
Photoinactivation of Staphylococci with 405 nm Light in a Trachea Model with Saliva Substitute at 37 °C

 ,
,  , ,
, ,  and
and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Microorganism and Medium
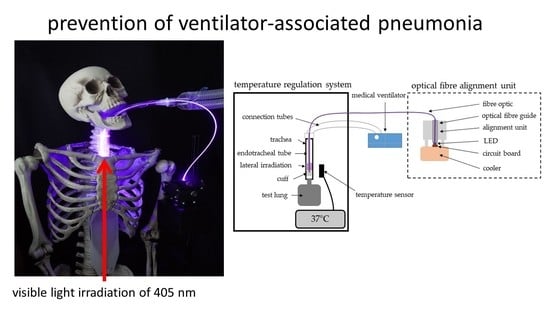
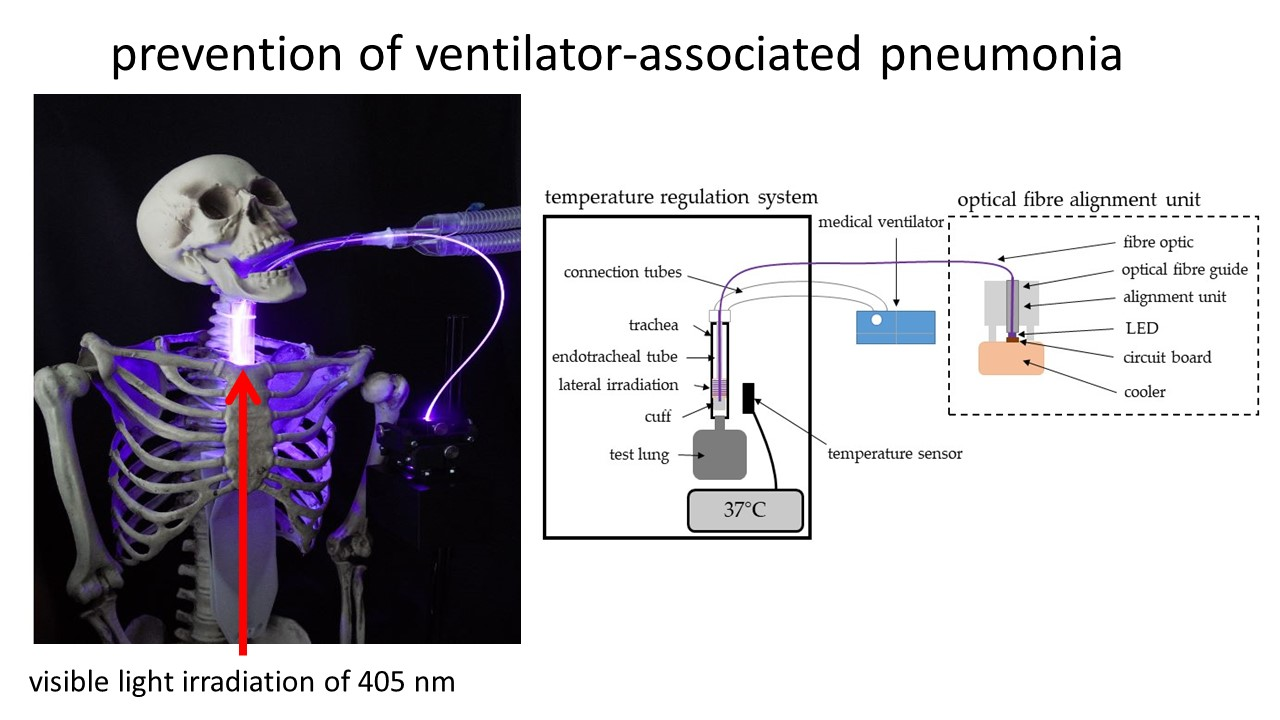
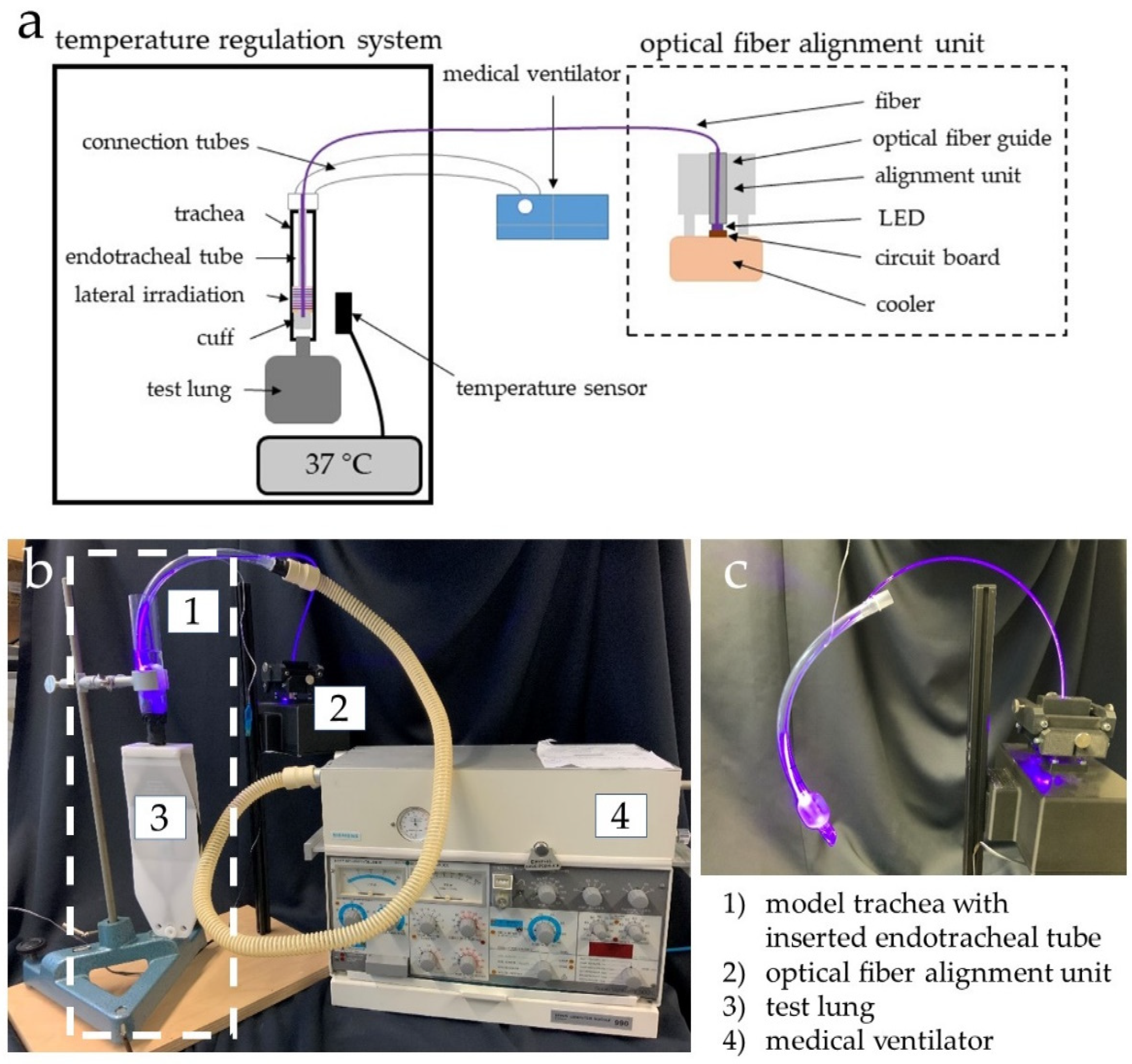
2.2. Illuminated Endotracheal Tube Prototype
2.3. Test Setup
2.4. Microbiological Experiments
2.4.1. S. carnosus Irradiation in PBS at 37 °C and 25 °C
2.4.2. Artificial Saliva Solution Comparison at 37 °C
2.4.3. S. carnosus Irradiation in Sal3 at 37 °C
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pendleton, J.N.; Gorman, S.P.; Gilmore, B.F. Clinical relevance of the ESKAPE pathogens. Expert Rev. Anti-Infect. Ther. 2013, 11, 297–308. [Google Scholar] [CrossRef] [PubMed]
- Rice, L.B. Federal Funding for the Study of Antimicrobial Resistance in Nosocomial Pathogens: No ESKAPE. J. Infect. Dis. 2008, 197, 1079–1081. [Google Scholar] [CrossRef] [PubMed]
- Craven, T.H.; Wojcik, G.; McCoubrey, J.; Brooks, O.; Grant, E.; Keating, S.; Reilly, J.; Laurenson, I.F.; Kefala, K.; Walsh, T.S. Ventilator-associated pneumonia surveillance using two methods. J. Hosp. Infect. 2020, 104, 522–528. [Google Scholar] [CrossRef] [PubMed]
- Melsen, W.G.; Rovers, M.M.; Groenwold, R.H.H.; Bergmans, D.C.J.J.; Camus, C.; Bauer, T.T.; Hanisch, E.W.; Klarin, B.; Koeman, M.; Krueger, W.A.; et al. Attributable mortality of ventilator-associated pneumonia: A meta-analysis of individual patient data from randomised prevention studies. Lancet Infect. Dis. 2013, 13, 665–671. [Google Scholar] [CrossRef]
- Dullenkopf, A.; Gerber, A.; Weiss, M. Fluid leakage past tracheal tube cuffs: Evaluation of the new Microcuff endotracheal tube. Intensive Care Med. 2003, 29, 1849–1853. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zanella, A.; Scaravilli, V.; Isgrò, S.; Milan, M.; Cressoni, M.; Patroniti, N.; Fumagalli, R.; Pesenti, A. Fluid leakage across tracheal tube cuff, effect of different cuff material, shape, and positive expiratory pressure: A bench-top study. Intensive Care Med. 2011, 37, 343–347. [Google Scholar] [CrossRef]
- Gil-Perotin, S.; Ramirez, P.; Marti, V.; Sahuquillo, J.M.; Gonzalez, E.; Calleja, I.; Menendez, R.; Bonastre, J. Implications of endotracheal tube biofilm in ventilator-associated pneumonia response: A state of concept. Crit. Care 2012, 16. [Google Scholar] [CrossRef] [Green Version]
- de Souza, P.R.; de Andrade, D.; Cabral, D.B.; Watanabe, E. Endotracheal tube biofilm and ventilator-associated pneumonia with mechanical ventilation. Microsc. Res. Tech. 2014, 77, 305–312. [Google Scholar] [CrossRef]
- Diaconu, O.; Siriopol, I.; Poloșanu, L.I.; Grigoraș, I. Endotracheal Tube Biofilm and its Impact on the Pathogenesis of Ventilator-Associated Pneumonia. J. Crit. Care Med. (Targu Mures) 2018, 4, 50–55. [Google Scholar] [CrossRef] [Green Version]
- Danin, P.-E.; Girou, E.; Legrand, P.; Louis, B.; Fodil, R.; Christov, C.; Devaquet, J.; Isabey, D.; Brochard, L. Description and microbiology of endotracheal tube biofilm in mechanically ventilated subjects. Respir. Care 2015, 60, 21–29. [Google Scholar] [CrossRef] [Green Version]
- Restrepo, M.I.; Anzueto, A.; Arroliga, A.C.; Afessa, B.; Atkinson, M.J.; Ho, N.J.; Schinner, R.; Bracken, R.L.; Kollef, M.H. Economic burden of ventilator-associated pneumonia based on total resource utilization. Infect. Control Hosp. Epidemiol. 2010, 31, 509–515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bekaert, M.; Timsit, J.-F.; Vansteelandt, S.; Depuydt, P.; Vésin, A.; Garrouste-Orgeas, M.; Decruyenaere, J.; Clec’h, C.; Azoulay, E.; Benoit, D. Attributable mortality of ventilator-associated pneumonia: A reappraisal using causal analysis. Am. J. Respir. Crit. Care Med. 2011, 184, 1133–1139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bundesamt für Verbraucherschutz und Lebensmittelsicherheit, Paul-Ehrlich-Gesellschaft. Report on the Consumption of Antimicrobials and the Spread of Antimicrobial Resistance in Human and Veterinary Medicine in Germany; Paul-Ehrlich-Gesellschaft für Chemotherapie e.V.: Rheinbach, Germany, 2015; pp. 1–183. [Google Scholar]
- Fair, R.; Tor, Y. Antibiotics and bacterial resistance in the 21st century. Perspect. Medicin. Chem. 2014, 6, 25–64. [Google Scholar] [CrossRef] [Green Version]
- Boucher, H.W.; Murray, B.E.; Powderly, W.G. Proposed U.S. Funding Cuts Threaten Progress on Antimicrobial Resistance. Ann. Intern. Med. 2017, 167, 738–739. [Google Scholar] [CrossRef] [PubMed]
- Spellberg, B.; Powers, J.H.; Brass, E.P.; Miller, L.G.; Edwards, J.E. Trends in antimicrobial drug development: Implications for the future. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2004, 38, 1279–1286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Behnke, M.; Aghdassi, S.J.; Hansen, S.; Diaz, L.A.P.; Gastmeier, P.; Piening, B. The Prevalence of Nosocomial Infection and Antibiotic Use in German Hospitals. Dtsch. Arztebl. Int. 2017, 114, 851–857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghosh, C.; Sarkar, P.; Issa, R.; Haldar, J. Alternatives to Conventional Antibiotics in the Era of Antimicrobial Resistance. Trends Microbiol. 2019, 27, 323–338. [Google Scholar] [CrossRef]
- Allen, H.K.; Trachsel, J.; Looft, T.; Casey, T.A. Finding alternatives to antibiotics. Ann. N. Y. Acad. Sci. 2014, 1323, 91–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hessling, M.; Spellerberg, B.; Hoenes, K. Photoinactivation of bacteria by endogenous photosensitizers and exposure to visible light of different wavelengths—A review on existing data. FEMS Microbiol. Lett. 2017, 364. [Google Scholar] [CrossRef] [PubMed]
- Rutala, W.; Kanamori, H.; Gergen, M.; Laux, J.; Sickbert-Bennett, E.; Anderson, D.; Sexton, D.; Weber, D. Light-emitting diode Disinfection as Continuous Room Surface Decontamination against Healthcare-Associated Pathogens. Open Forum Infect. Dis. 2017, 4, 194. [Google Scholar] [CrossRef]
- Murdoch, L.; Maclean, M.; MacGregor, J.; Anderson, G. Bactericidal effects of 405 nm light exposure demonstrated by inactivation of Escherichia, Salmonella, Shigella, Listeria, and Mycobacterium species in liquid suspensions and on exposed surfaces. Sci. World J. 2012, 2012, 137805. [Google Scholar] [CrossRef] [Green Version]
- Wang, T.; Dong, J.; Yin, H.; Zhang, G. Blue light therapy to treat candida vaginitis with comparisons of three wavelengths: An in vitro study. Lasers Med. Sci. 2020, 35, 1329–1339. [Google Scholar] [CrossRef]
- Ananthaswamy, H.N.; Pierceall, W.E. Molecular mechanisms of ultraviolet radiation carcinogenesis. Photochem. Photobiol. 1990, 52, 1119–1136. [Google Scholar] [CrossRef]
- Plavskii, V.Y.; Mikulich, A.V.; Tretyakova, A.I.; Leusenka, I.A.; Plavskaya, L.G.; Kazyuchits, O.A.; Dobysh, I.I.; Krasnenkova, T.P. Porphyrins and flavins as endogenous acceptors of optical radiation of blue spectral region determining photoinactivation of microbial cells. J. Photochem. Photobiol. B 2018, 183, 172–183. [Google Scholar] [CrossRef]
- Maclean, M.; MacGregor, S.J.; Anderson, J.G.; Woolsey, G. Inactivation of bacterial pathogens following exposure to light from a 405-nanometer light-emitting diode array. Appl. Environ. Microbiol. 2009, 75, 1932–1937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sicks, B.; Hoenes, K.; Spellerberg, B.; Hessling, M. Blue LEDs in Endotracheal Tubes May Prevent Ventilator-Associated Pneumonia. Photobiomodulation Photomed. Laser Surg. 2020. [Google Scholar] [CrossRef]
- Feldman, C.; Kassel, M.; Cantrell, J.; Kaka, S.; Morar, R.; Goolam Mahomed, A.; Philips, J.I. The presence and sequence of endotracheal tube colonization in patients undergoing mechanical ventilation. Eur. Respir. J. 1999, 13, 546–551. [Google Scholar] [CrossRef] [PubMed]
- Pytko-Polonczyk, J.; Jakubik, A.; Przeklasa-Bierowiec, A.; Muszynska, B. Artificial saliva and its use in biological experiments. J. Physiol. Pharmacol. Off. J. Pol. Physiol. Soc. 2017, 68, 807–813. [Google Scholar]
- Tanthanuch, S.; Kukiattrakoon, B.; Peerasukprasert, T.; Chanmanee, N.; Chaisomboonphun, P.; Rodklai, A. The effect of red and white wine on color changes of nanofilled and nanohybrid resin composites. Restor. Dent. Endod. 2016, 41, 130–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanthanuch, S.; Kukiattrakoon, B.; Peerasukprasert, T.; Chanmanee, N.; Chaisomboonphun, P.; Rodklai, A. Surface roughness and erosion of nanohybrid and nanofilled resin composites after immersion in red and white wine. J. Conserv. Dent. 2016, 19, 51–55. [Google Scholar] [CrossRef]
- DA Silva, M.A.B.; Vitti, R.P.; Sinhoreti, M.A.C.; Consani, R.L.X.; Da Silva-Júnior, J.G.; Tonholo, J. Effect of alcoholic beverages on surface roughness and microhardness of dental composites. Dent. Mater. J. 2016, 35, 621–626. [Google Scholar] [CrossRef] [Green Version]
- Pistone, S.; Goycoolea, F.M.; Young, A.; Smistad, G.; Hiorth, M. Formulation of polysaccharide-based nanoparticles for local administration into the oral cavity. Eur. J. Pharm. Sci. 2017, 96, 381–389. [Google Scholar] [CrossRef] [PubMed]
- Gal, J.; Fovet, Y.; Adib-Yadzi, M. About a synthetic saliva for in vitro studies. Talanta 2001, 53, 1103–1115. [Google Scholar] [CrossRef]
- Arvidson, K.; Johansson, E.G. Galvanic currents between dental alloys in vitro. Scand. J. Dent. Res. 1985, 93, 467–473. [Google Scholar] [CrossRef]
- Alshali, R.Z.; Salim, N.A.; Satterthwaite, J.D.; Silikas, N. Long-term sorption and solubility of bulk-fill and conventional resin-composites in water and artificial saliva. J. Dent. 2015, 43, 1511–1518. [Google Scholar] [CrossRef]
- Humphrey, S.P.; Williamson, R.T. A review of saliva: Normal composition, flow, and function. J. Prosthet. Dent. 2001, 85, 162–169. [Google Scholar] [CrossRef] [PubMed]
- Andrei, M.; Galateanu, B.; Hudita, A.; Costache, M.; Osiceanu, P.; Calderon Moreno, J.M.; Drob, S.I.; Demetrescu, I. Electrochemical comparison and biological performance of a new CoCrNbMoZr alloy with commercial CoCrMo alloy. Mater. Sci. Eng. C Mater. Biol. Appl. 2016, 59, 346–355. [Google Scholar] [CrossRef]
- Romonti, D.E.; Gomez Sanchez, A.V.; Milošev, I.; Demetrescu, I.; Ceré, S. Effect of anodization on the surface characteristics and electrochemical behaviour of zirconium in artificial saliva. Mater. Sci. Eng. C Mater. Biol. Appl. 2016, 62, 458–466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fusayama, T.; Katayori, T.; Nomote, S. Corrosion of Gold and Amalgam Placed in Contact with Each other. J. Dent. Res. 1963, 42, 1183–1197. [Google Scholar] [CrossRef] [PubMed]
- Pulikkottil, V.J.; Chidambaram, S.; Bejoy, P.U.; Femin, P.K.; Paul, P.; Rishad, M. Corrosion resistance of stainless steel, nickel-titanium, titanium molybdenum alloy, and ion-implanted titanium molybdenum alloy archwires in acidic fluoride-containing artificial saliva: An in vitro study. J. Pharm. Bioallied Sci. 2016, 8, S96–S99. [Google Scholar] [CrossRef] [PubMed]
- St Denis, T.G.; Vecchio, D.; Zadlo, A.; Rineh, A.; Sadasivam, M.; Avci, P.; Huang, L.; Kozinska, A.; Chandran, R.; Sarna, T.; et al. Thiocyanate potentiates antimicrobial photodynamic therapy: In situ generation of the sulfur trioxide radical anion by singlet oxygen. Free Radic. Biol. Med. 2013, 65, 800–810. [Google Scholar] [CrossRef] [Green Version]
- Momm, F.; Volegova-Neher, N.J.; Schulte-Mönting, J.; Guttenberger, R. Different saliva substitutes for treatment of xerostomia following radiotherapy. A prospective crossover study. Strahlenther. Onkol. 2005, 181, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Mystkowska, J.; Car, H.; Dąbrowski, J.R.; Romanowska, J.; Klekotka, M.; Milewska, A.J. Artificial Mucin-based Saliva Preparations—Physicochemical and Tribological Properties. Oral Health Prev. Dent. 2018, 16, 183–193. [Google Scholar] [CrossRef] [PubMed]
- Vissink, A.; Waterman, H.A.; s-Gravenmade, E.J.; Panders, A.K.; Vermey, A. Rheological properties of saliva substitutes containing mucin, carboxymethylcellulose or polyethylenoxide. J. Oral Pathol. 1984, 13, 22–28. [Google Scholar] [CrossRef]
- Hahnel, S.; Behr, M.; Handel, G.; Bürgers, R. Saliva substitutes for the treatment of radiation-induced xerostomia—a review. Support. Care Cancer 2009, 17, 1331–1343. [Google Scholar] [CrossRef] [PubMed]
- Wagner, C.E.; Wheeler, K.M.; Ribbeck, K. Mucins and Their Role in Shaping the Functions of Mucus Barriers. Annu. Rev. Cell Dev. Biol. 2018, 34, 189–215. [Google Scholar] [CrossRef] [Green Version]
- Tabak, L.A.; Levine, M.J.; Mandel, I.D.; Ellison, S.A. Role of salivary mucins in the protection of the oral cavity. J. Oral Pathol. 1982, 11, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Wolinsky, L.E.; Seto, B.; Cerveny, R. Effect of saliva substitutes upon binding of selected oral bacteria to hydroxyapatite. Caries Res. 1985, 19, 507–511. [Google Scholar] [CrossRef]
- de Jong, M.H.; van der Hoeven, J.S.; van OS, J.H.; Olijve, J.H. Growth of oral Streptococcus species and Actinomyces viscosus in human saliva. Appl. Environ. Microbiol. 1984, 47, 901–904. [Google Scholar] [CrossRef] [Green Version]
- Pratten, J.; Wills, K.; Barnett, P.; Wilson, M. In vitro studies of the effect of antiseptic-containing mouthwashes on the formation and viability of Streptococcus sanguis biofilms. J. Appl. Microbiol. 1998, 84, 1149–1155. [Google Scholar] [CrossRef] [PubMed]
- Dionysopoulos, D.; Strakas, D.; Koliniotou-Koumpia, E.; Koumpia, E. Effect of Er,Cr:YSGG laser irradiation on bovine enamel surface during in-office tooth bleaching ex vivo. Odontology 2017, 105, 320–328. [Google Scholar] [CrossRef]
- Qian, C.; Wu, X.; Zhang, F.; Yu, W. Electrochemical impedance investigation of Ni-free Co-Cr-Mo and Co-Cr-Mo-Ni dental casting alloy for partial removable dental prosthesis frameworks. J. Prosthet. Dent. 2016, 116, 112–118. [Google Scholar] [CrossRef]
- Engelhart, K.; Popescu, A.; Bernhardt, J. Using mid infrared technology as new method for the determination of the dwell time of salivary substitutes on three dimensional gingiva models. BMC Ear Nose Throat Disord. 2016, 16, 6. [Google Scholar] [CrossRef] [Green Version]
- Hashemi, M.M.; Rovig, J.; Bateman, J.; Holden, B.S.; Modelzelewski, T.; Gueorguieva, I.; von Dyck, M.; Bracken, R.; Genberg, C.; Deng, S.; et al. Preclinical testing of a broad-spectrum antimicrobial endotracheal tube coated with an innate immune synthetic mimic. J. Antimicrob. Chemother. 2018, 73, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Klompas, M. Oropharyngeal Decontamination with Antiseptics to Prevent Ventilator-Associated Pneumonia: Rethinking the Benefits of Chlorhexidine. Semin. Respir. Crit. Care Med. 2017, 38, 381–390. [Google Scholar] [CrossRef] [PubMed]
- Munro, C.L.; Grap, M.J.; Sessler, C.N.; Elswick, R.K.; Mangar, D.; Karlnoski-Everall, R.; Cairns, P. Preintubation application of oral chlorhexidine does not provide additional benefit in prevention of early-onset ventilator-associated pneumonia. Chest 2015, 147, 328–334. [Google Scholar] [CrossRef] [Green Version]
- Dsouza, R.; Spillman, D.R., Jr.; Barkalifa, R.; Monroy, G.L.; Chaney, E.J.; Johnson, M.A.; White, K.C.; Boppart, S.A. Efficacy of endotracheal tube suctioning in intubated intensive care unit patients determined by in vivo catheter-based optical coherence tomography—A pilot study. Quant. Imaging Med. Surg. 2020, 11, 1–8. [Google Scholar] [CrossRef]
- Hart, R.; McNeill, S.; Maclean, S.; Hornsby, J.; Ramsay, S. The prevalence of suspected ventilator-associated pneumonia in Scottish intensive care units. J. Intensive Care Soc. 2020, 21, 140–147. [Google Scholar] [CrossRef]
- Pozuelo-Carrascosa, D.P.; Herráiz-Adillo, Á.; Alvarez-Bueno, C.; Añón, J.M.; Martínez-Vizcaíno, V.; Cavero-Redondo, I. Subglottic secretion drainage for preventing ventilator-associated pneumonia: An overview of systematic reviews and an updated meta-analysis. Eur. Respir. Rev. 2020, 29. [Google Scholar] [CrossRef] [Green Version]
- Rouzé, A.; de Jonckheere, J.; Zerimech, F.; Labreuche, J.; Parmentier-Decrucq, E.; Voisin, B.; Jaillette, E.; Maboudou, P.; Balduyck, M.; Nseir, S. Efficiency of an electronic device in controlling tracheal cuff pressure in critically ill patients: A randomized controlled crossover study. Ann. Intensive Care 2016, 6, 93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valencia, M.; Ferrer, M.; Farre, R.; Navajas, D.; Badia, J.R.; Nicolas, J.M.; Torres, A. Automatic control of tracheal tube cuff pressure in ventilated patients in semirecumbent position: A randomized trial. Crit. Care Med. 2007, 35, 1543–1549. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.-Y.; Wintner, A.; Seed, P.C.; Brauns, T.; Gelfand, J.A.; Hamblin, M.R. Antimicrobial photodynamic therapy mediated by methylene blue and potassium iodide to treat urinary tract infection in a female rat model. Sci. Rep. 2018, 8, 7257. [Google Scholar] [CrossRef] [PubMed]
- Shehatou, C.; Logunov, S.L.; Dunman, P.M.; Haidaris, C.G.; Klubben, W.S. Characterizing the Antimicrobial Properties of 405 nm Light and the Corning® Light-Diffusing Fiber Delivery System. Lasers Surg. Med. 2019, 51, 887–896. [Google Scholar] [CrossRef] [Green Version]
- Biel, M.A.; Sievert, C.; Usacheva, M.; Teichert, M.; Wedell, E.; Loebel, N.; Rose, A.; Zimmermann, R. Reduction of Endotracheal Tube Biofilms Using Antimicrobial Photodynamic Therapy. Lasers Surg. Med. 2011, 43, 586–590. [Google Scholar] [CrossRef] [PubMed]
- Ganz, R.A.; Viveiros, J.; Ahmad, A.; Ahmadi, A.; Khalil, A.; Tolkoff, M.J.; Nishioka, N.S.; Hamblin, M.R. Helicobacter pylori in patients can be killed by visible light. Lasers Surg. Med. 2005, 36, 260–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lembo, A.J.; Ganz, R.A.; Sheth, S.; Cave, D.; Kelly, C.; Levin, P.; Kazlas, P.T.; Baldwin, P.C.; Lindmark, W.R.; McGrath, J.R.; et al. Treatment of Helicobacter pylori infection with intra-gastric violet light phototherapy: A pilot clinical trial. Lasers Surg. Med. 2009, 41, 337–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morici, P.; Battisti, A.; Tortora, G.; Menciassi, A.; Checcucci, G.; Ghetti, F.; Sgarbossa, A. The in vitro Photoinactivation of Helicobacter pylori by a Novel LED-Based Device. Front. Microbiol. 2020, 11, 283. [Google Scholar] [CrossRef] [Green Version]
- Battisti, A.; Fusi, F.; Orsini, B.; Romano, G.; Faraoni, P.; Gnerucci, A.; Tortora, G.; Menciassi, A.; Morici, P.; Checcucci, G.; et al. Design of an ingestible robotic pill based on LED sources for the treatment of gastrointestinal disorders. In Proceedings of the European Society for Photobiology 2017 Congress, Pisa, Italy, 4–8 September 2017. [Google Scholar] [CrossRef]
- Romano, G.; Tortora, G.; Calusi, S.; Orsini, B.; Gnerucci, A.; Fusi, F. Minimally invasive ingestible device to perform anti-bacterial phototherapy in the stomach. Phys. Med. 2016, 32, 215. [Google Scholar] [CrossRef]
- Hoenes, K.; Bauer, R.; Meurle, T.; Spellerberg, B.; Hessling, M. Inactivation Effect of Violet and Blue Light on ESKAPE Pathogens and closely related non-pathogenic Bacterial Species: A Promising Tool Against Antibiotic-Sensitive and Antibiotic-Resistant Microorganisms. Front. Microbiol. 2021, 11, 3429. [Google Scholar] [CrossRef]
- Enwemeka, C.S.; Williams, D.; Hollosi, S.; Yens, D.; Enwemeka, S.K. Visible 405 nm SLD light photo-destroys methicillin-resistant Staphylococcus aureus (MRSA) in vitro. Lasers Surg. Med. 2008, 40, 734–737. [Google Scholar] [CrossRef]
- Barneck, M.D.; Rhodes, N.L.R.; de La Presa, M.; Allen, J.P.; Poursaid, A.E.; Nourian, M.M.; Firpo, M.A.; Langell, J.T. Violet 405-nm light: A novel therapeutic agent against common pathogenic bacteria. J. Surg. Res. 2016, 206, 316–324. [Google Scholar] [CrossRef] [PubMed]
- Endarko, E.; Maclean, M.; Timoshkin, I.V.; MacGregor, S.J.; Anderson, J.G. High-intensity 405 nm light inactivation of Listeria monocytogenes. Photochem. Photobiol. 2012, 88, 1280–1286. [Google Scholar] [CrossRef] [PubMed]
- McKenzie, K.; Maclean, M.; Timoshkin, I.V.; MacGregor, S.J.; Anderson, J.G. Enhanced inactivation of Escherichia coli and Listeria monocytogenes by exposure to 405nm light under sub-lethal temperature, salt and acid stress conditions. Int. J. Food Microbiol. 2014, 170, 91–98. [Google Scholar] [CrossRef] [Green Version]
- Rath, K.M.; Maheshwari, A.; Bengtson, P.; Rousk, J. Comparative Toxicities of Salts on Microbial Processes in Soil. Appl. Environ. Microbiol. 2016, 82, 2012–2020. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sal1 [52] | Sal2 [40,53] | Sal3 [54] | Sal4 [51] |
|---|---|---|---|
| 19 mg/L MgCl2 6H20 2240 mg/L KCl 103 mg/L CaCl2 544 mg/L KH2PO2 | 400 mg/L NaCl 400 mg/L KCl 795 mg/L CaCl2 2H2O 690 mg/L NaH2PO2 H2O 5 mg/L Na2S 9H2O 1000 mg/L Urea (CH4N2O) | 4200 mg/L NaHCO3 500 mg/L NaCl 200 mg/L KCl | 1 g meat extract 2 g yeast extract 5 g proteose peptone 0.2 g NaCl 0.2 g KCl 0.3 g CaCl2 1.25 mL Urea 40% sterile filtered 1000 mL aqua dem. |
| Target Organ | Aim | Application | Reference |
|---|---|---|---|
| trachea | prevention of VAP | integration of 48 miniature LEDs in wall of ETT to reduce bacterial concentration in accumulating secretion at cuff, in vitro model, 450 nm, 6.6/13.4 mW/cm2, 280/480 J/cm2, room temperature | [27] |
| trachea | prevention of biofilm formation on ETT | in vitro polymicrobial biofilm of P. aeruginosa and S. aureus, light delivery by catheter, methylene blue (500 µg/mL) + 664 nm, 150 J/cm length of catheter | [65] |
| stomach | therapy of H. pylori colonization and correspondent diseases, especially in cases of antibiotic failure | in vivo, 10 patients with symptoms of dyspepsia or suspected peptide ulcer disease and tested positive for H. pylori, optical fiber passed through endoscope, 405 nm, 40 J/cm2 | [66] |
| stomach | therapy of H. pylori infection | in vivo, 18 patients, fiber optic bundle with diffusor with over-tube for flow of coolant to maintain 45° C, catheter-sheath in form of a multi-segmented balloon for positioning, 408 nm, 31–46 kJ, repopulation after irradiation | [67] |
| stomach | therapy of gastric infections | presentation of the idea of an ingestible LED capsule, in vitro tests on H. pylori and prototype design, 405 nm, 460 nm, (500 nm, 625 nm) | [68,69,70] |
| not specified | presenting a non-traditional approach for the prevention and/or therapeutic intervention of hospital acquired infections | in vitro tests on ESKAPE-pathogens and eukaryotic cells, experiments on agar, in liquid culture (incl. lung surfactant, human serum) and on surfaces, flexible Corning® light-diffusing fiber from silica glass, 230 µm diameter, 405 nm, 36–540 J/cm2 | [64] |
| urinary tract | therapy of catheter-associated urinary tract infections (CAUTI) | female rat model, light delivery by direct introduction of diffusing fiber into the bladder, 660 nm, 50 mW/cm2, 100 J/cm2, external addition of photosensitizer methylene blue and salt potassium iodide prior to irradiation by catheter | [63] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meurle, T.; Knaus, J.; Barbano, A.; Hoenes, K.; Spellerberg, B.; Hessling, M. Photoinactivation of Staphylococci with 405 nm Light in a Trachea Model with Saliva Substitute at 37 °C. Healthcare 2021, 9, 310. https://doi.org/10.3390/healthcare9030310
Meurle T, Knaus J, Barbano A, Hoenes K, Spellerberg B, Hessling M. Photoinactivation of Staphylococci with 405 nm Light in a Trachea Model with Saliva Substitute at 37 °C. Healthcare. 2021; 9(3):310. https://doi.org/10.3390/healthcare9030310
Chicago/Turabian StyleMeurle, Tobias, Johannes Knaus, Agustin Barbano, Katharina Hoenes, Barbara Spellerberg, and Martin Hessling. 2021. "Photoinactivation of Staphylococci with 405 nm Light in a Trachea Model with Saliva Substitute at 37 °C" Healthcare 9, no. 3: 310. https://doi.org/10.3390/healthcare9030310