
Influencing Factors of Acceptance and Use Behavior of Mobile Health Application Users: Systematic Review


Abstract
:1. Introduction
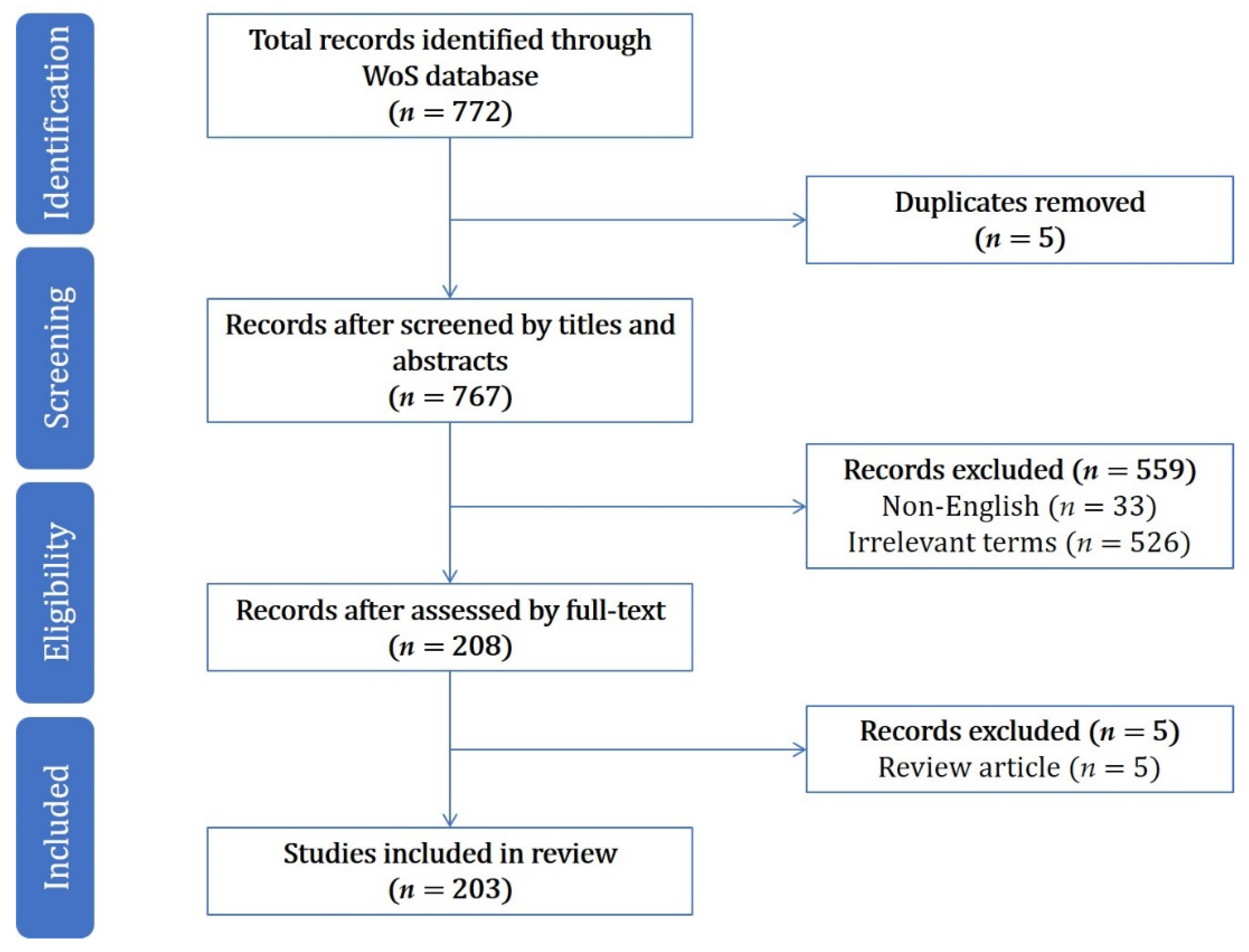
2. Materials and Methods
3. Results
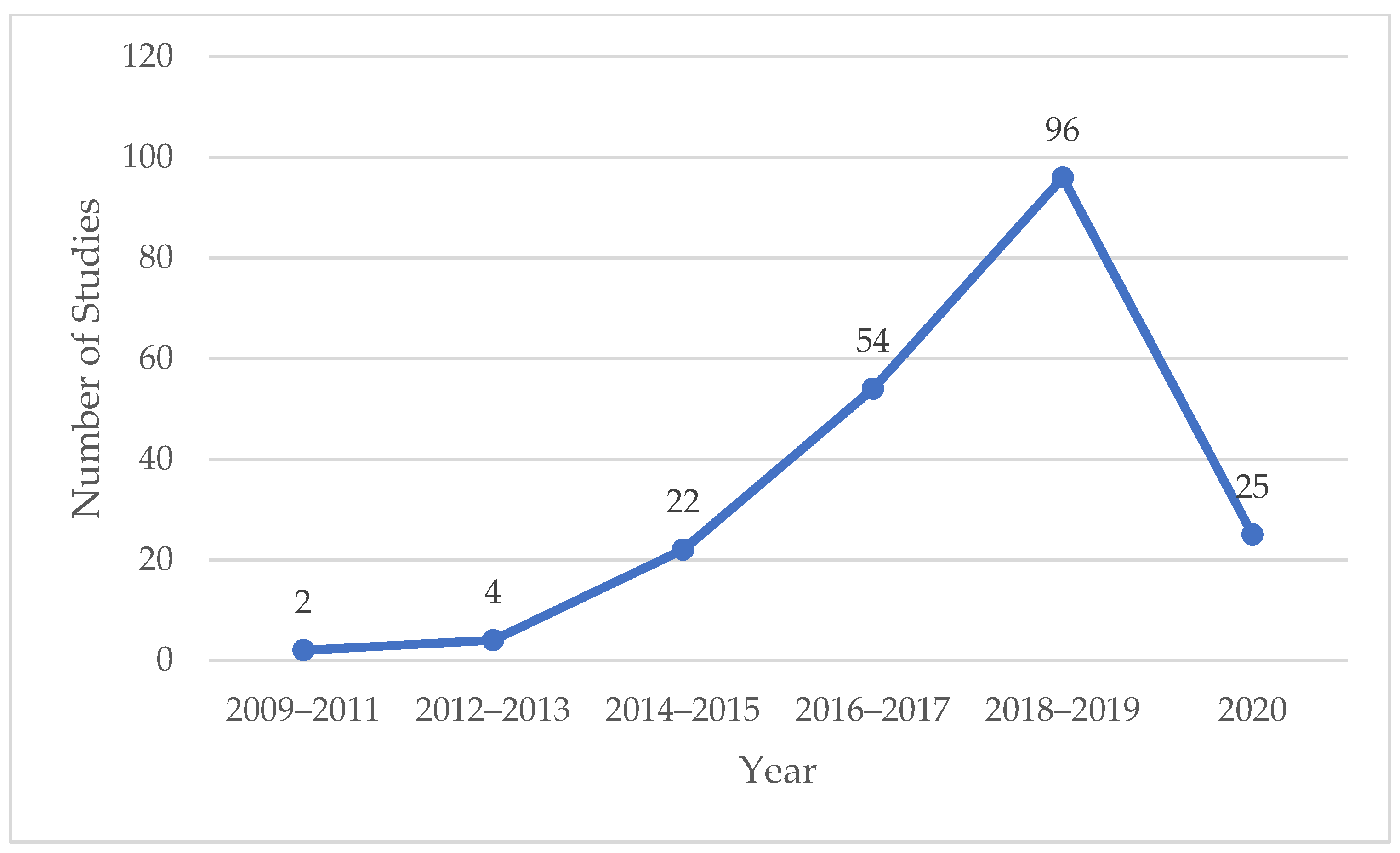
3.1. Year of Publication
3.2. Journal Distribution
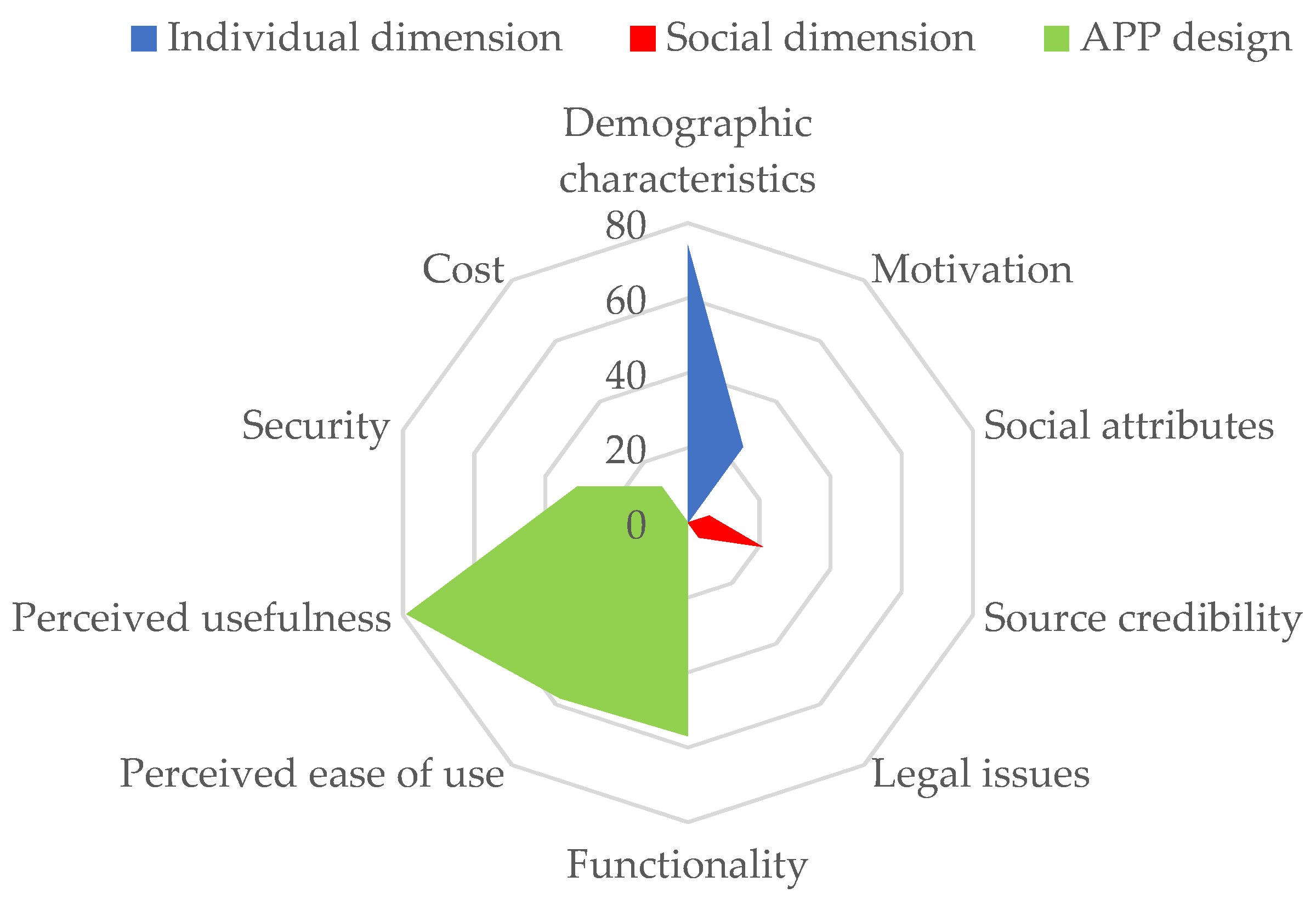
3.3. Influencing Factors in Acceptance and Use Behavior of Mobile Health Application Users
3.3.1. Individual Dimension
- Demographic characteristics.
- 2.
- Motivation.
3.3.2. Social Dimension
- Social attributes.
- 2.
- Source credibility.
- 3.
- Legal issues.
3.3.3. App Design
- Functionality.
- 2.
- Perceived ease of use and usefulness.
- 3.
- Security.
- 4.
- Cost.
4. Discussion
4.1. Considering the Demographic Factors That Affect Users’ Behavior
4.2. Strengthening the Publicity and System Management of Mobile Health Apps
4.3. Strengthening the Security and Privacy Measures of Mobile Health Apps
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Healthcare Mobile Application Market Size, Share & Trends Analysis Report By Type (Fitness Products Training, Appointment Booking & Construction), By Platform, By Technology, By End User, And Segment Forecasts, 2020–2027. Available online: https://www.grandviewresearch.com/industry-analysis/healthcare-mobile-applications-market (accessed on 7 September 2020).
- Bidargaddi, N.; Almirall, D.; Murphy, S.; Nahum-Shani, I.; Kovalcik, M.; Pituch, T.; Maaieh, H.; Strecher, V. To Prompt or Not to Prompt? A Microrandomized Trial of Time-Varying Push Notifications to Increase Proximal Engagement with a Mobile Health App. JMIR mHealth uHealth 2018, 6, e10123. [Google Scholar] [CrossRef]
- Cho, J.; Quinlan, M.M.; Park, D.; Noh, G.Y. Determinants of adoption of smartphone health apps among college students. Am. J. Health Behav. 2014, 38, 860–870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shen, C.; Wang, M.P.; Chu, J.T.; Wan, A.; Viswanath, K.; Chan, S.S.C.; Lam, T.H.W. Health App Possession Among Smartphone or Tablet Owners in Hong Kong: Population-Based Survey. JMIR mHealth uHealth 2017, 5, 21–34. [Google Scholar] [CrossRef] [Green Version]
- Ernsting, C.; Stuhmann, L.M.; Dombrowski, S.U.; Voigt-Antons, J.N.; Kuhlmey, A.; Gellert, P. Associations of Health App Use and Perceived Effectiveness in People with Cardiovascular Diseases and Diabetes: Population-Based Survey. JMIR mHealth uHealth 2019, 7, e12179. [Google Scholar] [CrossRef] [PubMed]
- Povey, J.; Mills, P.P.J.R.; Dingwall, K.M.; Lowell, A.; Singer, J.; Rotumah, D.; Bennett-Levy, J.; Nagel, T. Acceptability of Mental Health Apps for Aboriginal and Torres Strait Islander Australians: A Qualitative Study. J. Med. Internet Res. 2016, 18, e65. [Google Scholar] [CrossRef]
- Berkowitz, C.M.; Zullig, L.L.; Koontz, B.F.; Smith, S.K. Prescribing an App? Oncology Providers’ Views on Mobile Health Apps for Cancer Care. JCO Clin. Cancer Inform. 2017, 1, 1–7. [Google Scholar] [CrossRef]
- Biviji, R.; Vest, J.R.; Dixon, B.E.; Cullen, T.; Harle, C.A. Factors Related to User Ratings and User Downloads of Mobile Apps for Maternal and Infant Health: Cross-Sectional Study. JMIR mHealth uHealth 2020, 8, e15663. [Google Scholar] [CrossRef] [PubMed]
- Tuman, M.; Moyer, A. Health intentions and behaviors of health app owners: A cross-sectional study. Psychol. Health Med. 2019, 24, 819–826. [Google Scholar] [CrossRef]
- Zhou, L.; Bao, J.; Watzlaf, V.; Parmanto, B. Barriers to and Facilitators of the Use of Mobile Health Apps from a Security Perspective: Mixed-Methods Study. JMIR mHealth uHealth 2019, 7, e11223. [Google Scholar] [CrossRef] [PubMed]
- Najm, A.; Nikiphorou, E.; Kostine, M.; Richez, C.; Pauling, J.D.; Finckh, A.; Ritschl, V.; Prior, Y.; Balážová, P.; Stones, S.; et al. EULAR Points to Consider for The Development, Evaluation And Implementation Of Mobile Health Applications Aiding Self-Management In People Living With Rheumatic And Musculoskeletal Diseases. RMD Open 2019, 5, e001014. [Google Scholar] [CrossRef] [Green Version]
- Geuens, J.; Swinnen, T.W.; Westhovens, R.; de-Vlam, K.; Geurts, L.; Vanden-Abeele, V. A Review of Persuasive Principles in Mobile Apps for Chronic Arthritis Patients: Opportunities for Improvement. JMIR mHealth uHealth 2016, 4, e118. [Google Scholar] [CrossRef] [Green Version]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katz, J.E.; Rice, R.E. Public views of mobile medical devices and services: A US national survey of consumer sentiments towards RFID healthcare technology. Int. J. Med. Inform. 2009, 78, 104–114. [Google Scholar] [CrossRef] [PubMed]
- Reddy, R.; Majmudar, M.; Dhopeshwarkar, N.; Vacaro, V.; Isselbacher, E.; Bhatt, A.B. Mobile health apps preferences and practice among ambulatory cardiovascular patients. Future Cardiol. 2018, 14, 381–388. [Google Scholar] [CrossRef]
- Bhuyan, S.S.; Lu, N.; Chandak, A.; Kim, H.; Wyant, D.; Bhatt, J.; Kedia, S.; Chang, C.F. Use of Mobile Health Applications for Health-Seeking Behavior Among US Adults. J. Med. Syst. 2016, 40, 153. [Google Scholar] [CrossRef] [PubMed]
- James, D.C.S.; Harville, C. Barriers and Motivators to Participating in mHealth Research Among African American Men. Am. J. Mens Health 2015, 11, 1605–1613. [Google Scholar] [CrossRef]
- Crilly, P.; Jair, S.; Mahmood, Z.; Moin Khan, A.; Munir, A.; Osei-Bediako, I.; Samir, M.; Kayyali, R. Public views of different sources of health advice: Pharmacists, social media and mobile health applications. Int. J. Pharm. Pract. 2019, 27, 88–95. [Google Scholar] [CrossRef] [Green Version]
- Manierre, M.J. Gaps in knowledge: Tracking and explaining gender differences in health information seeking. Soc. Sci. Med. 2015, 128, 151–158. [Google Scholar] [CrossRef]
- Bol, N.; Helberger, N.; Weert, J.C.M. Differences in mobile health app use: A source of new digital inequalities? Inf. Soc. 2018, 34, 183–193. [Google Scholar] [CrossRef] [Green Version]
- Richman, A.R.; Webb, M.C.; Brinkley, J.; Martin, R.J. Sexual behaviour and interest in using a sexual health mobile app to help improve and manage college students’ sexual health. Sex Educ. Sex. Soc. Learn. 2014, 14, 310–322. [Google Scholar] [CrossRef]
- Krebs, P.; Duncan, D.T. Health App Use Among US Mobile Phone Owners: A National Survey. JMIR mHealth uHealth 2015, 3, e101. [Google Scholar] [CrossRef] [Green Version]
- Post, L.A.; Vaca, F.E.; Biroscak, B.J.; Dziura, J.; Brandt, C.; Bernstein, S.L.; Taylor, R.; Jagminas, L.; D’Onofrio, G. The Prevalence and Characteristics of Emergency Medicine Patient Use of New Media. JMIR mHealth uHealth 2015, 3, e72. [Google Scholar] [CrossRef] [PubMed]
- Laing, S.S.; Alsayid, M.; Ocampo, C.; Baugh, S. Mobile Health Technology Knowledge and Practices Among Patients of Safety-Net Health Systems in Washington State and Washington, DC. J. Patient Cent. Res. Rev. 2018, 5, 204–217. [Google Scholar] [CrossRef]
- Connolly, S.L.; Miller, C.J.; Koenig, C.J.; Zamora, K.A.; Wright, P.B.; Stanley, R.L.; Pyne, J.M. Veterans’ Attitudes Toward Smartphone App Use for Mental Health Care: Qualitative Study of Rurality and Age Differences. JMIR mHealth uHealth 2018, 6, e10748. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bender, M.S.; Choi, J.W.; Arai, S.; Paul, S.M.; Gonzalez, P.; Fukuoka, Y. Digital Technology Ownership, Usage, and Factors Predicting Downloading Health Apps Among Caucasian, Filipino, Korean, and Latino Americans: The Digital Link to Health Survey. JMIR mHealth uHealth 2014, 2, e43. [Google Scholar] [CrossRef] [PubMed]
- Deb, K.S.; Tuli, A.; Sood, M.; Chadda, R.; Verma, R.; Kumar, S.; Ganesh, R.; Singh, P. Is India ready for mental health apps (MHApps)? A quantitative-qualitative exploration of caregivers’ perspective on smartphone-based solutions for managing severe mental illnesses in low resource settings. PLoS ONE 2018, 13, e0203353. [Google Scholar]
- Robbins, R.; Krebs, P.; Jagannathan, R.; Jean-Louis, G.; Duncan, D.T. Health App Use Among US Mobile Phone Users: Analysis of Trends by Chronic Disease Status. JMIR mHealth uHealth 2017, 5, e197. [Google Scholar] [CrossRef]
- Cho, J.; Park, D.; Lee, H.E. Cognitive Factors of Using Health Apps: Systematic Analysis of Relationships Among Health Consciousness, Health Information Orientation, eHealth Literacy, and Health App Use Efficacy. J. Med. Internet Res. 2014, 16, 206–215. [Google Scholar] [CrossRef] [PubMed]
- Ernsting, C.; Dombrowski, S.U.; Oedekoven, M.; O’Sullivan, J.L.; Kanzler, M.; Kuhlmey, A.; Gellert, P. Using Smartphones and Health Apps to Change and Manage Health Behaviors: A Population-Based Survey. J. Med. Internet Res. 2017, 19, e101. [Google Scholar] [CrossRef]
- Chae, J. A Comprehensive Profile of Those Who Have Health-Related Apps. Health Educ. Behav. Off. Publ. Soc. Public Health Educ. 2018, 45, 591–598. [Google Scholar] [CrossRef]
- Milward, J.; Deluca, P.; Drummond, C.; Kimergård, A. Developing Typologies of User Engagement with the BRANCH Alcohol-Harm Reduction Smartphone App: Qualitative Study. JMIR mHealth uHealth 2018, 6, e11692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tran, B.X.; Zhang, M.W.B.; Le, H.T.; Nguyen, H.D.; Nguyen, L.H.; Nguyen, Q.L.T.; Tran, T.D.; Latkin, C.A.; Ho, R.C. What drives young Vietnamese to use mobile-health innovations? Implications for health communication and behavioral interventions. JMIR mHealth uHealth 2018, 6, e194. [Google Scholar] [CrossRef] [PubMed]
- Dutta-Bergman, M.J. Primary sources of health information: Comparisons in the domain of health attitudes, health cognitions, and health behaviors. Health Commun. 2004, 16, 273–288. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.; Lee, H.E.; Quinlan, M. Complementary Relationships Between Traditional Media and Health Apps Among American College Students. J. Am. Coll. Health 2015, 63, 248–257. [Google Scholar] [CrossRef] [PubMed]
- Collado-Borrell, R.; Escudero-Vilaplana, V.; Calles, A.; Garcia-Martin, E.; Marzal-Alfaro, B.; Gonzalez-Haba, E.; Herranz-Alonso, A.; Sanjurjo-Saez, M. Oncology Patient Interest in the Use of New Technologies to Manage Their Disease: Cross-Sectional Survey. J. Med. Internet Res. 2018, 20, e11006. [Google Scholar] [CrossRef]
- Shemesh, T.; Barnoy, S. Assessment of the Intention to Use Mobile Health Applications Using a Technology Acceptance Model in an Israeli Adult Population. Telemed. E-Health 2020, 26, 1141–1149. [Google Scholar] [CrossRef] [PubMed]
- Pierce, B.; Twohig, M.; Levin, M.E. Perspectives on the use of acceptance and commitment therapy related mobile apps: Results from a survey of students and professionals. J. Contextual Behav. Sci. 2016, 5, 215–224. [Google Scholar] [CrossRef] [Green Version]
- Saberi, P.; Siedle-Khan, R.; Sheon, N.; Lightfoot, M. The Use of Mobile Health Applications Among Youth and Young Adults Living with HIV: Focus Group Findings. AIDS Patient Care STDs 2016, 30, 254–260. [Google Scholar] [CrossRef] [Green Version]
- Günczler, M. “Is There an App for That?” Orthopaedic Patient Preferences for A Smartphone Application. Appl. Clin. Inform. 2017, 8, 832–844. [Google Scholar]
- Peng, W.; Kanthawala, S.; Yuan, S.; Hussain, S.A. A qualitative study of user perceptions of mobile health apps. BMC Public Health 2016, 16, 1158. [Google Scholar] [CrossRef] [Green Version]
- Mendiola, M.F.; Kalnicki, M.; Lindenauer, S. Valuable Features in Mobile Health Apps for Patients and Consumers: Content Analysis of Apps and User Ratings. JMIR mHealth uHealth 2015, 3, e40. [Google Scholar] [CrossRef]
- Hilliard, M.E.; Hahn, A.; Ridge, A.K.; Eakin, M.N.; Riekert, K.A. User Preferences and Design Recommendations for an mHealth App to Promote Cystic Fibrosis Self-Management. JMIR mHealth uHealth 2014, 2, e44. [Google Scholar] [CrossRef] [PubMed]
- Ramanathan, N.; Swendeman, D.; Comulada, W.S.; Estrin, D.; Rotheram-Borus, M.J. Identifying preferences for mobile health applications for self-monitoring and self-management: Focus group findings from HIV-positive persons and young mothers. Int. J. Med. Inform. 2013, 82, e38–e46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maturo, A.; Setiffi, F. The gamification of risk: How health apps foster self-confidence and why this is not enough. Health Risk Soc. 2016, 17, 477–494. [Google Scholar] [CrossRef]
- Whitson, J.R. Gaming the Quantified Self. Surveill. Soc. 2013, 11, 163–176. [Google Scholar] [CrossRef]
- Zaidan, S.; Roehrer, E. Popular Mobile Phone Apps for Diet and Weight Loss: A Content Analysis. JMIR mHealth uHealth 2016, 4, e80. [Google Scholar] [CrossRef]
- Han, K.J.; Subramanian, R.; Cameron, G.T. Listen before you leap: Sri Lankan health professionals’ perspectives on m-health. Health Inform. J. 2017, 25, 858–866. [Google Scholar] [CrossRef]
- Chen, Y.; Yang, L.; Zhang, M.; Yang, J. Central or Peripheral? Cognition Elaboration Cues’ Effect on Users’ Continuance Intention of Mobile Health Applications in the Developing Markets. Int. J. Med. Inform. 2018, 116, 33–45. [Google Scholar] [CrossRef]
- Vaghefi, I.; Tulu, B. The Continued Use of Mobile Health Apps: Insights from a Longitudinal Study. JMIR mHealth uHealth 2019, 7, e12983. [Google Scholar] [CrossRef] [Green Version]
- Morey, S.A.; Stuck, R.E.; Chong, A.W.; Barg-Walkow, L.H.; Mitzner, T.L.; Rogers, W.A. Mobile Health Apps: Improving Usability for Older Adult Users. Ergon. Des. 2019, 27, 4–13. [Google Scholar] [CrossRef]
- Ledderer, L.; Mller, A.; Fage-Butler, A. Adolescents’ participation in their healthcare: A sociomaterial investigation of a diabetes app. Digit. Health 2019, 5. [Google Scholar] [CrossRef]
- Anastasiadou, D.; Folkvord, F.; Serrano-Troncoso, E.; Lupiañez-Villanueva, F. Mobile Health Adoption in Mental Health: User Experience of a Mobile Health App for Patients with an Eating Disorder. JMIR mHealth uHealth 2019, 7, e12920. [Google Scholar] [CrossRef] [Green Version]
- Knoble, S.J.; Bhusal, M.R. Electronic diagnostic algorithms to assist mid-level health care workers in Nepal: A mixed-method exploratory study. Int. J. Med. Inform. 2015, 84, 334–340. [Google Scholar] [CrossRef]
- Matteo, D.D.; Fine, A.; Fotinos, K.; Rose, J. Patient Willingness to Consent to Mobile Phone Data Collection for Mental Health Apps: Structured Questionnaire. JMIR Ment. Health 2018, 5, e56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kenny, R.; Dooley, B.; Fitzgerald, A. Developing mental health mobile apps: Exploring adolescents’ perspectives. Health Inform. J. 2016, 22, 265–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenfeld, L.; Torous, J.; Vahia, I.V. Data Security and Privacy in Apps for Dementia: An Analysis of Existing Privacy Policies. Am. J. Geriatr. Psychiatry 2017, 25, 873–877. [Google Scholar] [CrossRef]
- Alaiad, A.; Alsharo, M.; Alnsour, Y. The Determinants of M-Health Adoption in Developing Countries: An Empirical Investigation. Appl. Clin. Inform. 2019, 10, 820–840. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Journals | Number of Studies | Journal Fields | Start Publishing Papers |
|---|---|---|---|
| JMIR mHealth and uHealth | 7 | Health Care Sciences & Services | 2014 |
| International Journal of Medical Informatics | 6 | Health Care Sciences & Services, Medical Informatics, Computer Science | 2009 |
| Journal of Medical Internet Research | 5 | Health Care Sciences & Services, Medical Informatics | 2014 |
| BMC Medical Informatics and Decision Making | 4 | Medical Informatics | 2013 |
| PLOS One | 4 | Comprehensive | 2016 |
| Telemedicine and E-Health | 3 | Health Care Sciences & Services | 2015 |
| Health Informatics Journal | 3 | Health Care Sciences & Services | 2016 |
| Digital Health | 3 | Health Care Sciences & Services | 2018 |
| Journal of Cancer Education | 3 | Medicine Education | 2018 |
| Influencing Factor (Number of Related Papers) | Related Variable | Main Conclusion | Literature |
|---|---|---|---|
| Demographic characteristics (74) | Age | Mobile health applications are mainly used by the young, while seniors, especially those aged over 70, seldom adopt or use mobile health applications | [15,16,17,18] |
| Gender | Males prefer fitness applications, while females prefer applications related to nutrition, self-healthcare, and reproduction | [19,20,21] | |
| Education level | Populations with a high education level tend to use mobile health applications | [22] | |
| Income | Income levels are positively correlated with the use of mobile health applications | [4,23,24] | |
| Medical insurance | Populations with a high medical insurance level have a stronger tendency to use mobile health applications | [16] | |
| Region | Compared to urban residents, rural ones are not likely to use mobile health applications | [16,25] | |
| Ethnicity and language | Difficulties in searching and understanding health information for non-native speakers may restrict their acceptance and use | [26,27] | |
| Health condition | Those with a lower self-rated health status are less likely to use mobile health applications; a chronic history is associated with use | [4,28] | |
| Motivation (25) | Health awareness | Populations with higher health awareness have a higher acceptance level of mobile health applications | [9,29,30,31,32] |
| E-health literacy | E-health literacy is considered as a prerequisite of using mobile health applications | [5,20,29] |
| Influencing Factor (Number of Related Papers) | Related Variable | Main Conclusion | Literature |
|---|---|---|---|
| Social attributes (6) | Sharing/social network | Social networking increases interests and a sense of achievement and promotes users’ staying power | [33] |
| Source credibility (21) | Media publicity | Perceived credibility of traditional mass media has a positive correlation with the cognition of mobile health applications | [34,35] |
| Recommendation of professionals | As an important source of medical information, healthcare professionals’ recommendations may influence users’ behavior | [36] | |
| Support from healthcare organization | Support from healthcare institutions may enhance the credibility of mobile health applications | [37] | |
| Legal issues (5) | Legal supervision | Lack of legal supervision decreases the users’ trust of mobile health applications | [38] |
| Influencing Factor (Number of Related Papers) | Related Variable | Main Conclusion | Literature |
|---|---|---|---|
| Functionality (57) | Quality of information | Accuracy, timeliness, and relevance positively affect users’ trust in mobile health applications | [8,39,40] |
| Core function | Users are interested in core functions such as reminders, notifications, encouragement, follow-up, and goal setting, as well as in the way they are provided | [2,41,42] | |
| Personalization | Personalization is a key characteristic that enhances the attractiveness and acceptability of mobile health applications | [42,43,44] | |
| Game-based | Gamification provides an emotional support for maintaining motivations | [45,46] | |
| Perceived ease of use (58) | User interface design | A clean and simple interface can help users better interact with applications | [50,51] |
| Efficiency | The enormous amount of energy and time consumed is a hindrance to users’ acceptance and use | [6,50,52,53,54] | |
| Perceived usefulness (79) | Perceived usefulness | This includes information quality, core functions, personalization, and social attributes | [2,8,33,39,40,41,42,43,44] |
| Security (31) | Security and privacy | Users’ concern about the security and privacy of health data is one of the reasons they do not use or do not continuously use mobile health applications | [10,55,56,57,58] |
| Cost (12) | Cost | Some users are not willing to pay for mobile health applications | [10,22] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, C.; Qi, H. Influencing Factors of Acceptance and Use Behavior of Mobile Health Application Users: Systematic Review. Healthcare 2021, 9, 357. https://doi.org/10.3390/healthcare9030357
Wang C, Qi H. Influencing Factors of Acceptance and Use Behavior of Mobile Health Application Users: Systematic Review. Healthcare. 2021; 9(3):357. https://doi.org/10.3390/healthcare9030357
Chicago/Turabian StyleWang, Chen, and Huiying Qi. 2021. "Influencing Factors of Acceptance and Use Behavior of Mobile Health Application Users: Systematic Review" Healthcare 9, no. 3: 357. https://doi.org/10.3390/healthcare9030357