
Proton Therapy for Mandibula Plate Phantom

 , ,
, ,  , , , and
, , , and
Abstract
:1. Introduction
2. Material and Method
3. Results
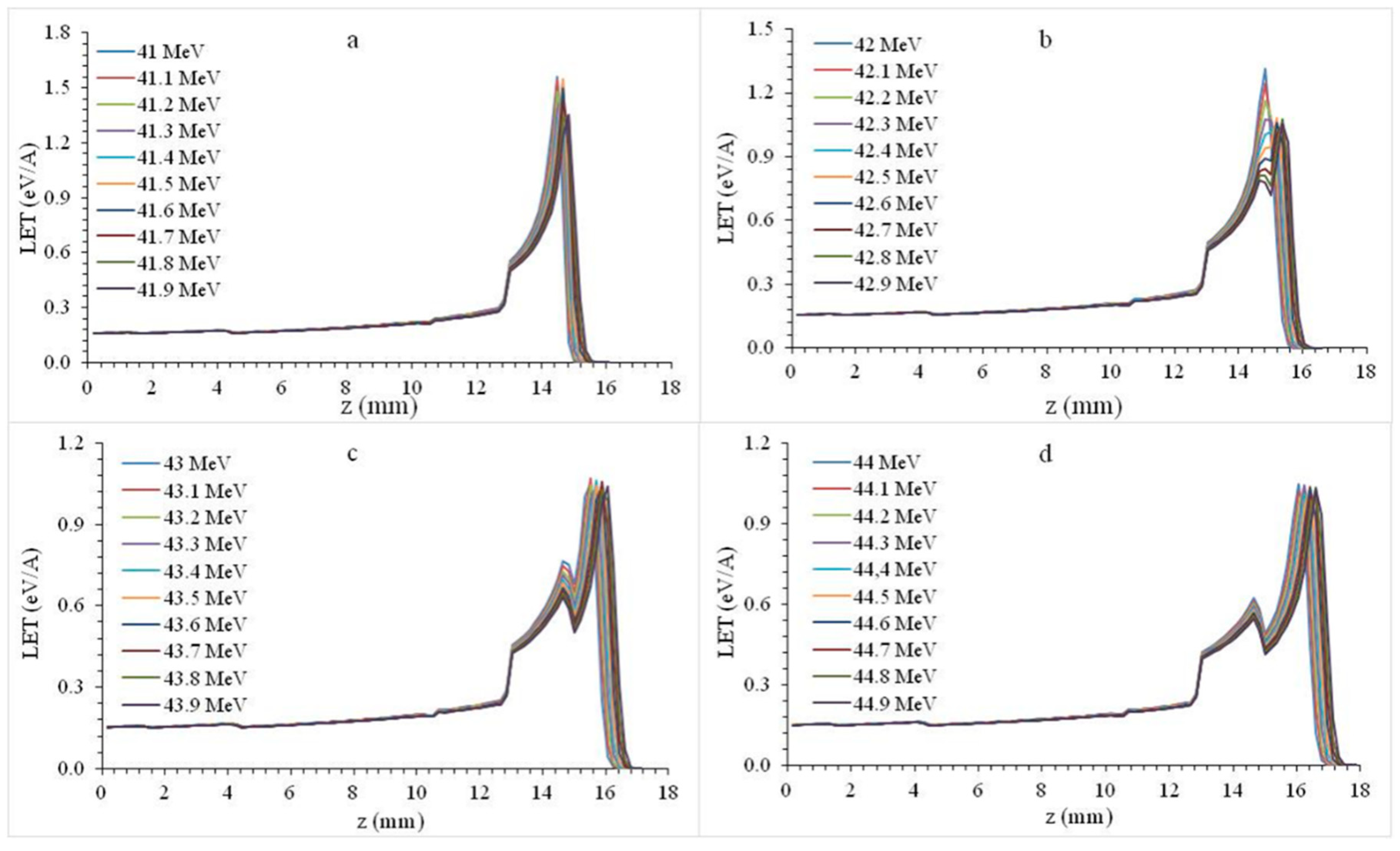
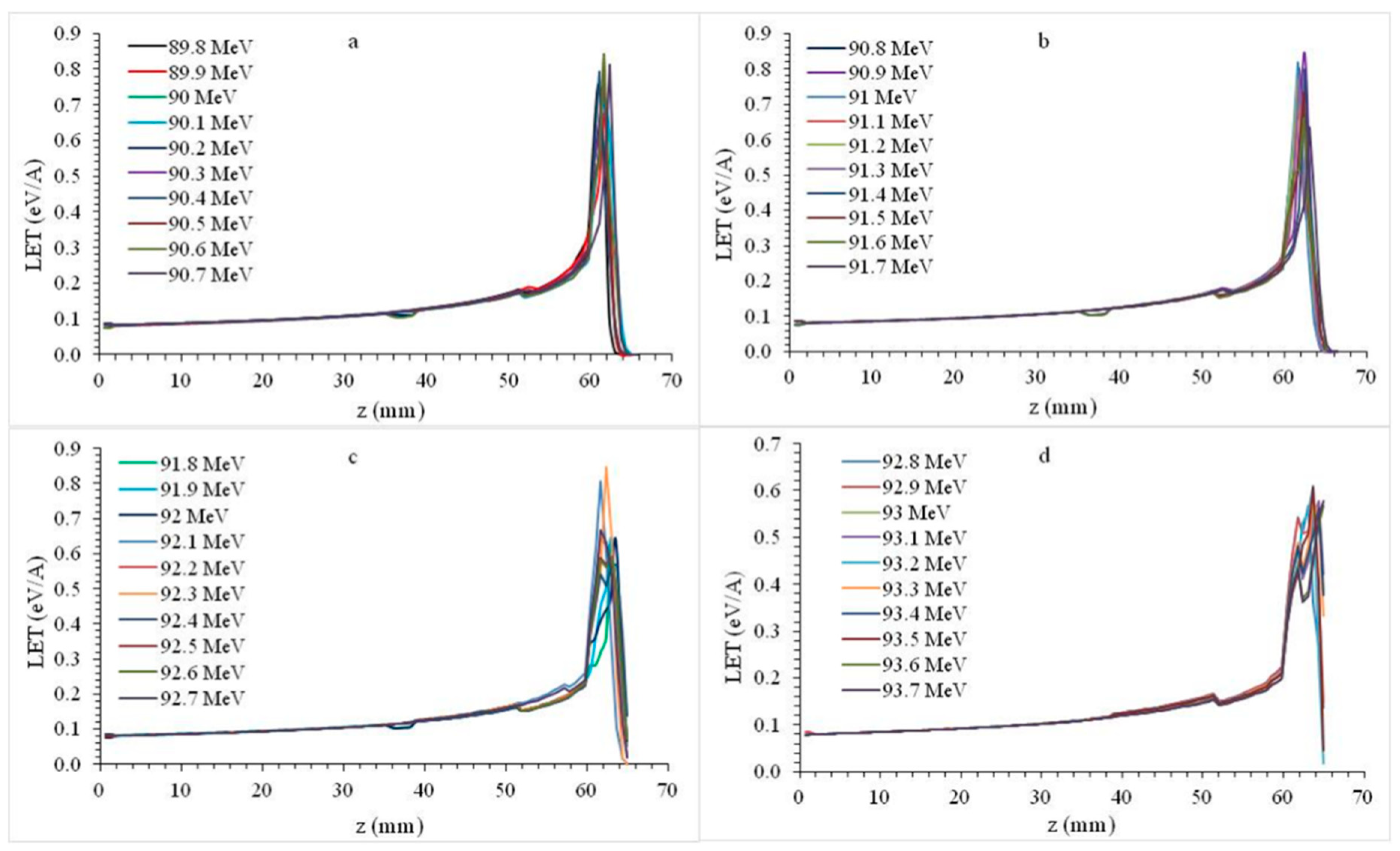
3.1. Bragg Peaks
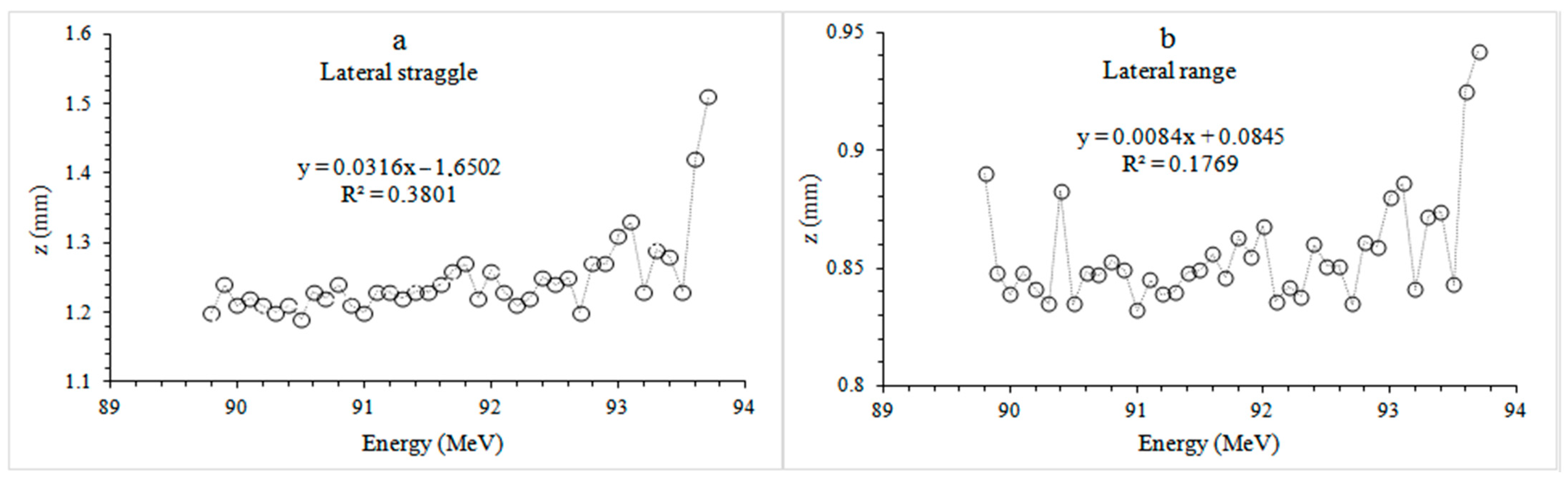
3.2. Lateral Range and Straggle
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wilson, R.R. Radiological Use of Fast Protons. Radiology 1946, 47, 487–491. [Google Scholar] [CrossRef]
- Lawrence, J.H.; Tobias, C.A.; Born, J.I.; Mccombs, R.K.; Roberts, J.E.; Anger, H.O. Pituitary irradiation with highenergy proton beams: A pre-liminary report. Cancer Res. 1958, 18, 121–134. [Google Scholar] [PubMed]
- Gragoudas, E.S.; Li, W.; Goitein, M.; Lane, A.M.; Munzenrider, J.E.; Egan, K.M. Evidence-Based Estimates of Outcome in Patients Irradiated for Intraocular Melanoma. Arch. Ophthalmol. 2002, 120, 1665–1671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gottschalk, B. Physics of proton interactions in matter. In Proton Therapy Physics; Pagannetti, H., Ed.; Taylor & Francis Inc.: Boca Raton, FL, USA, 2012; pp. 20–57. [Google Scholar]
- Carlsson, A.K.; Andrea, P.; Brahme, A. Monte Carlo and analytical calculation of computerized treatment plan optimization. Phys. Med. Biol 1997, 42, 1033–1053. [Google Scholar] [CrossRef] [PubMed]
- Hall, E.J.; Kellerer, A.M.; Rossi, H.H.; Lam, Y.-M.P. The relative biological effectiveness of 160 MeV protons-II. Int. Radiat. Oncol. Biol. Phys. 1978, 4, 1009–1013. [Google Scholar] [CrossRef] [Green Version]
- Li, J.S.; Shahine, B.; Fourkal, E.; Ma, C.-M. A particle track-repeating algorithm for proton beam dose calculation. Phys. Med. Biol. 2005, 50, 1001–1010. [Google Scholar] [CrossRef]
- Seravalli, E.; Robert, C.; Bauer, J.; Stichelbaut, F.; Kurz, C.; Smeets, J.; Ty, C.V.N.; Schaart, D.R.; Buvat, I.; Parodi, K.; et al. Monte Carlo calculations of positron emitter yields in proton radiotherapy. Phys. Med. Biol. 2012, 57, 1659–1673. [Google Scholar] [CrossRef]
- Kitagawa, A. Review on heavy ion radiotherapy and related ion sources. AIP Rev. Sci. Instrum. 2010, 81, 1–8. [Google Scholar]
- Jäkel, O. Ion Beam Science: Solved and Unsolved Problems. Invited Lectures Presented at A Symposium Arranged by the Royal Danish Academy of Sciences and Letters, Copenhagen, Denmark, 1–5 May 2006; Sigmund, P., Ed.; Karada Publishing Services (KPS): Nova Gorica, Slovenia, 2006; pp. 37–57. [Google Scholar]
- Jäkel, O. Medical physics aspects of particle therapy. Radiat. Prot. Dosim. 2009, 137, 156–166. [Google Scholar] [CrossRef] [Green Version]
- Cameron, J.C.; James, G.; Skofronick, J.G. Medical Physics; John Wiley & Sons: New York, NY, USA, 1978; pp. 1–10. [Google Scholar]
- Tokarek, R.; Bernstein, E.F.; Sullivan, F.; Uitto, J.; Mitchell, J.B.; Sullivan, F.J. Effect of therapeutic radiation on wound healing. Clin. Dermatol. 1994, 12, 57–70. [Google Scholar] [CrossRef]
- Schulz-Ertner, D.; Tsujii, H. Particle Radiation Therapy Using Proton and Heavier Ion Beams. J. Clin. Oncol. 2007, 25, 953–964. [Google Scholar] [CrossRef] [Green Version]
- McDonald, M.W.; Liu, Y.; Moore, M.G.; Johnstone, P.A. Acute toxicity in comprehensive head and neck radiation for nasopharynx and paranasal sinus cancers: Cohort comparisonof 3D conformal proton therapy and intensity modulated radiation therapy. Radiat. Oncol. 2016, 11, 32. [Google Scholar] [CrossRef] [Green Version]
- Romesser, P.B.; Cahlon, O.; Scher, E. Proton beam radiation therapy results in significantly reduced toxicity compared with intensi-ty-modulated radiation therapy for head and neck tumors that require ipsilateral radiation. Radiother. Oncol. 2016, 118, 286–292. [Google Scholar] [CrossRef] [Green Version]
- Parkins, G.E.; Armah, G.E.; Ampofo, P. Tumours and tumour-like lesions of the lower face at Korle Bu Teaching Hospital, Ghana—Sn eight year study. World J. Surg. Oncol. 2007, 5, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weber, A.L.; Bui, C.; Kaneda, T. Malignant tumors of the mandible and maxilla. Neuroimaging Clin. N. Am. 2003, 13, 509–524. [Google Scholar] [CrossRef]
- Koichi, M.; Yusuke, D.; Naoki, H.; Masayuki, M.; Kazuki, T.; Osamu, F.; Naoki, O.; Masao, M.; Nobukazu, F.; Ken-Ichi, N. Particle Radio-therapy Using Protons or Carbon Ions for Unresectable Locally Advanced Head and Neck Cancers with Skull Base Invasion. Jpn. J. Clin. Oncol. 2014, 44, 428–434. [Google Scholar]
- Alhadi, A.; Ibrahim, O.B.; Harri, K.S. Depth of invasion, tumor budding, and worst pattern of invasion: Prognostic indicators in ear-ly-stage oral tongue cancer. J. Oral Biol. Craniofac. Res. 2017, 7, 167–170. [Google Scholar]
- Brown, J.S.; Lowe, D.; Kalavrezos, N.; D’Souza, J.; Magennis, P.; Woolgar, J. Patterns of invasion and routes of tumor entry into the man-dible by oral squamous cell carcinoma. Head Neck 2002, 24, 370–383. [Google Scholar] [CrossRef] [PubMed]
- Loyola, A.M.; Cardoso, S.; De Faria, P.R.; Servato, J.P.S.; Eisenberg, A.L.; Dias, F.L.; Accioly, M.T.S.; Gomes, C.C.; Gomez, R.S.; Souza, S.O.M.C.; et al. Ameloblastic carcinoma: A Brazilian collaborative study of 17 cases. Histopathology 2016, 69, 687–701. [Google Scholar] [CrossRef] [PubMed]
- Ling, D.C.; Kabolizadeh, P.; Heron, D.E.; Ohr, J.P.; Wang, H.; Johnson, J.; Kubicek, G.J. Incidence of hospitalization in patients with head and neck cancer treated with intensity-modulated radiation therapy. Head Neck 2015, 37, 1750–1755. [Google Scholar] [CrossRef]
- Pignon, J.; Bourhis, J.; Domenge, C.; Designé, L. Chemotherapy added to locoregional treatment for head and neck squamous-cell car-cinoma: Three meta-analyses of updated individual data. Lancet 2000, 355, 949–955. [Google Scholar] [CrossRef]
- Katsura, K.; Sasai, K.; Sato, K.; Saito, M.; Hoshina, H.; Hayashi, T. Relationship between oral health status and development of osteora-dionecrosis of the mandible: A retrospective longitudinal study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2008, 105, 731–738. [Google Scholar] [CrossRef] [PubMed]
- Emami, B.; Lyman, J.; Brown, A.; Cola, L.; Goitein, M.; Munzenrider, J.; Shank, B.; Solin, L.; Wesson, M. Tolerance of normal tissue to therapeutic irradiation. Int. J. Radiat. Oncol. 1991, 21, 109–122. [Google Scholar] [CrossRef]
- Fujita, M.; Hirokawa, Y.; Kashiwado, K.; Akagi, Y.; Kashimoto, K.; Kiriu, H.; Ohtani, K.; Wada, T. An analysis of mandibular bone complications in radiotherapy for T1 and T2 carcinoma of the oral tongue. Int. J. Radiat. Oncol. 1996, 34, 333–339. [Google Scholar] [CrossRef]
- Mosel, D.D.; Bauer, R.L.; Lynch, D.P.; Hwang, S.T. Oral complications in the treatment of cancer patients. Oral Dis. 2011, 17, 550–559. [Google Scholar] [CrossRef]
- Nutting, C.M.; Morden, J.P.; Harrington, K.J.; Urbano, T.G.; Bhide, S.A.; Clark, C.; Miles, E.A.; Miah, A.B.; Newbold, K.; Tanay, M.; et al. Parotid-sparing intensity modulated versus conventional radiotherapy in head and neck cancer: A phase 3 multicentre randomised controlled trial. Lancet Oncol. 2011, 12, 127–136. [Google Scholar] [CrossRef] [Green Version]
- Kumar, R.; Madanikia, S.; Starmer, H.; Yang, W.; Murano, E.; Alcorn, S.; McNutt, T.; Le, Y.; Quon, H. Radiation dose to the floor of mouth muscles predicts swallowing complications following chemoradiation in oropharyngeal squamous cell carcinoma. Oral Oncol. 2014, 50, 65–70. [Google Scholar] [CrossRef]
- Rosenthal, D.I.; Chambers, M.S.; Fuller, C.D.; Rebueno, N.C.; Garcia, J.; Kies, M.S.; Morrison, W.H.; Ang, K.K.; Garden, A.S. Beam Path Toxicities to Non-Target Structures During Intensity-Modulated Radiation Therapy for Head and Neck Cancer. Int. J. Radiat. Oncol. 2008, 72, 747–755. [Google Scholar] [CrossRef]
- SRIM. Available online: http://www.srim.org/ (accessed on 18 June 2018).
- Samant, S.K.T.; Robbins, P.; Kumar, J.Z.; Ma, F.; Vieira, C.B.A. Hanchett Bone or cartilage invasion by advanced head and neck cancer: Intra-arterial supradose cisplatin chemotherapy and concomitant radiotherapy for organ preservation. Arch. Otolaryngol. Head Neck Surg. 2001, 127, 1451–1456. [Google Scholar] [CrossRef] [Green Version]
- Carroll, W.W. Combined neck and jaw resection for intraoral carcinoma. Surg. Gynecol. Obstet. 1952, 94, 1. [Google Scholar] [CrossRef] [PubMed]
- Latha, P.R.; Mridula, S.; Vinay, S.; Manoj, P. Mandibular conservation in oral cancer. Surg. Oncol. 2012, 21, 109–118. [Google Scholar]
- Konishi, M.; Suei, Y.; Fujita, M.; Tanimoto, K. Radiographic changes of the mandible after proton beam radiotherapy for oral cancer: A case report. Int. J. Case Rep. Images 2016, 8, 787–791. [Google Scholar] [CrossRef] [Green Version]
- Steneker, M.; Lomax, A.; Schneider, U. Intensity modulated photon and proton therapy for the treatment of head and neck tumors. Radiother. Oncol. 2006, 80, 263–267. [Google Scholar] [CrossRef]
- Morimoto, K.; Demizu, Y.; Hashimoto, N.; Mima, M.; Terashima, K.; Fujii, O.; Otsuki, N.; Murakami, M.; Fuwa, N.; Nibu, K.-I. Particle Radiotherapy Using Protons or Carbon Ions for Unresectable Locally Advanced Head and Neck Cancers with Skull Base Invasion†. Jpn. J. Clin. Oncol. 2014, 44, 428–434. [Google Scholar] [CrossRef] [Green Version]
- Van de Water, T.A.; Lomax, A.J.; Bijl, H.P.; de Jong, M.E.; Schilstra, C.; Hug, E.B.; Langendijk, J.A. Potential benefits of scanned intensity-modulated proton therapy versus advanced photon therapy with regard to sparing of the salivary glands in oropharyngeal cancer. Int. J. Radiat. Oncol. Biol. Phys. 2011, 71, 1216–1224. [Google Scholar] [CrossRef]
- Cozzi, L.; Fogliata, A.; Lomax, A.; Bolsi, A. A treatment planning comparison of 3D conformal therapy, intensity modulated photon therapy and proton therapy for treatment of advanced head and neck tumours. Radiother. Oncol. 2001, 61, 287–297. [Google Scholar] [CrossRef]
- Jakobi, A.; Bandurska-Luque, A.; Stützer, K.; Haase, R.; Löck, S.; Wack, L.-J.; Mönnich, D.; Thorwarth, D.; Perez, D.; Lühr, A.; et al. Identification of Patient Benefit from Proton Therapy for Advanced Head and Neck Cancer Patients Based on Individual and Subgroup Normal Tissue Complication Probability Analysis. Int. J. Radiat. Oncol. 2015, 92, 1165–1174. [Google Scholar] [CrossRef]
- Langendijk, J.; Lambin, P.; De Ruysscher, D.; Widder, J.; Bos, M.; Verheij, M. Selection of patients for radiotherapy with protons aiming at reduction of side effects: The model-based approach. Radiother. Oncol. 2013, 107, 267–273. [Google Scholar] [CrossRef] [Green Version]
- Van de Water, T.; Lomax, T.; Bij, H.P.; Schilstra, K.; Meertens, H.; Hug, E.; Langendijk, J. Comparative treatment planning study between scanned intensity modulated proton therapy and photon therapy in complex oropharyngeal carcinoma. Radiother. Oncol. 2008, 88, 77–78. [Google Scholar]
- Leeman, J.E.; Romesser, P.B.; Zhou, Y.; McBride, S.; Riaz, N.; Sherman, E.; Cohen, M.A.; Cahlon, O.; Lee, N. Proton therapy for head and neck cancer: Expanding the therapeutic window. Lancet Oncol. 2017, 18, e254–e265. [Google Scholar] [CrossRef]
- Ekinci, F.; Bölükdemir, M.H. The effect of the second peak formed in biomaterials used in a slab head phantom on the proton Bragg peak. J. Polytech. J. Polytech. 2020, 23, 129–136. [Google Scholar]
- Vogel, J.; Both, S.; Kirk, M.; Chao, H.-H.; Bagatell, R.; Zelig, T.; Womer, R.; Balamuth, N.; Reilly, A.; Kurtz, G.; et al. Proton therapy for pediatric head and neck malignancies. Pediatr. Blood Cancer 2018, 65, e26858. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
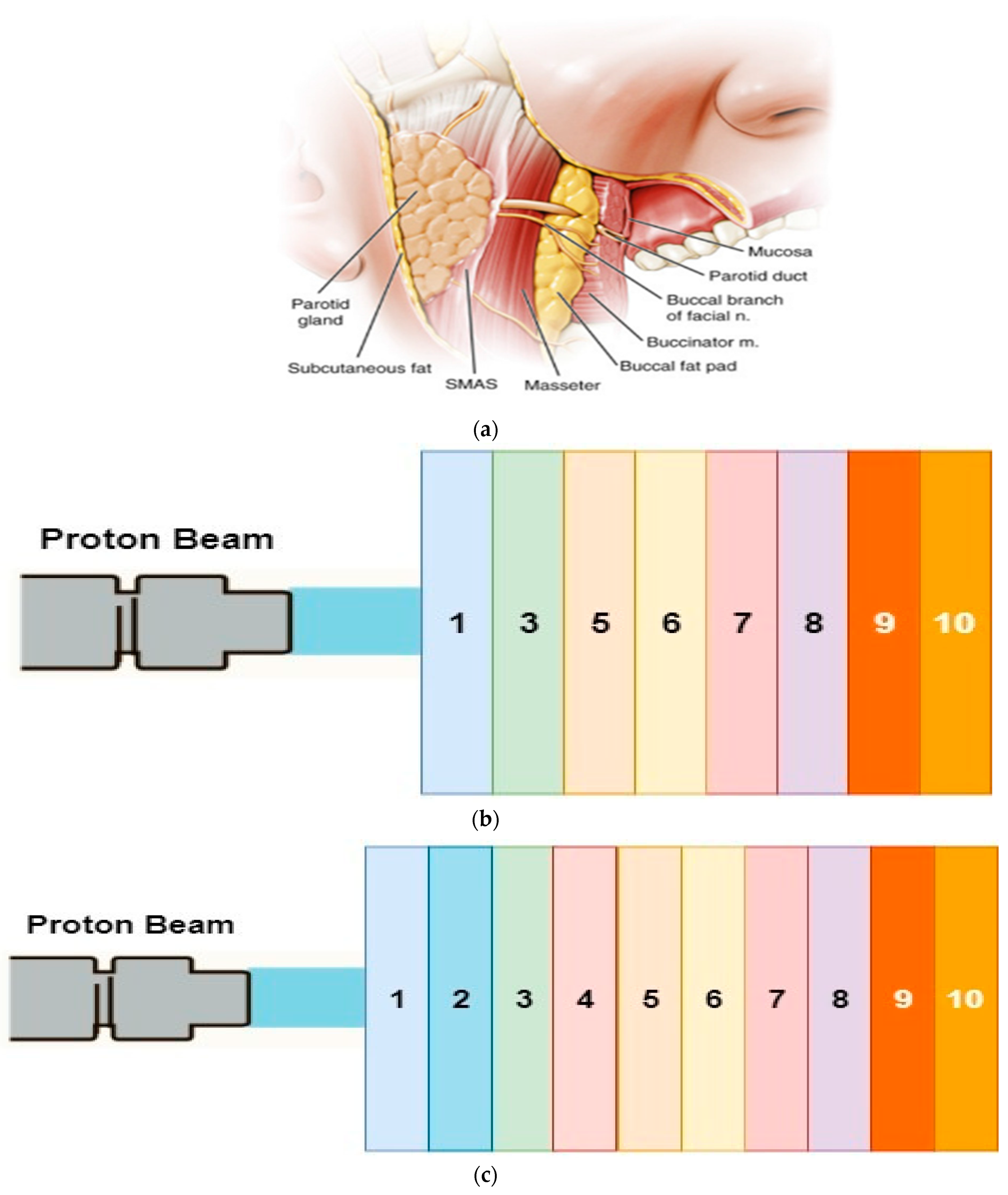
| Biomaterial | Chemical Composition (%) | Atomic Density (1022 atom/cm3) | Density (g/cm3) |
|---|---|---|---|
| 1. Skin | H 10; O 59.4; C 25; N 4.6; S 0.3; Cl 0.3; P 10.3; Na 0.2; K 0.1 | 9.88 | 1.02 |
| 2. Parotid gland | H 62.5; C 16.4; N 1.27; O19.6; S 0.037; Cl 0.016; Na 0.025; P 0.019 | 10.32 | 1.02 |
| 3. SMAS | H 58.3; C 37.4; N 1.45; O 1.89; F 0.532; Ca 0.266 | 10.65 | 1.027 |
| 4. Masseter muscle | H 52.6; C 8.9; N 1.6; O 26.6; S 5.85; Cl 1.76; K 0.64; P 0.404 | 10.11 | 1.05 |
| 5. Buccal Fat | H 63.4; C 28.4; N 0.304; O 7.77; Cl 0.018; Na 0.011 | 10.35 | 0.92 |
| 6. Mucosa | H 10.1; C 77.5; N 3.50; O 5.23; F 1.74;Ca 1.83 | 5.24 | 1.028 |
| 7. Saliva | H 66.6; O 33.3 | 10.02 | 1 |
| 8. Gum | H 52.6; C 32.9; N 0.862; O 7.89; Cl 1.72; Mg 3.63 | 8.88 | 1 |
| 9. Cortical bone | H 39.2; C 15; N 3.48; O 31.6; S 0.108; P 3.86; Ca 6.53; Mg 9.57 | 9.94 | 1.92 |
| 10. Cancellous bone | H 57.7; C 23; N 1.36; O 15.7; S 4.27; P 0.752; Ca 1.26; Fe 1.23 | 10.42 | 1.18 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Senirkentli, G.B.; Ekinci, F.; Bostanci, E.; Güzel, M.S.; Dağli, Ö.; Karim, A.M.; Mishra, A. Proton Therapy for Mandibula Plate Phantom. Healthcare 2021, 9, 167. https://doi.org/10.3390/healthcare9020167
Senirkentli GB, Ekinci F, Bostanci E, Güzel MS, Dağli Ö, Karim AM, Mishra A. Proton Therapy for Mandibula Plate Phantom. Healthcare. 2021; 9(2):167. https://doi.org/10.3390/healthcare9020167
Chicago/Turabian StyleSenirkentli, Güler Burcu, Fatih Ekinci, Erkan Bostanci, Mehmet Serdar Güzel, Özlem Dağli, Ahmad M. Karim, and Alok Mishra. 2021. "Proton Therapy for Mandibula Plate Phantom" Healthcare 9, no. 2: 167. https://doi.org/10.3390/healthcare9020167