
Marital Stability and Quality of Couple Relationships after Acquired Brain Injury: A Two-Year Follow-Up Clinical Study



Abstract
:1. Introduction
2. Materials and Methods
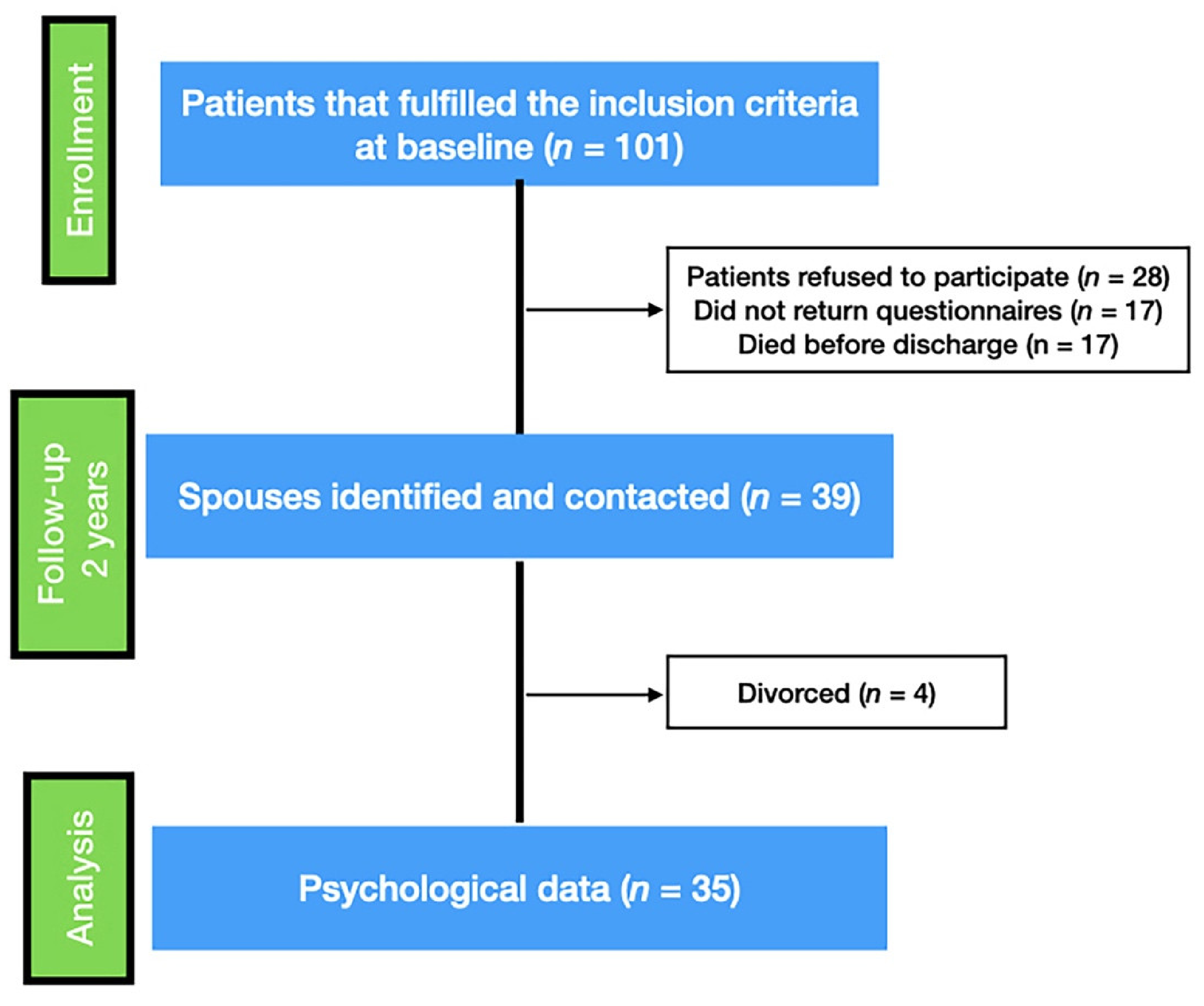
2.1. Participants
2.2. Design and Procedure
2.3. Outcome Measures
2.4. Statistical Analysis
3. Results
3.1. Clinical Data
3.2. Regression Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Anderson, A.; Keating, N. Marriage after the transition to stroke: A systematic review. Ageing Soc. 2018, 38, 2241–2279. [Google Scholar] [CrossRef]
- Burridge, A.C.; Huw, W.W.; Yates, P.J.; Harris, A.; Ward, C. Spousal relationship satisfaction following acquired brain injury: The role of insight and socio-emotional skill. Neuropsychol. Rehabil. 2007, 17, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Hammond, F.M.; Davis, C.S.; Whiteside, O.Y.; Philbrick, P.; Hirsch, M.A. Marital adjustment and stability following traumatic brain injury: A pilot qualitative analysis of spouse perspectives. J. Head Trauma Rehabil. 2011, 26, 69–78. [Google Scholar] [CrossRef] [PubMed]
- Stevens, L.F.; Lapis, Y.; Tang, X.; Sander, A.M.; Dreer, L.E.; Hammond, F.M.; Kreutzer, J.S.; O’Neil-Pirozzi, T.M.; Nakase-Richardson, R. Relationship Stability after Traumatic Brain Injury Among Veterans and Service Members: A VA TBI Model Systems Study. J. Head Trauma Rehabil. 2017, 32, 234–244. [Google Scholar] [CrossRef] [PubMed]
- Ayotte, B.J.; Yang, F.M.; Jones, R.N. Physical Health and Depression: A Dyadic Study of Chronic Health Conditions and Depressive Symptomatology in Older Adult Couples. J. Gerontol. 2010, 65, 438–448. [Google Scholar] [CrossRef] [Green Version]
- Thomeer, M.B. Multiple chronic conditions, spouse’s depressive symptoms, and gender within marriage. J. Health Soc. Behav. 2016, 57, 59–76. [Google Scholar] [CrossRef]
- Trygged, S.; Hedlund, E.; Kåreholt, I. Education and poststroke separation among couples with mutual children. J. Divorce Remarriage 2001, 52, 401–414. [Google Scholar] [CrossRef]
- Kreutzer, J.S.; Marwitz, J.H.; Hsu, N.; Williams, K.; Riddick, A. Marital stability after brain injury: An investigation and analysis. NeuroRehabilitation 2007, 22, 53–59. [Google Scholar] [CrossRef]
- Tooth, L.; Mckenna, K.; Barnett, A.; Prescott, C.; Murphy, S. Caregiver burden, time spent caring and health status in the first 12 months following stroke. Brain Inj. 2005, 19, 963–974. [Google Scholar] [CrossRef] [PubMed]
- Marshall, C.A.; Nalder, E.; Colquhoun, H.; Lenton, E.; Hansen, M.; Dawson, D.R.; Zabjek, K.; Bottari, C. Interventions to address burden among family caregivers of persons aging with TBI: A scoping review. Brain Inj. 2019, 33, 255–265. [Google Scholar] [CrossRef] [PubMed]
- Riley, G.A. The partner’s experience of traumatic brain injury and its recovery. Future Med. 2016, 1. [Google Scholar] [CrossRef] [Green Version]
- Liu, Q.; Wang, X.; Wang, Y.; Wang, C.; Zhao, X.; Liu, L. Association between marriage and outcomes in patients with acute ischemic stroke. J. Neurol. 2018, 265, 942–948. [Google Scholar] [CrossRef] [Green Version]
- Martin, S.C. Relational issues within couples coping with Parkinson’s disease: Implications and ideas for family-focused care. J. Fam. Nurs. 2016, 22, 224–251. [Google Scholar] [CrossRef] [PubMed]
- King, K.B.; Reis, H.T. Marriage and long-term survival after coronary artery bypass grafting. Health Psychol. 2012, 31, 55–62. [Google Scholar] [CrossRef]
- Aizer, A.A.; Chen, M.H.; McCarthy, E.P.; Mendu, M.L.; Koo, S.; Wilhite, T.J. Marital status and survival in patients with cancer. J. Clin. Oncol. 2013, 31, 3869–3876. [Google Scholar] [CrossRef]
- Kim, D. Relationships between Caregiving Stress, Depression, and Self-Esteem in Family Caregivers of Adults with a Disability. Occup. Ther. Int. 2017, 2017, 1686143. [Google Scholar] [CrossRef]
- Quinn, K.; Murray, C.D.; Malone, C. Spousal experiences of coping with and adapting to caregiving for a partner who has a stroke: A meta-synthesis of qualitative. Disabil. Rehabil. 2014, 36, 185–198. [Google Scholar] [CrossRef] [PubMed]
- Arango-Lasprilla, J.C.; Ketchum, J.M.; Dezfulian, T.; Kreutzer, J.S.; O’Neil-Pirozzi, T.M.; Hammond, F.; Jha, A. Predictors of marital stability 2 years following traumatic brain injury. Brain Inj. 2008, 22, 565–574. [Google Scholar] [CrossRef]
- Karney, B.R.; Cown, J.S. Families under Stress: An Assessment of Data, Theory, and Research on Marriage and Divorce in Military; RAND Corporation: Santa Monia, CA, USA, 2007. [Google Scholar]
- Gentili, P.; Contreras, L.; Cassaniti, M.; D’Arista, F. La Dyadic Adjustment Scale. Una misura dell’adattamento di coppia. Minerva Psichiatr. 2002, 43, 107–116. [Google Scholar]
- Margola, D.; Fenaroli, V.; Sorgente, A.; Lanz, M.; Costa, G. The Family Relationships Index (FRI): Multilevel confirmatory factor analysis in an Italian community sample. Eur. J. Psychol. Assess. 2019, 35, 335–345. [Google Scholar] [CrossRef]
- Kieffer-Kristensen, R.; Teasdale, T.W. Parental stress and marital relationships among patients with brain injury and their spouses. NeuroRehabilitation 2011, 28, 321–330. [Google Scholar] [CrossRef] [PubMed]
- Bonanno, G.A. Loss, trauma, and human resilience: Have we underestimated the human capacity to thrive after extremely aversive events? Am. Psychol. 2004, 59, 20–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kitzmüller, G.; Asplund, K.; Häggström, T. The long-term experience of family life after stroke. J. Neurosci. Nurs. 2012, 44, E1–E13. [Google Scholar] [CrossRef]
- Jaracz, K.; Grabowska-Fudala, B.; Górna, K.; Jaracz, J.; Moczko, J.; Kozubski, W. Burden in caregivers of long-term stroke survivors: Prevalence and determinants at 6 months and 5 years after stroke. Patient Educ. Couns. 2015, 98, 1011–1016. [Google Scholar] [CrossRef]
- Nir, Z.; Greenberger, C.; Bachner, Y.G. Profile, burden, and quality of life of IIsraeli stroke survivor caregivers: A longitudinal study. J. Neurosci. Nurs. 2009, 41, 92–105. [Google Scholar] [CrossRef] [PubMed]
- Nunnari, D.; Bramanti, P.; Marino, S. Cognitive reserve in stroke and traumatic brain injury patients. Neurol. Sci. 2014, 35, 1513–1518. [Google Scholar] [CrossRef] [PubMed]
- Stern, Y. What is cognitive reserve? Theory and research application of the reserve concept. J. Int. Neuropsychol. Soc. 2002, 8, 448–460. [Google Scholar] [CrossRef]
- Schneider, E.B.; Sur, S.; Raymont, V.; Duckworth, J.; Kowalski, R.G.; Efron, D.T.; Hui, X.; Selvarajah, S.; Hambridge, H.L.; Stevens, R.D. Functional recovery after moderate/severe traumatic brain injury: A role for cognitive reserve? Neurology 2014, 82, 1636–1642. [Google Scholar] [CrossRef] [Green Version]
- Bijttebier, P.; Delva, D.; Vanoost, S.; Bobbaers, H.; Lauwers, P.; Vertommen, H. Reliability and Validity of the Critical Care Family Needs Inventory in a Dutch-speaking Belgian sample. Heart Lung J. Acute Crit. Care 2000, 29, 278–286. [Google Scholar] [CrossRef] [Green Version]
- Turner, B.; Fleming, J.; Parry, J.; Vromans, M.; Cornwell, P.; Gordon, C.; Ownsworth, T. Caregivers of Adults with Traumatic Brain Injury: The Emotional Impact of Transition From Hospital to Home. Brain Impair. 2010, 11, 281–292. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; Zhang, X.-N.; Zhang, H.-L.; Huang, L.; Chi, Q.-Q.; Zhang, X.; Yun, X.-P. Differences in cognitive profiles between traumatic brain injury and stroke: A comparison of the Montreal Cognitive Assessment and Mini-Mental State Examination. Chin. J. Traumatol. 2016, 19, 271–274. [Google Scholar] [CrossRef]
- George, L.K.; Ellison, C.G.; Larson, D.B. Explaining the relationships between religious involvement and health. Psychol. Inq. 2002, 13, 190–200. [Google Scholar] [CrossRef]
- Corallo, F.; Bonanno, L.; Buono, V.L.; De Salvo, S.; Rifci, C.; Bramanti, A. Religious Coping in Caregiver of Patients with Acquired Brain Injuries. J. Relig. Health 2019, 58, 1444–1452. [Google Scholar] [CrossRef] [PubMed]
- Yoon, K.H.; Moon, Y.S.; Lee, Y.; Choi, S.H.; Moon, S.Y.; Seo, S.W.; Park, K.W.; Ku, B.D.; Han, H.J.; Park, K.H.; et al. The moderating effect of religiosity on caregiving burden and depressive symptoms in caregivers of patients with dementia. Aging Ment. Health 2018, 22, 141–147. [Google Scholar] [CrossRef]
- Sakineh, G.; Tengku Aizan, H.; Hamidon, B.; Farkhondeh, S.; Rahimah, I. Religious coping and psychological well-being among Iranian stroke caregivers. Iran. J. Nurs. Midwifery Res. 2014, 19, 478–484. [Google Scholar]
- Koenig, H.G. Religion, spirituality, and health: The research and clinical implications. ISRN Psychiatry 2012, 2012, 278730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pierce, L.L.; Steiner, V.; Havens, H.; Tormoehlen, K. Spirituality Expressed by Caregivers of Stroke Survivors. West. J. Nurs. Res. 2008, 30, 606–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanks, R.A.; Boileau, N.R.; Norman, A.L.; Nakase-Richardson, R.; Mariouw, K.H.; Carlozzi, N.E. Spirituality and outcomes in caregivers of persons with traumatic brain injury (TBI). Rehabil. Psychol. 2020, 65, 347–359. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Clinical Variables | Values (Mean ±SD/Percentage) |
|---|---|
| Barthel Index at discharge | 61 ± 23.7 |
| ABI phenotype | • 57% Vascular • 43% Traumatic |
| Brain lesion localization | • 44% Frontal Lobe • 34% Temporal Lobe • 7% Parietal Lobe • 15% Occipital Lobe |
| Hemispheric lesion (% left) | 46% left |
| Variables | Patients | Spouses | p-Value |
|---|---|---|---|
| Demographic | |||
| Age (years) | 57.5 ± 1.7 | 55.7 ± 11.1 | 0.44 § |
| Educational level | 14% elementary school 32% middle school 37% high school 17% university | 11% elementary school 29% middle school 37% high school 23% university | 0.22 * |
| Job employment (Y/N) | 71% no | 51% no | 0.15 * |
| Spiritual orientation (Y/N) | 8% no | 5% no | 0.56 * |
| Religious commitment | 25% never 28% rarely 34% often 13% very often | 15% never 28% rarely 39% often 18% very often | 0.22 * |
| Psychological | |||
| FRI at discharge | 9.2 ± 2.8 | 9.4 ± 2.4 | 0.75 § |
| FRI after 2 years | 9.4 ± 2.7 | 9.6 ± 2.2 | 0.74 § |
| DAS at discharge | 109.8 ± 14.1 | 109.5 ± 16.1 | 0.93 § |
| DAS after 2 years | 108.6 ± 17.4 | 106.7 ± 16.9 | 0.64 § |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laratta, S.; Giannotti, L.; Tonin, P.; Calabrò, R.S.; Cerasa, A. Marital Stability and Quality of Couple Relationships after Acquired Brain Injury: A Two-Year Follow-Up Clinical Study. Healthcare 2021, 9, 283. https://doi.org/10.3390/healthcare9030283
Laratta S, Giannotti L, Tonin P, Calabrò RS, Cerasa A. Marital Stability and Quality of Couple Relationships after Acquired Brain Injury: A Two-Year Follow-Up Clinical Study. Healthcare. 2021; 9(3):283. https://doi.org/10.3390/healthcare9030283
Chicago/Turabian StyleLaratta, Stefania, Lucia Giannotti, Paolo Tonin, Rocco Salvatore Calabrò, and Antonio Cerasa. 2021. "Marital Stability and Quality of Couple Relationships after Acquired Brain Injury: A Two-Year Follow-Up Clinical Study" Healthcare 9, no. 3: 283. https://doi.org/10.3390/healthcare9030283