
Lessons from the COVID-19 Pandemic on the Use of Artificial Intelligence in Digital Radiology: The Submission of a Survey to Investigate the Opinion of Insiders

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
1.1. Problems with the Use of RT-PCR
- The big demand is undermining supplies that are very complex due to complex kits and materials to be found during the pandemic.
- The type of test is particularly expensive due to both the kits and the materials used (the handling difficulties in the COVID-19 era are further increasing in price), both for man time in processing.
- The reactions involved require important technical times. Time in the pandemic era is showing itself as an important parameter, and is strongly correlated with contact tracing. Longer time implies a higher risk of spreading the SARS-CoV-2 virus.
- The type of test requires personnel trained in specific degree courses in biomedical laboratory techniques and/or biology.
- The specific training referred to in the previous point must be done in the presence of others to train the staff in the use of laboratory instruments and kits, and this is very difficult in the pandemic period, since many of the internship activities have been limited and/or replaced with remote activity.
- Focusing only on a type of test as a gold standard from the point of view of optimization and resource management is required, and an equally effective solution is needed as a backup technique.
1.2. Possible at the Moment to Investigate Answers That AI in Digital Radiology Could Give
- It has no supply-critical issues thanks to digital techniques (there are no longer the problems of plate development).
- It has no material cost problems (for the same reasons as above). In addition, AI can greatly reduce man time with automation.
- It has a response time that is immediate, which translates into important advantages for contact tracing.
- It requires trained personnel, but AI automation could make a strong contribution to cost minimization.
- It needs training, however, the training on diagnostic images can also be practiced through remote techniques thanks to the exchange of images that can also be practiced through telemedicine systems based on eHealth and mHealth.
- It could represent an alternative and/or backup system.
2. Objective
- (a)
- Develop an electronic survey on this topic suitable for a multitude of healthcare professionals;
- (b)
- Submit it and collect useful suggestions to carry out a specific survey by category useful for subsequent monitoring and interactions with the related scientific companies; and
- (c)
- Apply it to a first category of health professionals.
3. Methods
3.1. Privacy Issues
3.2. Data Protection Issues
3.3. Subjects and Perspectives
4. Results and Discussion
4.1. Numerical Outcome from the Survey
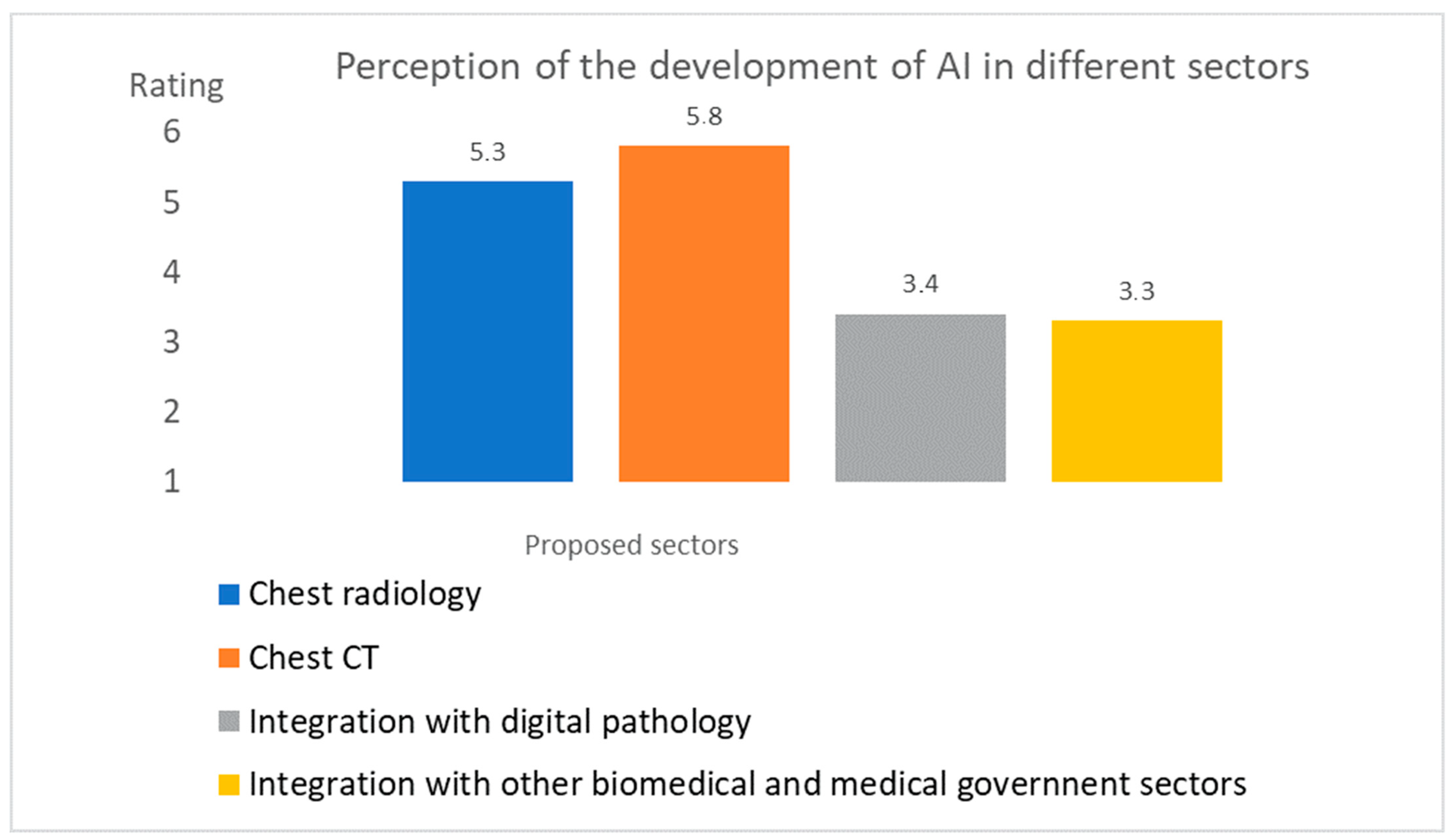
- Both chest CT and radiography were considered diagnostic areas of great development during the pandemic; both of the average values obtained were higher than TA.
- The other two areas of integration towards other non-radiological technologies were not considered areas of great development, having both obtained a value below the TA threshold.
- Both training and infrastructure were considered areas to invest in as far as artificial intelligence is concerned. The values obtained were in fact well above the TA threshold.
- The integration into eHealth and mHealth instead showed a value equal to 3.6, just above the TA threshold.
4.2. Validation of the Submission on a Second Sample of MRTs
4.3. Comments and Observations from the Survey
- (1)
- Further useful information about the problem.
- (2)
- Observations about the tool itself.
- comm-1
- Appreciation for the initiative in various forms (150 cases), which then led to the creation of the article. In some cases, the MRT figure was particularly valued.
- comm-2
- The desire for the survey to be a stable and permanent monitoring tool (11 cases).
- comm-3
- Concern about the downsizing of one’s profession due to possible automatisms (three cases).
- comm-4
- Lack of confidence in the ability to readjust work processes (four cases) on the basis of AI.
- comm-5
- The request for further development of the survey on the needs for interaction with AI (in addition to the training one has already foreseen) (four cases).
- comm-6
- The lack of clarity of the role played in a possible process of interaction with AI (three cases).
- comm-7
- The clear separation between the world of research and the world of clinical practice in reference to the topic (two cases).
- comm-8
- The non-usefulness of the questionnaire (one case).
5. Conclusions and Work in Progress
5.1. Highlights in the Study
- Digital radiology consists of a management process of radiological techniques and a decision-making process.
- The heart of the management process is the MRT, who interacts with the patient in the radiology laboratory and who is also the figure most exposed to COVID-19.
- Certainly, artificial intelligence could simplify processes with automation, reducing processing times (including exposure), decision times, and costs.
- Training in packages dedicated to AI applied to radiology could also be done with tutorials and remote training and exercises carried out on large public databases available, such as those shown in the study.
- The massive use of eHealth and/or mHealth solutions could make it easier to interact and finalize the further decision-making and/or administrative processes of RIS and HIS.
- The perception of a great development in thoracic radiography and CT, but a loss of opportunity in integration with non-radiological technologies.
- The belief that it is appropriate to invest in training and infrastructure dedicated to AI.
- The widespread idea that AI can become a strong complementary tool to human activity.
5.2. Work in Progress
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fu, L.; Wang, B.; Yuan, T.; Chen, X.; Ao, Y.; Fitzpatrick, T.; Li, P.; Zhou, Y.; Lin, Y.F.; Duan, Q.; et al. Clinical characteristics of coronavirus disease 2019 (COVID-19) in China: A systematic review and meta-analysis. J. Infect. 2020, 80, 656–665. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Rahbari, R.; Moradi, N.; Abdi, M. rRT-PCR for SARS-CoV-2: Analytical considerations. Clin. Chim. Acta 2021, 516, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Corman, V.M.; Landt, O.; Kaiser, M.; Molenkamp, R.; Meijer, A.; Chu, D.K.; Bleicker, T.; Brunink, S.; Schneider, J.; Schmidt, M.L.; et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Eurosurveillance 2020, 25, 2000045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pang, J.; Wang, M.X.; Ang, I.Y.H.; Tan, S.H.X.; Lewis, R.F.; Chen, J.I.; Gutierrez, R.A.; Gwee, S.X.W.; Chua, P.E.Y.; Yang, Q.; et al. Potential Rapid Diagnostics, Vaccine and Therapeutics for 2019 Novel Coronavirus (2019-nCoV): A Systematic Review. J. Clin. Med. 2020, 9, 623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaltenboeck, B.; Wang, C. Advances in real-time PCR: Application to clinical laboratory diagnostics. Adv. Clin. Chem. 2005, 40, 219–259. [Google Scholar] [PubMed]
- Mayer, G.; Muller, J.; Lunse, C.E. RNA diagnostics: Real-time RT-PCR strategies and promising novel target RNAs. Wiley Interdiscip. Rev. RNA 2011, 2, 32–41. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.H.; Cai, L.; Cheng, Z.S.; Cheng, H.; Deng, T.; Fan, Y.P.; Fang, C.; Huang, D.; Huang, L.Q.; Huang, Q.; et al. A rapid advice guideline for the diagnosis and treatment of 2019 novel coronavirus (2019-nCoV) infected pneumonia (standard version). Mil. Med. Res. 2020, 7, 4. [Google Scholar] [CrossRef] [Green Version]
- Lippi, G.; Plebani, M. Laboratory abnormalities in patients with COVID-2019 infection. Clin. Chem. Lab. Med. 2020, 58, 1131–1134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lippi, G.; Simundic, A.M.; Plebani, M. Potential preanalytical and analytical vulnerabilities in the laboratory diagnosis of coronavirus disease 2019 (COVID-19). Clin. Chem. Lab. Med. 2020, 58, 1070–1076. [Google Scholar] [CrossRef] [Green Version]
- Espy, M.J.; Uhl, J.R.; Sloan, L.M.; Buckwalter, S.P.; Jones, M.F.; Vetter, E.A.; Yao, J.D.; Wengenack, N.L.; Rosenblatt, J.E.; Smith, F.; et al. Real-time PCR in clinical microbiology: Applications for routine laboratory testing. Clin. Microbiol. Rev. 2006, 19, 165–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lippi, G.; Lima-Oliveira, G.; Brocco, G.; Bassi, A.; Salvagno, G.L. Estimating the intra- and inter-individual imprecision of manual pipetting. Clin. Chem. Lab. Med. 2017, 55, 962–966. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; von Meyer, A.; Cadamuro, J.; Simundic, A.M.C. European Federation of Clinical, P. Laboratory Medicine Working Group for Preanalytical, PREDICT: A checklist for preventing preanalytical diagnostic errors in clinical trials. Clin. Chem. Lab. Med. 2020, 58, 518–526. [Google Scholar] [CrossRef] [Green Version]
- van Zyl, G.; Maritz, J.; Newman, H.; Preiser, W. Lessons in diagnostic virology: Expected and unexpected sources of error. Rev. Med. Virol. 2019, 29, e2052. [Google Scholar] [PubMed]
- Tang, Y.W.; Schmitz, J.E.; Persing, D.H.; Stratton, C.W. Laboratory Diagnosis of COVID-19: Current Issues and Challenges. J. Clin. Microbiol. 2020, 58, 108. [Google Scholar] [CrossRef] [Green Version]
- Alsharif, M.H.; Alsharif, Y.H.; Yahya, K.; Alomari, O.A.; Albreem, M.A.; Jahid, A. Deep learning applications to combat the dissemination of COVID-19 disease: A review. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 11455–11460. [Google Scholar] [CrossRef]
- Ozsahin, I.; Sekeroglu, B.; Musa, M.S.; Mustapha, M.T.; Uzun Ozsahin, D. Review on Diagnosis of COVID-19 from Chest CT Images Using Artificial Intelligence. Comput. Math. Methods Med. 2020, 2020, 9756518. [Google Scholar] [CrossRef]
- Pham, T.D. Classification of COVID-19 chest X-rays with deep learning: New models or fine tuning? Health Inf. Sci. Syst. 2020, 9, 2. [Google Scholar] [CrossRef]
- COVID-19 Radiography Database. Available online: https://www.kaggl e.com/tawsifurrahman/covid19-radiography-database (accessed on 2 July 2020).
- COVID-19 Chest X-ray Dataset Initiative. Available online: https://githu b.com/agchung/Figure1-COVID -chestxray-datas et (accessed on 2 July 2020).
- IEEE8023/Covid Chest X-ray Dataset. Available online: https://githu b.com/ieee8 023/covid-chest xray-datas et (accessed on 2 July 2020).
- van Ginneken, B. The Potential of Artificial Intelligence to Analyze Chest Radiographs for Signs of COVID-19 Pneumonia. Radiology 2020, 204238. [Google Scholar] [CrossRef]
- Wehbe, R.M.; Sheng, J.; Dutta, S.; Chai, S.; Dravid, A.; Barutcu, S.; Wu, Y.; Cantrell, D.R.; Xiao, N.; Allen, B.D.; et al. DeepCOVID-XR: An Artificial Intelligence Algorithm to Detect COVID-19 on Chest Radiographs Trained and Tested on a Large US Clinical Dataset. Radiology 2020, 203511. [Google Scholar] [CrossRef]
- Murphy, K.; Smits, H.; Knoops, A.J.G.; Korst, M.B.J.M.; Samson, T.; Scholten, E.T.; Schalekamp, S.; Schaefer-Prokop, C.M.; Philipsen, R.H.H.M.; Meijers, A.; et al. COVID-19 on the Chest Radiograph: A Multi-Reader Evaluation of an AI System. Radiology 2020, 296, E166–E172. [Google Scholar] [CrossRef]
- Zhang, R.; Xin Tie, X.; Qi, Z.; Bevins, N.B.; Zhang, C.; Griner, D.; Song, T.K.; Nadig, J.D.; Schiebler, M.L.; Garrett, J.W.; et al. Diagnosis of COVID-19 Pneumonia Using Chest Radiography: Value of Artificial Intelligence. Radiology 2020. [Google Scholar] [CrossRef]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. ImageNet classification with deep convolutional neural networks. Commun. ACM 2017, 60, 84–90. [Google Scholar] [CrossRef]
- Szegedy, C.; Liu, W.; Jia, Y.; Sermanet, P.; Reed, S.; Anguelov, D.; Erhan, D.; Vanhoucke, V.; Rabinovich, A. Going deeper with convolutions. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Columbus, OH, USA, 23–28 June 2015; pp. 1–9. [Google Scholar]
- Iandola, F.N.; Han, S.; Moskewicz, M.W.; Ashraf, K.; Dally, W.J.; Keutzer, K. SqueezeNet: AlexNet-level accuracy with 50x fewer parameters and <0.5 MB model size. arXiv 2016, arXiv:1602.07360. [Google Scholar]
- Summers, R.M. Artificial Intelligence of COVID-19 Imaging: A Hammer in Search of a Nail. Radiology 2020, 204226. [Google Scholar] [CrossRef]
- Giansanti, D. The artificial intelligence in digital pathology and digital radiology: Where are we? Healthcare 2021, 9, 30. [Google Scholar] [CrossRef]
- Giansanti, D. Towards the evolution of the mHealth in mental health with youth: The cyber-space used in psychological rehabilitation is becoming wearable into a pocket. mHealth 2020, 6, 18. [Google Scholar] [CrossRef] [PubMed]
- Giansanti, D.; Monoscalco, L. The Cyber-Risk in Cardiology: Towards an Investigation on the Self Perception among the Cardiologists. mHealth 2020. Available online: https://mhealth.amegroups.com/article/view/37310/28600 (accessed on 13 March 2021).
- Giansanti, D.; Monoscalco, L. A smartphone-based survey in mHealth to investigate the introduction of the artificial intelligence into cardiology. mHealth 2021. [Google Scholar] [CrossRef] [PubMed]







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giansanti, D.; Rossi, I.; Monoscalco, L. Lessons from the COVID-19 Pandemic on the Use of Artificial Intelligence in Digital Radiology: The Submission of a Survey to Investigate the Opinion of Insiders. Healthcare 2021, 9, 331. https://doi.org/10.3390/healthcare9030331
Giansanti D, Rossi I, Monoscalco L. Lessons from the COVID-19 Pandemic on the Use of Artificial Intelligence in Digital Radiology: The Submission of a Survey to Investigate the Opinion of Insiders. Healthcare. 2021; 9(3):331. https://doi.org/10.3390/healthcare9030331
Chicago/Turabian StyleGiansanti, Daniele, Ivano Rossi, and Lisa Monoscalco. 2021. "Lessons from the COVID-19 Pandemic on the Use of Artificial Intelligence in Digital Radiology: The Submission of a Survey to Investigate the Opinion of Insiders" Healthcare 9, no. 3: 331. https://doi.org/10.3390/healthcare9030331