–961. [Google Scholar] [CrossRef] [PubMed]
- Bryant, T.; Leaver, C.; Dunn, J. Unmet healthcare need, gender, and health inequalities in Canada. Health Policy 2009, 91, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Fiorillo, D. Reasons for unmet needs for health care: The role of social capital and social support in some western EU countries. Int. J. Health Econ. Manag. 2020, 20, 79–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, L. Social Capital and Psychological Distress. J. Health Soc. Behav. 2011, 52, 478–492. [Google Scholar] [CrossRef] [PubMed]
- House, J.S.; Landis, K.; Umberson, D. Social relationships and health. Science 1988, 241, 540–545. [Google Scholar] [CrossRef]
- Kumar, S.; Calvo, R.; Avendano, M.; Sivaramakrishnan, K.; Berkman, L.F. Social support, volunteering and health around the world: Cross-national evidence from 139 countries. Soc. Sci. Med. 2012, 74, 696–706. [Google Scholar] [CrossRef]
- Perry, M.; Williams, R.L.; Wallerstein, N.; Waitzakin, H. Social capital and health care experiences among low-income individuals. Am. J. Public Health 2008, 98, 330–336. [Google Scholar] [CrossRef]
- Broadhead, W.E.; Gehlbach, S.H.; de Gruy, F.V.; Kaplan, B.H. The Duke-UNC Functional Social Support Questionnaire. Measurement of social support in family medicine patients. Med. Care 1988, 26, 709–723. [Google Scholar] [CrossRef]
- Bellón, J.A.; Delgado, A.; Luna, J.; Lardelli, P. Validez y fiabilidad del cuestionario de apoyo social funcional Duke-UNC-11. Atención Primaria 1996, 18, 153–163. [Google Scholar]
- Van Oyen, H.; Bogaert, P.; Yokota, R.T.C.; Berger, N. Measuring disability: A systematic review of the validity and reliability of the Global Activity Limitations Indicator (GALI). Arch. Public Health 2018, 76, 25. [Google Scholar] [CrossRef] [Green Version]
- Bogaert, P.; Van Oyen, H.; Beluche, I.; Cambois, E.; Robine, J.M. The use of the global activity limitation indicator and healthy life years by member states and the European Commission. Arch. Public Health 2018, 76, 30. [Google Scholar] [CrossRef] [Green Version]
- Instituto Nacional de Estadística. Spanish National Health Survey. 2017. Available online: https://www.ine.es/dyngs/INEbase/en/operacion.htm?c=Estadistica_C&cid=1254736176783&menu=ultiDatos&idp=1254735573175 (accessed on 3 December 2020).
- World Health Organization. International Classification of Functioning, Disability and Health: ICF; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Mañas, E.; Rivera, L.F.; Gallo, M.T.; Montes, O.; Figueroa, C.; Castellano, M.; Prieto, P. El Impacto de la Violencia de Género en España: Una Valoración de sus Costes en 2016; Delegación de Gobierno para la Violencia de Género, Ministerio de la Presidencia, Relaciones con las Cortes e Igualdad, Centro de publicaciones: Madrid, Spain, 2019; Available online: https://violenciagenero.igualdad.gob.es/violenciaEnCifras/estudios/investigaciones/2019/pdfs/El_impacto_de_la_VG_ES.pdf (accessed on 14 January 2021).
- Vela, E.; Clèries, M.; Vella, V.A.; Adroher, C.; García-Altés, A. Análisis poblacional del gasto en servicios sanitarios en Cataluña (España): ¿qué y quién consume más recursos? Gac. Sanit. 2017, 33, 24–31. [Google Scholar] [CrossRef]
- Ten, C. Impacto del Equipamiento en el Coste del área de Imagen Médica del Hospital Universitario y Politécnico La Fe (Valencia). Master’s Thesis, Universitat Politècnica de València, Valencia, 18 July 2013. Available online: https://riunet.upv.es/bitstream/handle/10251/34711/TFM-CARLOTA%20TEN%20ROLDAN.pdf?sequence=1&isAllowed=y (accessed on 14 January 2021).
- Sociedad Española de Ultrasonidos (SEUS). Los Costes de la Ecografía, Documento SEUS 1-2012; Sociedad Española de Radiología Médica: Madrid, Spain, 2012; Available online: https://www.seram.es/images/site/seus-sociedad-española-de-ultrasonidos.original.pdf (accessed on 14 January 2021).
- Olivas, M. Resonancias magnéticas. Una oportunidad de ahorro. Auditoría operativa de la gestión del concierto de resonancias magnéticas en la Comunitat Valenciana. Audit. Pública 2014, 63, 11–20. [Google Scholar]
- De la Revilla, L.; Bailón, E.; Luna, J.D.; Delgado, A.; Prados, M.A.; Fleitas, L. Validación de una escala de apoyo social funcional para su uso en la consulta del médico de familia. Atención Primaria 1991, 8, 688–692. [Google Scholar]
- Cuéllar-Flores, I.; Dresch, V. Validación del cuestionario de Apoyo Social Funcional Duke-UNK-11 en personas cuidadoras. Rev. Iberoam. De Diagnóstico Y Evaluación-E Avaliaçao Psicológica 2012, 34, 89–101. [Google Scholar]
- López, M.J.; Orueta, R.; Gómez-Caro, S.; Sánchez, A.; Carmona, J.; Alonso, F.J. El rol de Cuidador de personas dependientes y sus repercusiones sobre su Calidad de Vida y su Salud. Rev. Clínica De Med. De Fam. 2009, 2, 332–339. [Google Scholar] [CrossRef] [Green Version]
- Pérez, A.; García, L.; Rodríguez, E.; Losada, A.; Porras, N.; Gómez, M.A. Función familiar y salud mental del ciudador de familiares con dependencia. Atención Primaria 2009, 41, 621–628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masanet, E.; La Parra, D. Relación entre el número de horas de cuidado informal y el estado de salud mental de las personas cuidadoras. Rev. Española De Salud Pública 2011, 85, 257–266. [Google Scholar] [CrossRef] [Green Version]
- Rivas-Diez, R. Apoyo Social Funcional en mujeres de la población general y en mujeres maltratadas chilenas. Propiedades psicométricas del Duke-UNC-11. Rev. Iberoam. De Diagnóstico Y Evaluación-E Avaliaçao Psicológica 2013, 36, 9–27. [Google Scholar]
- González, D.; Ducca, L.V.; García, C. La incidencia del apoyo social comunitario en la calidad de vida de personas con discapacidad. Siglo Cero 2020, 51, 83–103. [Google Scholar] [CrossRef]
- World Bank; World Health Organization. The World Report on Disability. 2011. Available online: http://www.who.int/disabilities/world_report/2011/en/ (accessed on 21 January 2018).
- Banks, L.M.; Kuper, H.; Polack, S. Poverty and disability in low- and middle-income countries: A systematic review. PLoS ONE 2017, 12, e0189996. [Google Scholar] [CrossRef] [Green Version]
- Kuper, H.; Monteath-van Dok, A.; Wing, K.; Danquah, L.; Evans, J.; Zuurmond, M.; Gallinetti, J. The Impact of Disability on the Lives of Children; Cross-Sectional Data Including 8900 Children with Disabilities and 898,834 Children without Disabilities across 30 Countries. PLoS ONE 2014, 9, e107300. [Google Scholar] [CrossRef] [PubMed]
- Ng, M.; Fullman, N.; Dieleman, J.L.; Flaxman, A.D.; Murray, C.J.L.; Lim, S.S. Effective Coverage: A Metric for Monitoring Universal Health Coverage. PLoS Med. 2014, 11, e1001730. [Google Scholar] [CrossRef]
- Bright, T.; Kuper, H. A Systematic Review of Access to General Healthcare Services for People with Disabilities in Low and Middle Income Countries. Int. J. Environ. Res. Public Health 2018, 15, 1879. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hawe, P.; Shiell, A. Social capital and health promotion: A review. Soc. Sci. Med. 2000, 51, 871–885. [Google Scholar] [CrossRef]
- Sakellariou, D.; Rotarou, E.S. Access to healthcare for men and women with disabilities in the UK: Secondary analysis of cross-sectional data. BMJ Open 2017, 7, e016614. [Google Scholar] [CrossRef] [PubMed]
- Ashe, S.; Duvvury, N.; Raghavendra, S.; Scriver, S.; O’Donovan, D. Methodological Approaches for Estimating the Economic Costs of Violence Against Women and Girls. What Works to Prevent Violence Against Women and Girls Programme. 2017. Available online: https://www.whatworks.co.za/documents/publications/90-methodological-approaches-for-estimating-the-economic-costs-of-vawg/file (accessed on 14 January 2021).
- Duvvury, N.; Callan, A.; Carney, P.; Raghavendra, S. Women’s Voice, Agency, and Participation Research Series; The Workd Bank: Washington, DC, USA, 2013; Available online: https://openknowledge.worldbank.org/handle/10986/16697 (accessed on 14 January 2021).
- Hoddenbagh, J.; Zhang, T.; McDonald, S. An Estimation of the Economic Impact of Violent Victimization in Canada, 2009; Research and Statistical Division, Department of Justice: Ottawa, ON, Canada, 2014.


{kind=link}
| Age | Count | Frequency |
| From 15 to 29 years old | 3,371,139 | 16.81% |
| From 30 to 49 years old | 7,073,835 | 35.28% |
| From 50 to 64 years old | 4,780,142 | 23.84% |
| From 65 to 80 years old | 3,359,199 | 16.75% |
| More than 80 years old | 1,466,441 | 7.30% |
| Perceived Health Status | Count | Frequency |
| Very Good | 3,854,482 | 19.22% |
| Good | 9,470,639 | 47.23% |
| Fair | 4,739,030 | 23.64% |
| Bad | 1,514,248 | 7.55% |
| Very bad | 472,358 | 2.36% |
| Global Activity Limitation Indicator | Count | Frequency |
| Severely limited | 1,069,577 | 5.34% |
| Limited, but not severely | 4,806,974 | 23.98% |
| Not limited | 14,170,396 | 70.68% |
| Healthcare Service | Unit Cost (UCi), € |
|---|---|
| Number of times the respondent has consulted a general practitioner or family doctor in the past four weeks | 46.98 |
| Number of times the respondent has consulted a specialist in the last four weeks | 120.05 |
| Number of times respondent has been hospitalized in the past twelve months, excluding childbirth or caesarean sections | 8906.55 |
| Admission to a day hospital over the past twelve months for intervention, treatment, or to have a test done | 173.39 |
| Use of any emergency service in the past twelve months | 182.68 |
| Use of other services over the past 12 months: Physiotherapist over the past twelve months | 24.01 |
| Use of other services over the past 12 months: Psychologist, Psychotherapist or Psychiatrist | 100.21 |
| Use of other services over the past 12 months: Nurse or Midwife | 24.01 |
| Diagnostic tests carried out in the past 12 months: X-ray | 20.70 |
| Diagnostic tests carried out in the past 12 months: CAT scan | 37.12 |
| Diagnostic tests carried out in the past 12 months: Ultrasound | 26.06 |
| Diagnostic tests carried out in the past 12 months: MRI | 112.32 |
| Emotional and Personal Support Items | First P.C. | Second P.C. |
|---|---|---|
| EPS-01: Visits with friends and relatives | 0.220 | 0.744 |
| EPS-02: Help around the house | 0.184 | 0.791 |
| EPS-03: Praise and recognition for a good job | 0.249 | 0.723 |
| EPS-04: I have people who care what happens to me | 0.712 | 0.336 |
| EPS-05: I get love and affection | 0.719 | 0.287 |
| EPS-06: I get chances to talk to someone about problems at work or with my housework | 0.893 | 0.165 |
| EPS-07: I get chances to talk to someone I trust about my personal or family problems | 0.903 | 0.162 |
| EPS-08: I get chances to talk about money matters | 0.868 | 0.177 |
| EPS-09: I get invitations to go out and do things with other people | 0.595 | 0.421 |
| EPS-10: I get useful advice about important things in life | 0.757 | 0.316 |
| EPS-11: I get help when I am sick in bed | 0.677 | 0.308 |
| Global Activity Limitation Indicator | ||||
|---|---|---|---|---|
| Not Limited | Limited | |||
| Emotional and Personal Support | N | % | N | % |
| Below average EPS | 3,994,546 | 29.23 | 2,246,794 | 40.39 |
| Above average EPS | 9,672,982 | 70.77 | 3,315,579 | 59.61 |
| Healthcare Service (Si) | Not Limited | Limited | F-Statistics (p-Value) |
|---|---|---|---|
| Number of times the respondent has consulted a general practitioner or family doctor in the past four weeks | 0.36 | 0.78 | 1,007,809.37 (<0.001) |
| Number of times the respondent has consulted a specialist in the last four weeks | 0.25 | 0.51 | 347,495.36 (<0.001) |
| Number of times respondent has been hospitalized in the past twelve months, excluding childbirth or caesarean sections | 1.17 | 1.48 | 31,973.20 (<0.001) |
| Admission to a day hospital over the past twelve months for intervention, treatment, or to have a test done | 3.46 | 17.01 | 11,788.97 (<0.001) |
| Use of any emergency service in the past twelve months | 1.69 | 2.33 | 67,320.62 (<0.001) |
| Use of other services over the past 12 months: Physiotherapist over the past twelve months | 16.55% | 23.61% | 137,471.16 (<0.001) |
| Use of other services over the past 12 months: Psychologist, Psychotherapist or Psychiatrist | 4.14% | 12.08% | 441,789.20 (<0.001) |
| Use of other services over the past 12 months: Nurse or Midwife | 14.92% | 26.09% | 353,738.17 (<0.001) |
| Diagnostic tests carried out in the past 12 months: X-ray | 20.18% | 45.90% | 1,471,102.62 (<0.001) |
| Diagnostic tests carried out in the past 12 months: CAT scan | 5.06% | 17.75% | 870,652.06 (<0.001) |
| Diagnostic tests carried out in the past 12 months: Ultrasound | 19.31% | 26.88% | 141,287.46 (<0.001) |
| Diagnostic tests carried out in the past 12 months: MRI | 5.58% | 17.45% | 734,905.14 (<0.001) |
| Healthcare Service (Si) | Below Average EPS (NB) | Above Average EPS (NA) | F-Statistic (p-Value) |
|---|---|---|---|
| Number of times the respondent has consulted a general practitioner or family doctor in the past four weeks | 0.83 (2,158,411) | 0.75 (3,433,199) | 5343.93 (<0.001) |
| Number of times the respondent has consulted a specialist in the last four weeks | 0.51 (1,764,468) | 0.52 (2,969,236) | 646.46 (<0.001) |
| Number of times respondent has been hospitalized in the past twelve months, excluding childbirth or caesarean sections | 1.51 (385,449) | 1.45 (622,098) | 2452.11 (<0.001) |
| Admission to a day hospital over the past twelve months for intervention, treatment, or to have a test done | 19.48 (329,307) | 15.67 (609,365) | 151.09 (<0.001) |
| Use of any emergency service in the past twelve months | 2.46 (1,047,554) | 2.25 (1,704,129) | 955.13 (<0.001) |
| Use of other services over the past 12 months: Physiotherapist over the past twelve months | 20.07% (2,245,468) | 25.79% (3,629,757) | 27,378.90 (<0.001) |
| Use of other services over the past 12 months: Psychologist, Psychotherapist or Psychiatrist | 13.45% (2,246,794) | 11.22% (3,627,255) | 8013.95 (<0.001) |
| Use of other services over the past 12 months: Nurse or Midwife | 19.87% (2,246,794) | 29.94% (3,621,446) | 69,686.00 (<0.001) |
| Diagnostic tests carried out in the past 12 months: X-ray | 45.10% (2,245,385) | 46.39% (3,624,818) | 1928.72 (<0.001) |
| Diagnostic tests carried out in the past 12 months: CAT scan | 18.05% (2,244,874) | 17.57% (3,619,857) | 118.09 (<0.001) |
| Diagnostic tests carried out in the past 12 months: Ultrasound | 26.09% (2,241,611) | 27.36% (3,629,405) | 3185.51 (<0.001) |
| Diagnostic tests carried out in the past 12 months: MRI | 14.32% (2,243,072) | 19.39% (3,602,544) | 32,314.80 (<0.001) |
| Healthcare Service (Si) | Ci (Million €) | ||
|---|---|---|---|
| Number of times the respondent has consulted a general practitioner or family doctor in the past four weeks | 205.28 | −8.12 | −3.95% |
| Number of times the respondent has consulted a specialist in the last four weeks | 292.56 | 2.73 | 0.93% |
| Number of times respondent has been hospitalized in the past twelve months, excluding childbirth or caesarean sections | 13,243.09 | −205.51 | −1.55% |
| Admission to a day hospital over the past twelve months for intervention, treatment, or to have a test done | 2768.44 | −217.41 | −7.85% |
| Use of any emergency service in the past twelve months | 1170.61 | −39.24 | −3.35% |
| Use of other services over the past 12 months: Physiotherapist over the past twelve months | 33.30 | 3.09 | 9.27% |
| Use of other services over the past 12 months: Psychologist, Psychotherapist or Psychiatrist | 71.09 | -5.02 | −7.05% |
| Use of other services over the past 12 months: Nurse or Midwife | 36.75 | 5.43 | 14.78% |
| Diagnostic tests carried out in the past 12 months: X-ray | 55.77 | 0.60 | 1.07% |
| Diagnostic tests carried out in the past 12 months: CAT scan | 38.64 | -0.40 | −1.04% |
| Diagnostic tests carried out in the past 12 months: Ultrasound | 41.06 | 0.74 | 1.80% |
| Diagnostic tests carried out in the past 12 months: MRI | 114.91 | 12.78 | 11.12% |
| ALL HEALTHCARE SERVICES | 18,071.49 | −450.32 | −2.49% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vargas-Vargas, M.; Meseguer-Santamaría, M.-L.; Sánchez-Alberola, F. Economic Evaluation of Emotional and Personal Support in the Health Care of Women with Disabilities. Healthcare 2021, 9, 438. https://doi.org/10.3390/healthcare9040438
Vargas-Vargas M, Meseguer-Santamaría M-L, Sánchez-Alberola F. Economic Evaluation of Emotional and Personal Support in the Health Care of Women with Disabilities. Healthcare. 2021; 9(4):438. https://doi.org/10.3390/healthcare9040438
Chicago/Turabian StyleVargas-Vargas, Manuel, María-Leticia Meseguer-Santamaría, and Francisco Sánchez-Alberola. 2021. "Economic Evaluation of Emotional and Personal Support in the Health Care of Women with Disabilities" Healthcare 9, no. 4: 438. https://doi.org/10.3390/healthcare9040438