
Can Traditional Chinese Medicine Diagnosis Be Parameterized and Standardized? A Narrative Review

 ,
,  ,
,  and
and
Abstract
:1. Introduction
- A rational communicable theory;
- Scientific proof of efficacy and safety;
- Measures of quality control.
2. Tongue Diagnosis
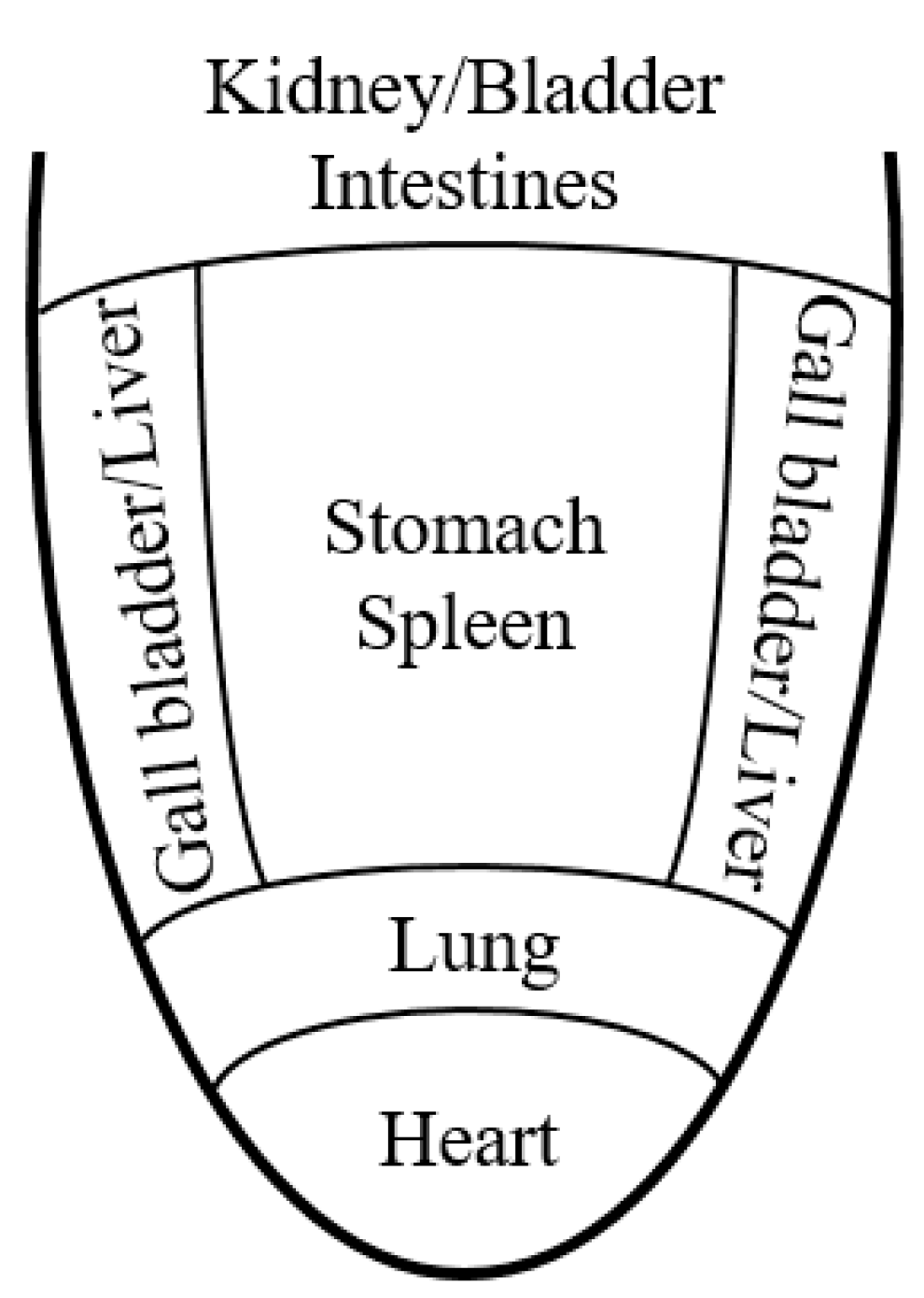
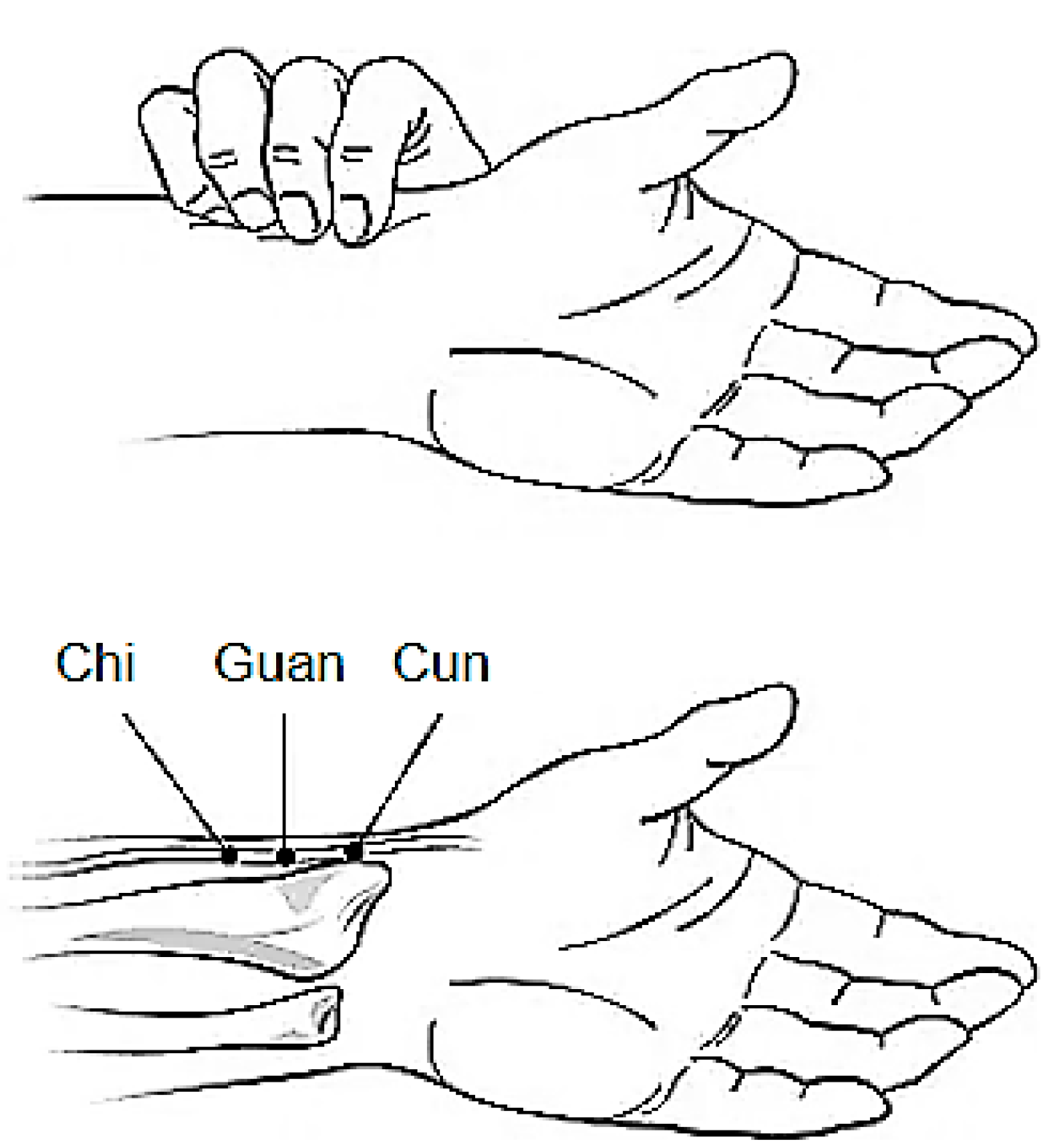
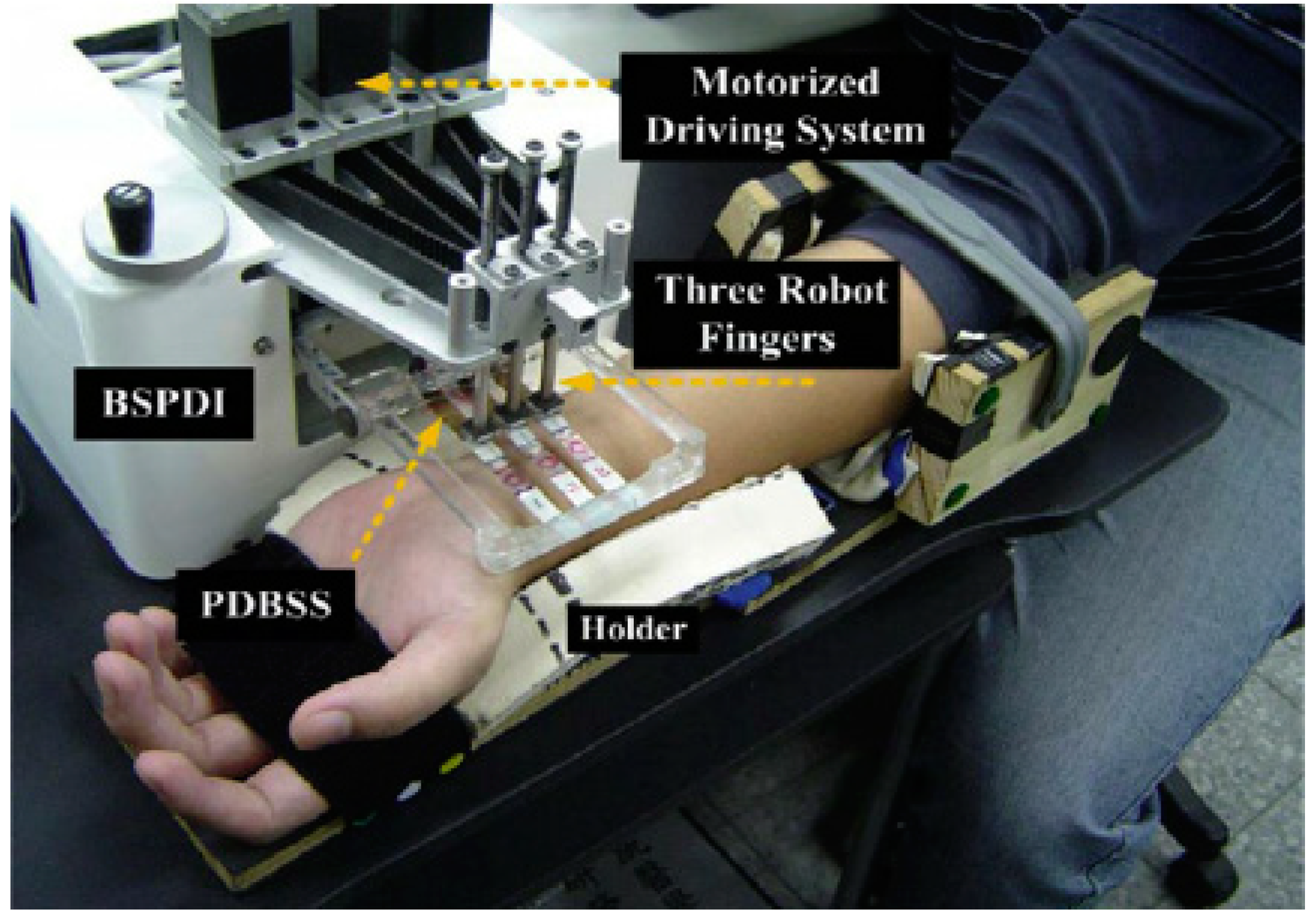
3. Pulse Diagnosis
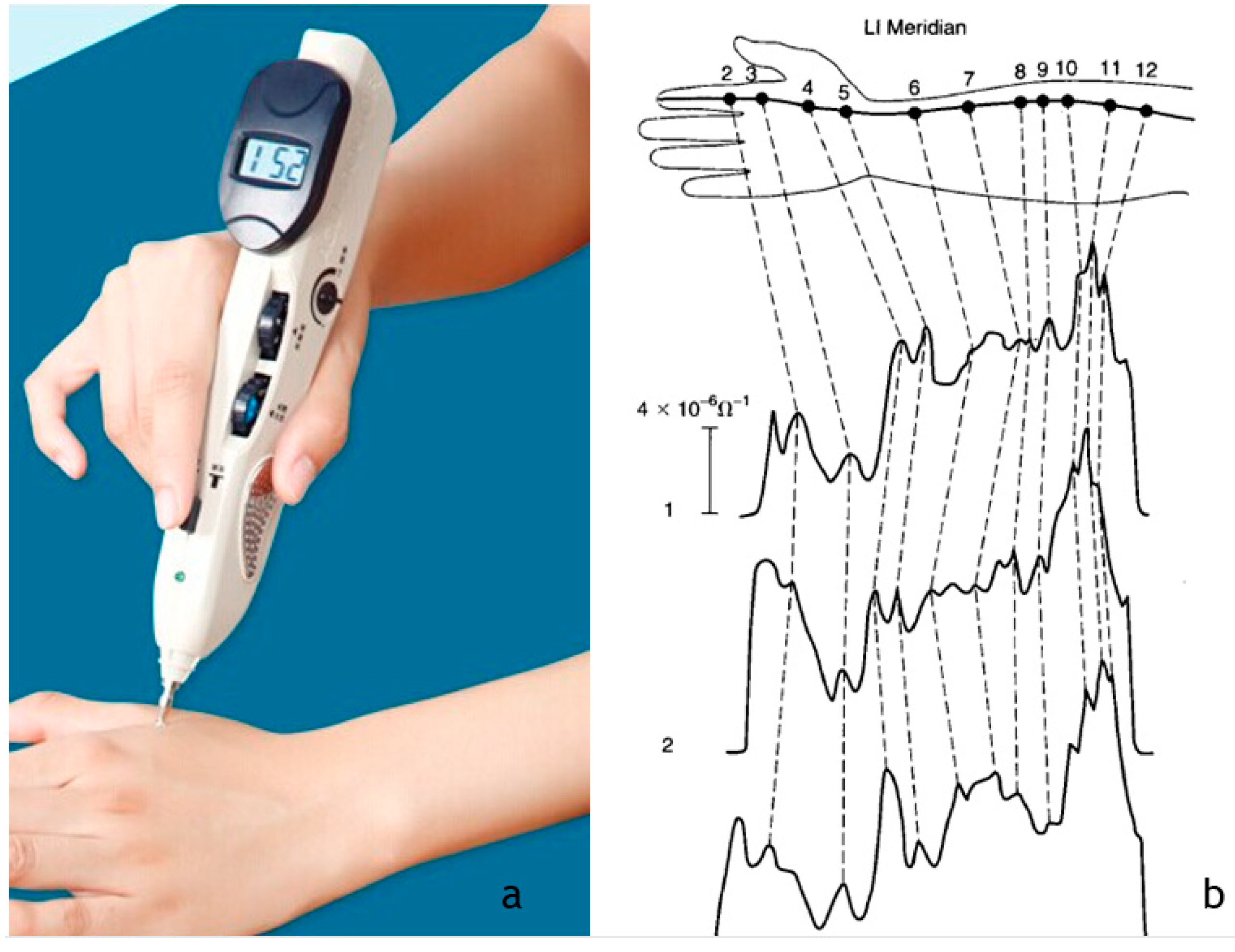
4. Electrophysiological Diagnosis Devices
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, Y.H.; Xu, A.L. Zheng: A systems biology approach to diagnosis and treatments. Science 2014, 346, S13–S15. [Google Scholar]
- Leung, E.L.-H.; Wong, V.K.-W.; Jiang, Z.-H.; Li, T.; Liu, L. Integrated network-based medicine: The role of traditional Chinese medicine in developing a new generation of medicine. Science 2014, 346, S16–S18. [Google Scholar]
- Vickers, A.J.; Cronin, A.M.; Maschino, A.C.; Lewith, G.; MacPherson, H.; Foster, N.E.; Sherman, K.J.; Witt, C.M.; Linde, K.; Collaboration, A.T. Acupuncture for chronic pain: Individual patient data meta-analysis. Arch. Intern. Med. 2012, 172, 1444–1453. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.-J.; Chen, H.-Y.; Yip, K.-c.; Ng, R.; Wong, V.T. The effectiveness and safety of acupuncture therapy in depressive disorders: Systematic review and meta-analysis. J. Affect. Disord. 2010, 124, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.-Y.; Shim, S.-R.; Rhee, H.Y.; Park, H.-J.; Jung, W.-S.; Moon, S.-K.; Park, J.-M.; Ko, C.-N.; Cho, K.-H.; Park, S.-U. Effectiveness of acupuncture and bee venom acupuncture in idiopathic Parkinson's disease. Parkinsonism Relat. Disord. 2012, 18, 948–952. [Google Scholar] [CrossRef] [PubMed]
- Cheong, K.B.; Zhang, J.-P.; Huang, Y. The effectiveness of acupuncture in postoperative gastroparesis syndrome—A systematic review and meta-analysis. Complementary Ther. Med. 2014, 22, 767–786. [Google Scholar] [CrossRef]
- Shi, H.; Fang, J.-q.; Li, B.-w.; Cong, W.-j.; Zhang, Y.; Chen, L. Efficacy assessment for different acupuncture therapies in the treatment of frozen shoulder. World J. Acupunct. Moxibustion 2012, 22, 6–11. [Google Scholar] [CrossRef]
- Law, D.; McDonough, S.; Bleakley, C.; Baxter, G.D.; Tumilty, S. Laser Acupuncture for Treating Musculoskeletal Pain: A Systematic Review with Meta-analysis. J. Acupunct. Meridian Stud. 2015, 8, 2–16. [Google Scholar] [CrossRef] [Green Version]
- Matos, L.; Goncalves, M.; Silva, A.; Mendes, J.; Machado, J.; Greten, H. Assessment of Qigong-related effects by infrared thermography: A case study. J. Chin. Integr. Med. 2012, 10, 663–666. [Google Scholar] [CrossRef]
- Zeng, Y.; Luo, T.; Xie, H.; Huang, M.; Cheng, A.S. Health benefits of qigong or tai chi for cancer patients: A systematic review and meta-analyses. Complementary Ther. Med. 2014, 22, 173–186. [Google Scholar] [CrossRef]
- Lee, M.S.; Pittler, M.H.; Ernst, E. Internal Qigong for Pain Conditions: A Systematic Review. J. Pain 2009, 10, 1121–1127. [Google Scholar] [CrossRef]
- Matos, L.C.; Sousa, C.M.; Gonçalves, M.; Gabriel, J.; Machado, J.; Greten, H.J. Qigong as a Traditional Vegetative Biofeedback Therapy: Long-Term Conditioning of Physiological Mind-Body Effects. Biomed Res. Int. 2015, 2015. [Google Scholar] [CrossRef] [Green Version]
- Cardoso, R.; Lumini-Oliveira, J.A.; Santos, M.J.; Ramos, B.; Matos, L.C.; Machado, J.; Greten, H.J.; Franconi, G. Acupuncture can be beneficial for exercise-induced muscle soreness: A randomised controlled trial. J. Bodyw. Mov. Ther. 2020, 24, 8–14. [Google Scholar] [CrossRef]
- Chan, S.; Ferreira, S.; Ramos, B.; Santos, M.J.; Matos, L.C.; Machado, J. Assessment of Acupuncture and Moxibustion Effects on the Electrophysiological Properties of the Ulnar Nerve: A Nerve Conduction Study. Integr. Med. Int. 2017, 4, 198–207. [Google Scholar] [CrossRef]
- Duarte, L.; Gonçalves, M.; Mendes, P.; Matos, L.C.; Greten, H.J.; Machado, J. Can Qigong improve attention in adolescents? A prospective randomised controlled trial. J. Bodyw. Mov. Ther. 2020, 24, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, J.M.S.; Mestre, M.I.C.; Matos, L.C.; Machado, J.P. Effects of taijiquan and qigong practice over behavioural disorders in school-age children: A pilot study. J. Bodyw. Mov. Ther. 2019, 23, 11–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chae, Y.; Chang, D.-S.; Lee, S.-H.; Jung, W.-M.; Lee, I.-S.; Jackson, S.; Kong, J.; Lee, H.; Park, H.-J.; Lee, H.; et al. Inserting Needles Into the Body: A Meta-Analysis of Brain Activity Associated With Acupuncture Needle Stimulation. J. Pain 2013, 14, 215–222. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.; Hu, X.-Y.; Razmovski-Naumovski, V.; Robinson, N. Challenges and opportunities of integrating traditional Chinese medicine into mainstream medicine: A review of the current situation. Eur. J. Integr. Med. 2015, 7, 67–75. [Google Scholar] [CrossRef]
- Greten, H.J. What is the role of Chinese medical theory in modern scientific research. J. Acupunct. Tuina Sci. 2008, 6, 259–260. [Google Scholar] [CrossRef]
- Greten, H.J. Chinese medicine as vegetative systems biology: Part I: Therapeutic methods. HNO 2011, 59, 1160–1164. [Google Scholar] [CrossRef]
- Greten, H.J. Chinese medicine as vegetative systems biology: Part II: The structure of TCM diagnosis. HNO 2011, 59, 1165–1175. [Google Scholar] [CrossRef]
- Karner, M.; Brazkiewicz, F.; Remppis, A.; Fischer, J.; Gerlach, O.; Stremmel, W.; Subramanian, S.V.; Greten, H.J. Objectifying Specific and Nonspecific Effects of Acupuncture: A Double-Blinded Randomised Trial in Osteoarthritis of the Knee. Evid. Based Complementary Altern. Med. 2013, 2013, 7. [Google Scholar] [CrossRef]
- Maimer, A.; Remppis, A.; Sack, F.-U.; Ringes-Lichtenberg, S.; Greten, T.; Brazkiewicz, F.; Schröder, S.; Goncalves, M.; Efferth, T.; Greten, H.J.; et al. Objectifying Acupuncture Effects by Lung Function and Numeric Rating Scale in Patients Undergoing Heart Surgery. Evid. Based Complementary Altern. Med. 2013, 2013, 7. [Google Scholar] [CrossRef] [Green Version]
- O'Brien, K.A.; Birch, S. A review of the reliability of traditional East Asian medicine diagnoses. J. Altern. Complementary Med. 2009, 15, 353–366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O'Brien, K.A.; Abbas, E.; Zhang, J.; Guo, Z.-X.; Luo, R.; Bensoussan, A.; Komesaroff, P.A. Understanding the reliability of diagnostic variables in a Chinese medicine examination. J. Altern. Complementary Med. 2009, 15, 727–734. [Google Scholar] [CrossRef]
- Lee, Y.-S.; Ryu, Y.; Yoon, D.-E.; Kim, C.-H.; Hong, G.; Hwang, Y.-C.; Chae, Y. Commonality and Specificity of Acupuncture Point Selections. Evid. Based Complementary Altern. Med. 2020, 2020, 2948292. [Google Scholar] [CrossRef] [PubMed]
- Madsen, M.V.; Gøtzsche, P.C.; Hróbjartsson, A. Acupuncture treatment for pain: Systematic review of randomised clinical trials with acupuncture, placebo acupuncture, and no acupuncture groups. BMJ 2009, 338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, S.-X.; Lee, P.C.; Anderson, T.L.; Li, X.-Y.; Jiang, I.Z. Response of Local Nitric Oxide Release to Manual Acupuncture and Electrical Heat in Humans: Effects of Reinforcement Methods. Evid. Based Complementary Altern. Med. 2017, 2017, 4694238. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Kang, D.-I. Positioning standardized acupuncture points on the whole body based on X-ray computed tomography images. Med. Acupunct. 2014, 26, 40–49. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Kang, D.-I. Partially Automated Method for Localizing Standardized Acupuncture Points on the Heads of Digital Human Models. Evid. Based Complementary Altern. Med. 2015, 2015, 483805. [Google Scholar] [CrossRef]
- Zhang, N.L.; Fu, C.; Liu, T.F.; Chen, B.X.; Poon, K.M.; Chen, P.X.; Zhang, Y.L. A data-driven method for syndrome type identification and classification in traditional Chinese medicine. J. Integr. Med. 2017, 15, 110–123. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.-S.; Ryu, Y.; Jung, W.-M.; Kim, J.; Lee, T.; Chae, Y. Understanding Mind-Body Interaction from the Perspective of East Asian Medicine. Evid. Based Complementary Altern. Med. 2017, 2017, 7618419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flaws, B.; Sionneau, P. The Treatment of Modern Western Medical Diseases with Chinese Medicine: A Textbook & Clinical Manual; Blue Poppy Enterprises, Inc.: Portland, OR, USA, 2001. [Google Scholar]
- Greten, H. Understanding TCM—Scientific Chinese Medicine—The Heidelberg Model; Course Version; Heidelberg School: Heidelberg, Germany, 2008. [Google Scholar]
- Jung, C.J.; Jeon, Y.J.; Kim, J.Y.; Kim, K.H. Review on the current trends in tongue diagnosis systems. Integr. Med. Res. 2012, 1, 13–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiu, C.-C. A novel approach based on computerized image analysis for traditional Chinese medical diagnosis of the tongue. Comput. Methods Programs Biomed. 2000, 61, 77–89. [Google Scholar] [CrossRef]
- Cui, Y.; Liao, S.; Wang, H. ROC-Boosting: A feature selection method for health identification using tongue image. Comput. Math. Methods Med. 2015, 2015, 362806. [Google Scholar] [CrossRef]
- Zhang, B.; Wang, X.; You, J.; Zhang, D. Tongue color analysis for medical application. Evid. Based Complementary Altern. Med. 2013, 2013, 264742. [Google Scholar] [CrossRef] [Green Version]
- Lo, L.-c.; Chen, Y.-F.; Chen, W.-J.; Cheng, T.-L.; Chiang, J.Y. The study on the agreement between automatic tongue diagnosis system and traditional Chinese medicine practitioners. Evid. Based Complementary Altern. Med. 2012, 2012, 505063. [Google Scholar] [CrossRef]
- Yu, S.; Yang, J.; Wang, Y.; Zhang, Y. Color Active Contour Models Based Tongue Segmentation in Traditional Chinese Medicine. In Proceedings of the 2007 1st International Conference on Bioinformatics and Biomedical Engineering, Wuhan, China, 6–8 July 2007. [Google Scholar]
- Bo, P.; Zhang, D.; Kuanquan, W. The bi-elliptical deformable contour and its application to automated tongue segmentation in Chinese medicine. IEEE Trans. Med Imaging 2005, 24, 946–956. [Google Scholar]
- Jia, W.; Yonghong, Z.; Jing, B. Tongue Area Extraction in Tongue Diagnosis of Traditional Chinese Medicine. In Proceedings of the 2005 IEEE Engineering in Medicine and Biology 27th Annual Conference, Shanghai, China, 1–4 September 2005. [Google Scholar]
- Wang, Y.; Zhou, Y.; Yang, J.; Xu, Q. An Image Analysis System for Tongue Diagnosis in Traditional Chinese Medicine. In Computational and Information Science: First International Symposium, CIS 2004, Shanghai, China, 16–18 December 2004, Proceedings; Zhang, J., He, J.-H., Fu, Y., Eds.; Springer: Berlin/Heidelberg, Germany, 2005; pp. 1181–1186. [Google Scholar]
- Wei, C.C.; Wang, C.H.; Huang, S.W. Using threshold method to separate the edge, coating and body of tongue in automatic tongue diagnosis. In The 6th International Conference on Networked Computing and Advanced Information Management; IEEE: New York, NY, USA, 2010. [Google Scholar]
- Lo, L.; Hou, M.; Chen, Y.; Chiang, J.; Hsu, C. Automatic tongue diagnosis system. In International Conference on Biomedical Engineering and Informatics; IEEE Press: Tianjin, China, 2009. [Google Scholar]
- Hsu, P.-C.; Huang, Y.-C.; Chiang, J.Y.; Chang, H.-H.; Liao, P.-Y.; Lo, L.-C. The association between arterial stiffness and tongue manifestations of blood stasis in patients with type 2 diabetes. BMC Complementary Altern. Med. 2016, 16, 324. [Google Scholar] [CrossRef] [Green Version]
- Chiu, C.-C.; Lan, C.-Y.; Chang, Y.-H. Objective assessment of blood stasis using computerized inspection of sublingual veins. Comput. Methods Programs Biomed. 2002, 69, 1–12. [Google Scholar] [CrossRef]
- Yan, Z.; Wang, K.; Li, N. Computerized feature quantification of sublingual veins from color sublingual images. Comput. Methods Programs Biomed. 2009, 93, 192–205. [Google Scholar] [CrossRef]
- Kim, J.; Han, G.-J.; Choi, B.-H.; Park, J.-W.; Park, K.; Yeo, I.-K.; Ryu, B.-H. Development of differential criteria on tongue coating thickness in tongue diagnosis. Complementary Ther. Med. 2012, 20, 316–322. [Google Scholar] [CrossRef]
- Kim, J.; Han, G.; Ko, S.-J.; Nam, D.-H.; Park, J.-W.; Ryu, B.; Kim, J. Tongue diagnosis system for quantitative assessment of tongue coating in patients with functional dyspepsia: A clinical trial. J. Ethnopharmacol. 2014, 155, 709–713. [Google Scholar] [CrossRef]
- Han, S.; Chen, Y.; Hu, J.; Ji, Z. Tongue images and tongue coating microbiome in patients with colorectal cancer. Microb. Pathog. 2014, 77, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Su, W.; Xu, Z.-y.; Wang, Z.-q.; Xu, J.-t. Objectified study on tongue images of patients with lung cancer of different syndromes. Chin. J. Integr. Med. 2011, 17, 272–276. [Google Scholar] [CrossRef]
- Lo, L.-C.; Cheng, T.-L.; Chiang, J.Y.; Damdinsuren, N. Breast cancer index: A perspective on tongue diagnosis in traditional chinese medicine. J. Tradit. Complementary Med. 2013, 3, 194–203. [Google Scholar] [CrossRef] [Green Version]
- Kanawong, R.; Obafemi-Ajayi, T.; Ma, T.; Xu, D.; Li, S.; Duan, Y. Automated tongue feature extraction for ZHENG classification in traditional Chinese medicine. Evid. Based Complementary Altern. Med. 2012, 2012, 912852. [Google Scholar] [CrossRef] [PubMed]
- Lo, L.-c.; Cheng, T.-L.; Chen, Y.-J.; Natsagdorj, S.; Chiang, J.Y. TCM tongue diagnosis index of early-stage breast cancer. Complementary Ther. Med. 2015, 23, 705–713. [Google Scholar] [CrossRef]
- Gareus, I.; Rampp, T.; Tan, L.; Luedtke, R.; Niggemeier, C.; Lauche, R.; Klose, P.; Dobos, G. Introducing a computer-assisted, digital tongue-imaging device for standardization of traditional tongue diagnosis. Forsch. Komplementärmedizin/Res. Complementary Med. 2014, 21, 190–196. [Google Scholar] [CrossRef]
- Lo, L.-c.; Chen, Y.-f.; Chiang, J.Y.; Cheng, T.-l.; Damdinsuren, N. Education of Chinese medicine tongue diagnosis by automatic tongue diagnosis system. Chin. J. Integr. Med. 2015, 1–10. [Google Scholar] [CrossRef]
- Hu, M.-C.; Cheng, M.-H.; Lan, K.-C. Color correction parameter estimation on the smartphone and its application to automatic tongue diagnosis. J. Med Syst. 2016, 40, 18. [Google Scholar] [CrossRef]
- Greten, H.J. Clinical Subjects, Scientific Chinese Medicine, The Heidelberg Model; Heidelberg School of Chinese Medicine: Heidelberg, Germany, 2008. [Google Scholar]
- Basicmedicalkey. Traditional Chinese Medicine: Pulse Diagnosis. 2017. Available online: https://basicmedicalkey.com/chinese-medicine-pulse-diagnosis/ (accessed on 20 January 2021).
- Bilton, K.; Hammer, L.; Zaslawski, C. Contemporary Chinese Pulse Diagnosis: A Modern Interpretation of an Ancient and Traditional Method. J. Acupunct. Meridian Stud. 2013, 6, 227–233. [Google Scholar] [CrossRef] [Green Version]
- Cassidy, C.M. Contemporary Chinese Medicine and Acupuncture; Churchill Livingstone: London, UK, 2002. [Google Scholar]
- Johnson, J.A.; Stewart, J.M.; Howell, M.H. Chinese Medical Qigong Therapy: A Comprehensive Clinical Guide; International Institute of Medical Qigong: Pacific Grove, CA, USA, 2000. [Google Scholar]
- Chu, Y.-W.; Luo, C.-H.; Chung, Y.-F.; Hu, C.-S.; Yeh, C.-C. Using an array sensor to determine differences in pulse diagnosis—Three positions and nine indicators. Eur. J. Integr. Med. 2014, 6, 516–523. [Google Scholar] [CrossRef]
- Tang, A.C.Y.; Chung, W.Y.J.; Wong, T.K.S. Validation of a novel traditional Chinese medicine pulse diagnostic model using an artificial neural network. Evid. Based Complementary Altern. Med. 2012, 2012, 685094. [Google Scholar] [CrossRef]
- Bilton, K.; Zaslawski, C. Reliability of Manual Pulse Diagnosis Methods in Traditional East Asian Medicine: A Systematic Narrative Literature Review. J. Altern. Complementary Med. 2016, 22, 599–609. [Google Scholar] [CrossRef]
- Chen, W.-S.; Yuan, S.-Y.; Liao, H.-E. Data compression for arterial pulse waveform. Am. J. Chin. Med. 2001, 29, 533–545. [Google Scholar] [CrossRef]
- Wang, H.; Cheng, Y. A quantitative system for pulse diagnosis in traditional Chinese medicine. In 2005 IEEE Engineering in Medicine and Biology 27th Annual Conference; IEEE: New York, NY, USA, 2006. [Google Scholar]
- Wang, H.-Y.; Zhang, P.-Y. A model for automatic identification of human pulse signals. J. Zhejiang Univ. Sci. A 2008, 9, 1382–1389. [Google Scholar] [CrossRef]
- Wang, H.-Y.; Zhang, P.-Y. Investigation on the automatic parameters extraction of pulse signals based on wavelet transform. J. Zhejiang Univ. Sci. A 2007, 8, 1283–1289. [Google Scholar] [CrossRef]
- Zhang, P.-Y.; Wang, H.-Y. A framework for automatic time-domain characteristic parameters extraction of human pulse signals. Eurasip J. Adv. Signal Process. 2008, 2008, 55. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Zhang, L.; Zhang, D.; Zhang, D. Wrist pulse signal diagnosis using modified Gaussian models and Fuzzy C-Means classification. Med. Eng. Phys. 2009, 31, 1283–1289. [Google Scholar] [CrossRef]
- Velik, R. An objective review of the technological developments for radial pulse diagnosis in Traditional Chinese Medicine. Eur. J. Integr. Med. 2015, 7, 321–331. [Google Scholar] [CrossRef]
- Shu, J.-J.; Sun, Y. Developing classification indices for Chinese pulse diagnosis. Complementary Ther. Med. 2007, 15, 190–198. [Google Scholar] [CrossRef] [Green Version]
- Xu, L.; Meng, M.Q.-H. Pulse images recognition using fuzzy neural network. Expert Syst. Appl. 2009, 36, 3805–3811. [Google Scholar] [CrossRef]
- Chung, Y.-F.; Hu, C.-S.; Yeh, C.-C.; Luo, C.-H. How to standardize the pulse-taking method of traditional Chinese medicine pulse diagnosis. Comput. Biol. Med. 2013, 43, 342–349. [Google Scholar] [CrossRef]
- Luo, C.-H.; Chung, Y.-F.; Hu, C.-S.; Yeh, C.-C.; Si, X.-C.; Feng, D.-H.; Lee, Y.-C.; Huang, S.-I.; Yeh, S.-M.; Liang, C.-H. Possibility of quantifying TCM finger-reading sensations: I. Bi-Sensing Pulse Diagnosis Instrument. Eur. J. Integr. Med. 2012, 4, e255–e262. [Google Scholar] [CrossRef]
- Chung, C.-Y.; Cheng, Y.-W.; Luo, C.-H. Neural network study for standardizing pulse-taking depth by the width of artery. Comput. Biol. Med. 2015, 57, 26–31. [Google Scholar] [CrossRef]
- Comunetti, A.; Laage, S.; Schiessl, N.; Kistler, A. Characterisation of human skin conductance at acupuncture points. Experientia 1995, 51, 328–331. [Google Scholar] [CrossRef] [PubMed]
- Pérez Samartín, A.L. Las propiedades eléctricas del punto de acupuntura: Una reflexión más. Rev. Int. De Acupunt. 2011, 5, 108–110. [Google Scholar] [CrossRef]
- Ahn, A.C.; Martinsen, Ø.G. Electrical characterization of acupuncture points: Technical issues and challenges. J. Altern. Complementary Med. 2007, 13, 817–824. [Google Scholar] [CrossRef] [Green Version]
- Turner, L.; Linden, W.; Talbot Ellis, A.; Millman, R. Measurement Reliability for Acupoint Activity Determined with the Prognos Ohmmeter. Appl. Psychophysiol. Biofeedback 2010, 35, 251–256. [Google Scholar] [CrossRef] [Green Version]
- Limited, L.T.C. Electric Acupuncture Stimulator with Acupoint Detector. 2015. Available online: http://leosensemedical.sale.enlightcorp.com (accessed on 25 January 2021).
- Spaulding, K.; Chamberlin, K. The Transport of Extremely Low-Frequency Electrical Signals Through an Acupuncture Meridian Compared to Nonmeridian Tissue. J. Altern. Complementary Med. 2011, 17, 127–132. [Google Scholar] [CrossRef]
- Lee, M.S.; Jeong, S.-Y.; Lee, Y.-H.; Jeong, D.-M.; Eo, Y.-G.; Ko, S.-B. Differences in electrical conduction properties between meridians and non-meridians. Am. J. Chin. Med. 2005, 33, 723–728. [Google Scholar] [CrossRef]
- Wong, F.W.S.; Lim, C.E.D.; Smith, W. A new bioimpedance research device (BIRD) for measuring the electrical impedance of acupuncture meridians. J. Altern. Complementary Med. 2010, 16, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.-B.; Lee, N.-R.; Shin, T.-M.; Lee, Y.-H. Development and Evaluation of a Multi-frequency Bioelectrical Impedance Analysis Analyzer for Estimating Acupoint Composition. J. Acupunct. Meridian Stud. 2014, 7, 33–43. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.-H.; Lee, M.S.; Shin, B.-C.; Jeong, J.-S.; Jeong, D.-M.; Hwang, I.C.; Kim, J.I. Effects of Acupuncture on Potential Along Meridians of Healthy Subjects and Patients with Gastric Disease. Am. J. Chin. Med. 2005, 33, 879–885. [Google Scholar] [CrossRef] [PubMed]
- Colbert, A.P.; Spaulding, K.; Larsen, A.; Ahn, A.C.; Cutro, J.A. Electrodermal activity at acupoints: Literature review and recommendations for reporting clinical trials. J. Acupunct. Meridian Stud. 2011, 4, 5–13. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.; Kim, S.; Son, T.; Kang, D.; Jung, B. Meridian electrical potential response to acupuncture stimulation between operator and subject. J. Acupunct. Meridian Stud. 2010, 3, 249–254. [Google Scholar] [CrossRef]
- Lee, Y.-H.; Ryu, Y.-H.; Jung, B. Investigation of Electrical Responses to Acupuncture Stimulation: The Effect of Electrical Grounding and Insulation Conditions. J. Acupunct. Meridian Stud. 2009, 2, 49–55. [Google Scholar] [CrossRef] [Green Version]
- Colbert, A.P.; Larsen, A.; Chamberlin, S.; Decker, C.; Schiffke, H.C.; Gregory, W.L.; Thong, T. A Multichannel System for Continuous Measurements of Skin Resistance and Capacitance at Acupuncture Points. J. Acupunct. Meridian Stud. 2009, 2, 259–268. [Google Scholar] [CrossRef] [Green Version]
- Xu, M.-M.; Guo, J.-K.; Xu, J.-S.; Zhang, C.-X.; Liu, S.-T.; Liao, R.-T.; Lin, C.-T.; Guo, J.-H.; Rao, P.-F. Monitoring the effects of acupoint antioxidant intervention by measuring electrical potential difference along the meridian. Evid. Based Complementary Altern. Med. 2015, 2015, 286986. [Google Scholar] [CrossRef]
- Kim, S.-B.; Shin, T.-M.; Lee, Y.-H. Development and evaluation of a bio-ion measurement system on acupoints for meridian diagnosis. J. Acupunct. Meridian Stud. 2013, 6, 110–118. [Google Scholar] [CrossRef]
- Pontarollo, F.; Rapacioli, G.; Bellavite, P. Increase of electrodermal activity of heart meridian during physical exercise: The significance of electrical values in acupuncture and diagnostic importance. Complementary Ther. Clin. Pract. 2010, 16, 149–153. [Google Scholar] [CrossRef]
- Matos, L.C.; Machado, J.; Greten, H.J.; Monteiro, F.J. Changes of skin electrical potential in acupoints from Ren Mai and Du Mai conduits during Qigong practice: Documentation of a clinical phenomenon. J. Bodyw. Mov. Ther. 2019, 23, 713–720. [Google Scholar] [CrossRef]
- Matos, L.C.; Lopes, L.T.; Freire, V.A.; Machado, J.P.; Monteiro, F.J.; Greten, H.J. Can the electrical potential of acupoints be used to assess the functional state of meridians and the effects of therapeutics? An exploratory data analysis. J. Bodyw. Mov. Ther. 2021, in press. [Google Scholar]
- Prokhorov, E.; Prokhorova, T.; González-Hernández, J.; Kovalenko, Y.A.; Llamas, F.; Moctezuma, S.; Romero, H. In vivo dc and ac measurements at acupuncture points in healthy and unhealthy people. Complementary Ther. Med. 2006, 14, 31–38. [Google Scholar] [CrossRef]
- Tseng, Y.-J.; Hu, W.-L.; Hung, I.-L.; Hsieh, C.-J.; Hung, Y.-C. Electrodermal screening of biologically active points for upper gastrointestinal bleeding. Am. J. Chin. Med. 2014, 42, 1111–1121. [Google Scholar] [CrossRef] [PubMed]
- Fico, T.; Duchon, F.; Dubravsky, J. Hardware and software realization of EDSD for acupuncture research and practice. IEEE J. Biomed. Health Inform. 2014, 18, 1207–1213. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.D.; Gau, J.T.; Wang, Y.H. Ryodoraku as a tool monitoring the effects of walking exercise. Zhong Xi Yi Jie He Xue Bao 2011, 9, 1319–1325. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.-T.; Chang, Y.-H.; Lin, W.-Y.; Xu, J.-M.; Chen, H.-Y.; Chou, P.-L.; Cheng, C.-W.; Chen, Y.-L.; Lin, F.-Y.; Tsai, F.-J.; et al. Applications of Meridian Electrical Conductance for Renal Colic: A Prospective Study. J. Altern. Complementary Med. 2010, 16, 861–866. [Google Scholar] [CrossRef] [Green Version]
- Tsai, M.-Y.; Kuo, C.-E.; Huang, Y.-C.; Hsieh, C.-L.; Chen, Y.-H.; Chen, W.-C. Meridian energy analysis of the immediate effect of coffee consumption. Eur. J. Integr. Med. 2014, 6, 74–81. [Google Scholar] [CrossRef]
- Su, D.; Liu, C.; Chiang, C.; Wang, W. Analysis of the Long-term Effect of Office Lighting Environment on Human Reponses. World Acad. Sci. Eng. Technol. 2012, 67, 332–339. [Google Scholar]
- Lin, M.L.; Wu, H.C.; Hsieh, Y.H.; Su, C.T.; Shih, Y.S.; Lin, C.W.; Wu, J.H. Evaluation of the effect of laser acupuncture and cupping with ryodoraku and visual analog scale on low back pain. Evid. Based Complementary Alternat. Med. 2012, 2012, 521612. [Google Scholar] [CrossRef]
- Leung, T.-K.; Lin, M.-T.; Chen, C.-A.; Hsu, C.-Y.; Lin, S.-L.; Chen, C.W. The analysis of normalized effects on meridian current level after the photoluminescent bioceramic treatment on acupuncture points. J. Altern. Complementary Med. 2015, 21, 472–479. [Google Scholar] [CrossRef]
- Weng, C.-S.; Hung, Y.-L.; Shyu, L.-Y.; Chang, Y.-H. A study of electrical conductance of meridian in the obese during weight reduction. Am. J. Chin. Med. 2004, 32, 417–425. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Wang, Q.; Liang, H.; Dong, H.; Li, Y.; Ng, E.H.Y.; Wu, X. Biophysical Characteristics of Meridians and Acupoints: A Systematic Review. Evid. Based Complementary Altern. Med. 2012, 2012, 793841. [Google Scholar] [CrossRef] [Green Version]
- Wong, Y.C.P. Need of integrated dietary therapy for persons with diabetes mellitus and “unhealthy” body constitution presentations. J. Integr. Med. 2016, 14, 255–268. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matos, L.C.; Machado, J.P.; Monteiro, F.J.; Greten, H.J. Can Traditional Chinese Medicine Diagnosis Be Parameterized and Standardized? A Narrative Review. Healthcare 2021, 9, 177. https://doi.org/10.3390/healthcare9020177
Matos LC, Machado JP, Monteiro FJ, Greten HJ. Can Traditional Chinese Medicine Diagnosis Be Parameterized and Standardized? A Narrative Review. Healthcare. 2021; 9(2):177. https://doi.org/10.3390/healthcare9020177
Chicago/Turabian StyleMatos, Luís Carlos, Jorge Pereira Machado, Fernando Jorge Monteiro, and Henry Johannes Greten. 2021. "Can Traditional Chinese Medicine Diagnosis Be Parameterized and Standardized? A Narrative Review" Healthcare 9, no. 2: 177. https://doi.org/10.3390/healthcare9020177