
Effects of Tooth Brushing Training, Based on Augmented Reality Using a Smart Toothbrush, on Oral Hygiene Care among People with Intellectual Disability in Korea


Abstract
:1. Introduction
2. Materials and Methods
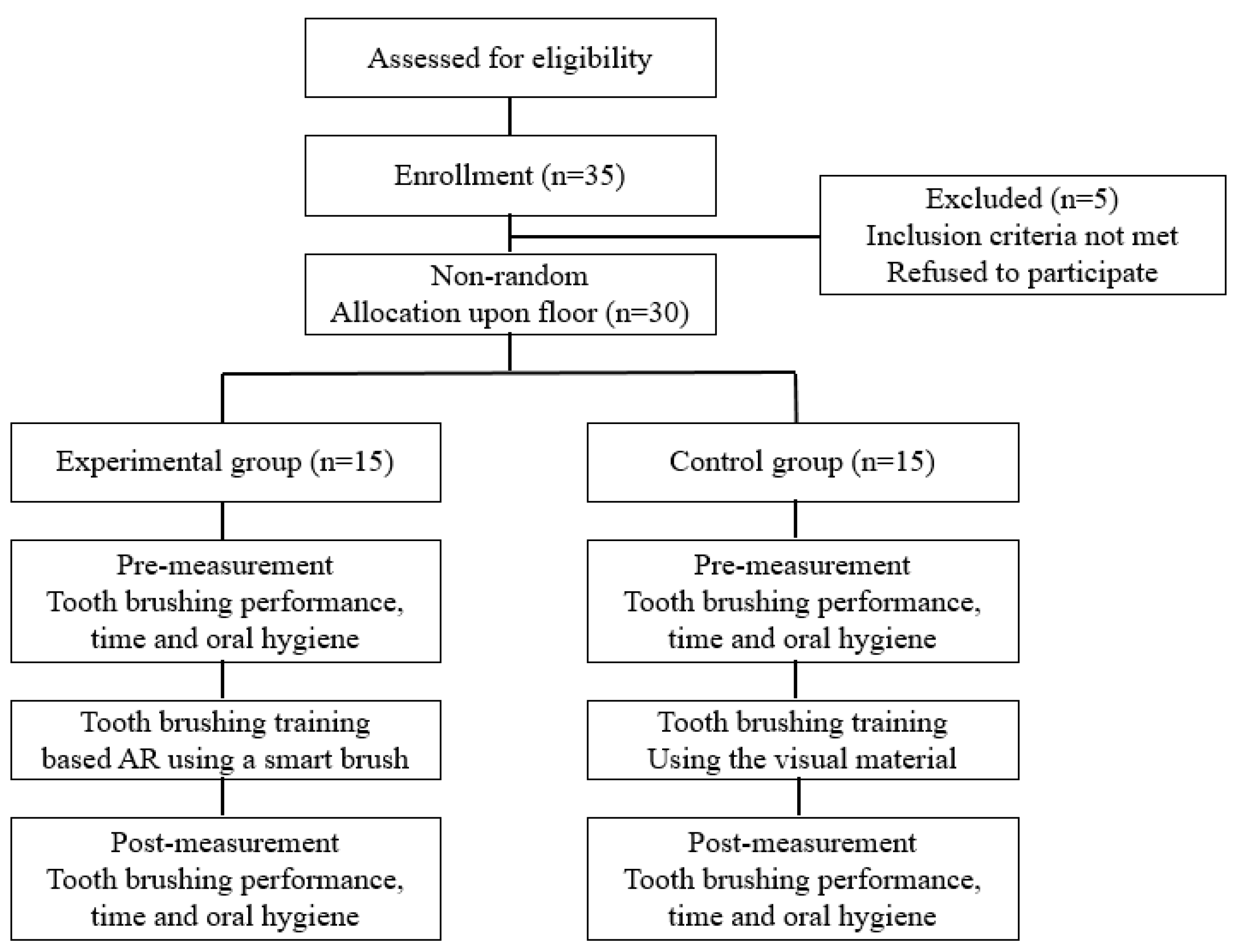
2.1. Study Subjects
2.2. Tooth-Brushing Training Based on the AR Using Smart Toothbrush
2.3. Tooth-Brushing Training Using Visual Material
2.4. Measures
2.4.1. Tooth-Brushing Performance Assessment
2.4.2. Oral Hygiene Assessment
2.5. Statistical Analysis
3. Results
3.1. Characteristics of Subjects
3.2. Results of Tooth-Brushing Performance
3.3. Results of Oral Hygiene
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Papagiannopoulou, V.; Oulis, C.J.; Papaioannou, W.; Antonogeorgos, G.; Yfantopoulos, J. Validation of a Greek version of the oral health impact profile 14 ((OHIP-14) for using among adults. Health Qual. Life Outcomes 2012, 10, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Gerritsen, A.E.; Allen, P.F.; Witter, D.J.; Bronkhorst, E.M.; Creugers, N.H. Tooth loss and oral health-related quality of life: A systematic review and meta-analysis. Health Qual. Life Outcomes 2010, 8, 126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panchbhai, A.S. Oral health care needs in the dependent elderly in India. Indian J. Palliat. Care 2012, 8, 19–26. [Google Scholar] [CrossRef]
- Howell, R.; Brimble, M. Dental health management for children with special healthcare needs. Nurs. Child. Young People 2013, 25, 19–22. [Google Scholar] [CrossRef]
- Addy, M.; Hunter, M. Can tooth brushing damage your health?: Effects on oral and dental tissues. Int. Dent. J. 2003, 53, 177–186. [Google Scholar]
- Ottley, C. Improving children’s dental health. J. Fam. Health Care 2002, 12, 122–125. [Google Scholar]
- Altun, C.; Guven, G.; Akgun, O.M.; Akkurt, M.D.; Basak, F.; Akbulut, E. Oral health status of disabled individuals attending special schools. Eur. J. Dent. 2010, 4, 361–366. [Google Scholar] [PubMed]
- Faria, A.L.; Andrade, A.; Soares, L.; Badia, S.B. Benefits of virtual reality based cognitive rehabilitation through simulated activities of daily living: A randomized controlled trial with stroke patients. J. Neuroeng. Rehabil. 2016, 13, 96. [Google Scholar] [CrossRef] [Green Version]
- Tolvanen, M.; Lahti, S.; Hausen, H. Changes in tooth brushing frequency in relation to changes in oral health-related knowledge and attitudes among children: A longitudinal study. Eur. J. Oral Sci. 2010, 118, 284–289. [Google Scholar] [CrossRef]
- de Castilho, A.R.F.; Mialhe, F.L.; de Souze Barbosa, T.; Puppin-Rontani, R.M. Influence of family environment on children’s oral health: A systemic review. J. Pediatr. 2013, 89, 116–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolawole, K.A.; Oziegbe, E.O.; Bamise, C.T. Oral hygiene measures and the periodontal status of school children. Int. J. Dent. Hyg. 2011, 9, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Laver, K.; George, S.; Thomas, S.; Deutsch, J.E.; Crotty, M. Virtual reality for stroke rehabilitation. Stroke 2012, 43, e20–e21. [Google Scholar] [CrossRef]
- Kim, K.S.; Yoon, T.H.; Lee, J.W.; Kim, D.J. Interactive tooth brushing education by a smart toothbrush system via 3D visualization. Comput. Methods Programs Biomed. 2009, 96, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Optale, G.; Urgesi, C.; Busato, V.; Marin, S.; Piron, L.; Oriftis, K.; Gamberini, L.; Capodieci, S.; Bordin, A. Controlling memory impairment in elderly adults using virtual reality memory training: A randomized controlled pilot study. Neurorehabil. Neural Repair 2010, 24, 348–357. [Google Scholar] [CrossRef]
- Yip, B.C.; Man, D.W. Virtual reality-based prospective memory training program for people with acquired brain injury. Neurorehabilitation 2013, 32, 103–115. [Google Scholar] [CrossRef] [PubMed]
- Gamito, P.; Oliveira, J.; Coelho, C.; Morais, D.; Lopes, P.; Pacheco, J.; Brito, R.; Soares, F.; Santos, N.; Barata, A.F. Cognitive training on stroke patients via virtual reality-based serious games. Disabil. Rehabil. 2017, 39, 385–388. [Google Scholar] [CrossRef] [PubMed]
- Navarro, M.D.; Lloréns, R.; Noé, E.; Ferri, J.; Alcañiz, M. Validation of a low-cost virtual reality system for training street-crossing: A comparative study in healthy, neglected and non-neglected stroke individuals. Neuropsychol. Rehabil. 2013, 23, 597–618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, L.; Abreu, B.C.; Seale, G.S.; Masel, B.; Christiansen, C.H.; Ottenbacher, K.J. A virtual reality environment for evaluation of a daily living skill in brain injury rehabilitation: Reliability and validity. Arch. Phys. Med. Rehabil. 2003, 84, 1118–1124. [Google Scholar] [CrossRef]
- Graetz, C.; Bielfeldt, J.; Wolff, L.; Springer, C.; EI-Sayed, K.M.F.; Salzer, S.; Badri-Hoher, S.; Dorfer, C.E. Tooth brushing education via a smart software visualization system. J. Periodontol. 2013, 84, 186–195. [Google Scholar] [CrossRef]
- Han, C.; Jo, S.A.; Jo, I.; Kim, E.; Park, M.H.; Kang, Y. An adaptation of the Korean mini-mental state examination (K-MMSE) in elderly Koreans: Demographic influence and population-based norms (the AGE study). Arch. Gerontol. Geriatr. 2008, 47, 302–310. [Google Scholar] [CrossRef]
- Kitten Planet. Brush Monster User Guide; Kitten Planaet, Co.: Seoul, Korea, 2018. [Google Scholar]
- Kim, N.Y.; Lee, S.Y. Effect of oral health education with Q-Scan in Preschool children. J. Dent. Hyg. Sci. 2015, 15, 696–702. [Google Scholar] [CrossRef] [Green Version]
- Korpela, J.; Miyaji, R.; Maekawa, T.; Nozaki, K.; Tamagawa, H. Evaluating tooth brushing performance with smartphone sound data. In Proceedings of the 2015 ACM International Joint Conference on Pervasive and Ubiquitous Computing, Osaka, Japan, 7–11 September 2015; pp. 109–120. [Google Scholar]
- Hong, I.; Woo, H.S.; Shim, S.; Li, C.Y.; Yoonjeong, L.; Velozo, C.A. Equating activities of daily living outcome measures: The functional independence measure and the Korean version of Modified Barthel Index. Disabil. Rehabil. 2018, 40, 217–224. [Google Scholar] [CrossRef]
- Mashima, I.; Theodorea, C.F.; Thaweboon, B.; Thaweboon, S.; Scannapieco, F.A.; Nakazawa, F. Exploring the salivary microbiome of children stratified by the oral hygiene index. PLoS ONE 2017, 12, e185274. [Google Scholar] [CrossRef]
- Arowojolu, M.O.; Fawole, O.I.; Dosumu, E.B.; Opeodu, O.I. A comparative study of the oral hygiene status of smoker and non-smokers in Ibadan, Oyo state. Niger. Med. J. J. Niger. Med. Assoc. 2013, 54, 240. [Google Scholar]
- Li, X.; Kolltveit, K.M.; Tronstad, L.; Olsen, I. Systemic diseases caused by oral infection. Clin. Microbiol. Rev. 2000, 13, 547–558. [Google Scholar] [CrossRef]
- Watt, R.; Fuller, S.; Harnett, R.; Treasure, E.; Stillman-Lowe, C. Oral health promotion evaluation–time for development. Community Dent. Oral Epidemiol. 2001, 29, 161–166. [Google Scholar] [CrossRef]
- Hachisu, T.; Kajimoto, H. Augmentation of Toothbrush by Modulating Sounds Resulting from Brushing; Springer: Berlin, Germany, 2012. [Google Scholar]
- Östberg, A.L. Adolescents’ views of oral health education: A qualitative study. Acta Odontol. Scand. 2005, 63, 300–307. [Google Scholar] [CrossRef] [PubMed]
- Flagg, A.; Boger, J.; Mihailidis, A. An intelligent toothbrush: Machines for smart brushing. In Proceedings of the RESNA/ICTA Meeting: Advancing Rehabilitation Technologies for an Aging Society, Toronto, Canada, 5–8 June 2011; pp. 1–4. [Google Scholar]
- Bacca Acosta, J.L.; Baldiris Navarro, S.M.; Fabregat Gesa, R.; Graf, S. Augmented reality trends in education: A systematic review of research and applications. J. Educ. Technol. Soc. 2014, 17, 133–149. [Google Scholar]
- Källestål, C.; Dahlgren, L.; Stenlund, H. Oral health behavior and self-esteem in Swedish adolescents over four years. J. Adolesc. Health 2006, 38, 583–590. [Google Scholar] [CrossRef]
- Geurs, N.C. Osteoporosis and periodontal disease. Periodontology 2000 2007, 44, 29–43. [Google Scholar] [CrossRef]


{kind=link}
| Activities | Dependent | Maximal Assist | Partial Assist | Minimal Assist | Independent | Time | Cronbach’sAlpha | ||
|---|---|---|---|---|---|---|---|---|---|
| Performance of teeth brushing | Outer surface | Front teeth | 0.919 | ||||||
| Back teeth | |||||||||
| Inner surface | Front teeth | 0.961 | |||||||
| Back teeth | |||||||||
| Total scores | /20 points | /s | |||||||
| Characteristics | Experimental Group | Control Group | U | Z | p-Value | |
|---|---|---|---|---|---|---|
| Age (Mean ± S.D) | 45.33 ± 10.42 | 45.67 ± 10.34 | 106.50 | −0.250 | 0.806 | |
| Sex (n, %) | M | 7 (46.7) | 7 (46.7) | 50.00 | 0.000 | 1.000 |
| F | 8 (53.3) | 7 (53.3) | ||||
| Disability grade (n, %) | 2 | 10 (66.7) | 10 (66.7) | 50.00 | 0.000 | 1.000 |
| 3 | 5 (33.3) | 5 (33.3) | ||||
| Groups | Tooth Brushing | Pre (Mean ± S.D) | 1 Month after (Mean ± S.D) | 2 Month after (Mean ± S.D) | 3 Month after (Mean ± S.D) | Mean Difference | X2 | p-Value |
|---|---|---|---|---|---|---|---|---|
| Experimental group | Performance (points) | 12.27 ± 3.20 | 15.47 ± 2.64 | 17.20 ± 1.82 | 17.60 ± 1.84 | 5.33 | 34.756 | 0.000 *** |
| Time (sec) | 85.80 ± 9.73 | 89.67 ± 9.19 | 95.73 ± 9.52 | 101.13 ± 7.68 | 15.33 | 27.658 | 0.000 *** | |
| Control group | Performance (points) | 12.80 ± 3.69 | 12.40 ± 3.56 | 14.13 ± 2.88 | 12.73 ± 3.15 | −0.07 | 3.000 | 0.392 |
| Time (sec) | 84.07 ± 9.65 | 83.40 ± 9.92 | 87.47 ± 8.79 | 87.00 ± 8.49 | 2.93 | 3.857 | 0.277 |
| Test | Tooth Brushing | Experimental Group (Mean ± S.D) | Control Group (Mean ± S.D) | Mean Difference | Z | p-Value |
|---|---|---|---|---|---|---|
| Pre | Performance (points) | 12.27 ± 3.20 | 12.80 ± 3.69 | 0.53 | −0.815 | 0.461 |
| Time (sec) | 85.80 ± 9.73 | 84.07 ± 9.65 | −1.73 | −0.462 | 0.653 | |
| I Month after | Performance (points) | 15.47 ± 2.64 | 12.40 ± 3.56 | −3.07 | −2.727 | 0.007 ** |
| Time (sec) | 89.67 ± 9.19 | 83.40 ± 9.92 | −6.27 | −3.238 | 0.001 ** | |
| 2 Month after | Performance (points) | 17.20 ± 1.82 | 14.13 ± 2.88 | −3.07 | −3.216 | 0.001 ** |
| Time (sec) | 95.73 ± 9.52 | 87.47 ± 8.79 | −8.26 | −2.861 | 0.004 ** | |
| 3 Month after | Performance (points) | 17.60 ± 1.84 | 12.73 ± 3.15 | −4.87 | −4.210 | 0.000 *** |
| Time (sec) | 101.13 ± 7.68 | 87.00 ± 8.49 | −14.13 | −3.688 | 0.000 *** |
| Groups | Items | Pre (Mean ± S.D) | Post (Mean ± S.D) | Mean Difference | Z | p-Value |
|---|---|---|---|---|---|---|
| Experimental group | Debris index (points) | 1.32 ± 0.56 | 0.99 ± 0.38 | −0.33 | −2.673 | 0.008 ** |
| Calculus index (points) | 1.49 ± 0.69 | 0.86 ± 0.51 | −0.63 | −2.940 | 0.003 ** | |
| Total score (points) | 2.81 ± 1.14 | 1.87 ± 0.86 | −0.94 | −2.940 | 0.003 ** | |
| Control group | Debris index (points) | 1.45 ± 0.78 | 1.37 ± 0.37 | −0.08 | −0.089 | 0.929 |
| Calculus index (points) | 1.33 ± 0.88 | 1.29 ± 0.43 | −0.04 | −0.569 | 0.569 | |
| Total score (points) | 2.78 ± 1.56 | 2.73 ± 0.81 | −0.05 | −0.408 | 0.683 |
| Tests | Items | Experimental Group | Control Group | Mean Difference | Z | p-Value |
|---|---|---|---|---|---|---|
| Pre | Debris index (points) | 1.32 ± 0.56 | 1.45 ± 0.78 | 0.13 | −0.925 | 0.367 |
| Calculus index (points) | 1.49 ± 0.69 | 1.33 ± 0.88 | −0.16 | −0.520 | 0.624 | |
| Total score (points) | 2.81 ± 1.14 | 2.78 ± 1.56 | −0.03 | −0.166 | 0.870 | |
| Post | Debris index (points) | 0.99 ± 0.38 | 1.37 ± 0.37 | 0.38 | −2.455 | 0.015 * |
| Calculus index (points) | 0.86 ± 0.51 | 1.29 ± 0.43 | 0.43 | −2.020 | 0.045 * | |
| Total score (points) | 1.87 ± 0.86 | 2.73 ± 0.81 | 0.86 | −2.141 | 0.033 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeon, B.; Oh, J.; Son, S. Effects of Tooth Brushing Training, Based on Augmented Reality Using a Smart Toothbrush, on Oral Hygiene Care among People with Intellectual Disability in Korea. Healthcare 2021, 9, 348. https://doi.org/10.3390/healthcare9030348
Jeon B, Oh J, Son S. Effects of Tooth Brushing Training, Based on Augmented Reality Using a Smart Toothbrush, on Oral Hygiene Care among People with Intellectual Disability in Korea. Healthcare. 2021; 9(3):348. https://doi.org/10.3390/healthcare9030348
Chicago/Turabian StyleJeon, Byoungjin, Jinseok Oh, and Sungmin Son. 2021. "Effects of Tooth Brushing Training, Based on Augmented Reality Using a Smart Toothbrush, on Oral Hygiene Care among People with Intellectual Disability in Korea" Healthcare 9, no. 3: 348. https://doi.org/10.3390/healthcare9030348