
Challenges and Obstacles Faced by Trainee Female Physicians: An Integrative Research on Gender Discrimination, Stress, Depression and Harassment

 , and
, and
Abstract
:1. Introduction
- Assessment of the nature and extent of challenges faced by the female trainee physicians;
- Evaluation of the impact of these challenges on the mental, social and professional life of female trainee physicians;
- Recommendation of policy development to minimize the workplace challenges faced by female physicians.
2. Materials and Methods
3. Results
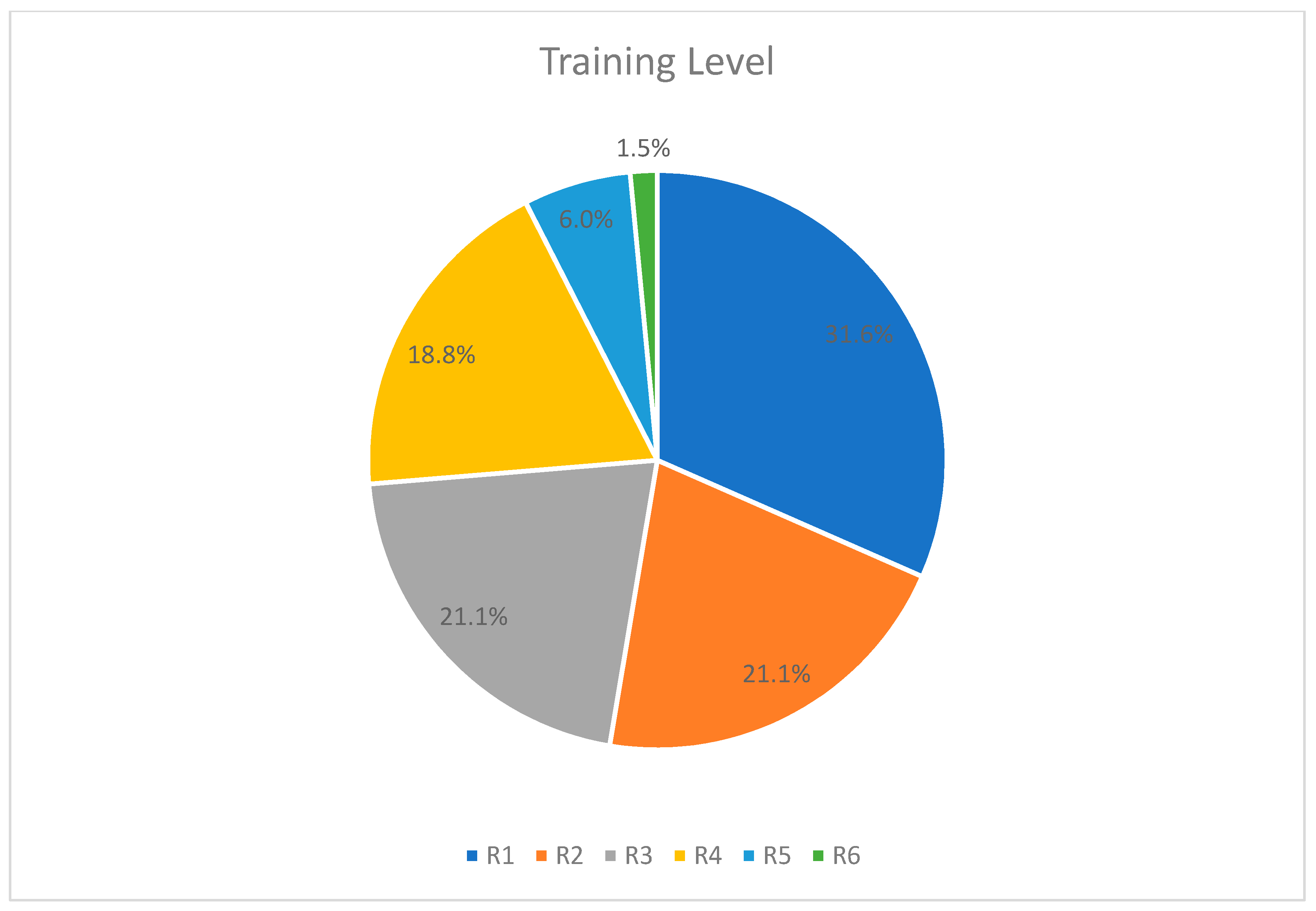
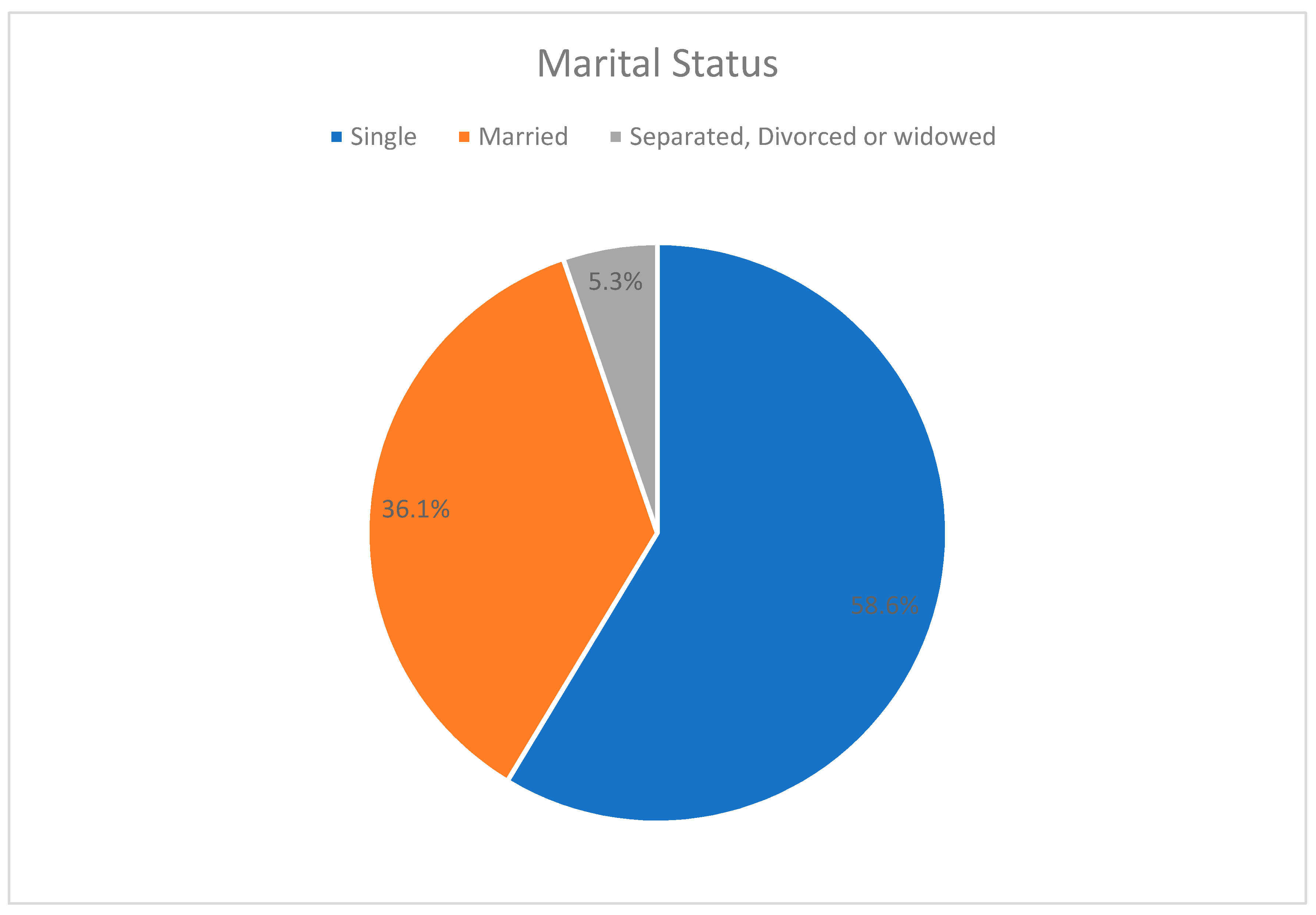
3.1. Demographics
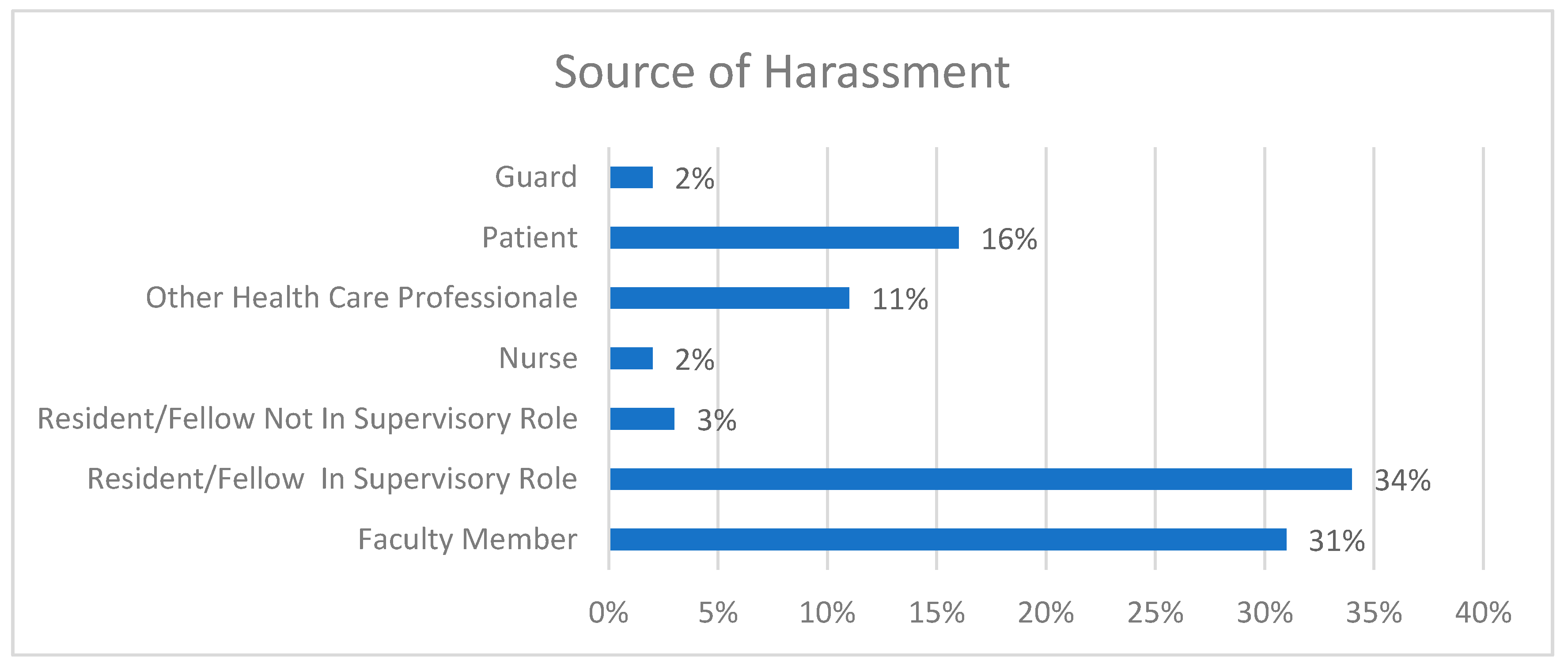
3.2. Facts on Harassment and Discrimination
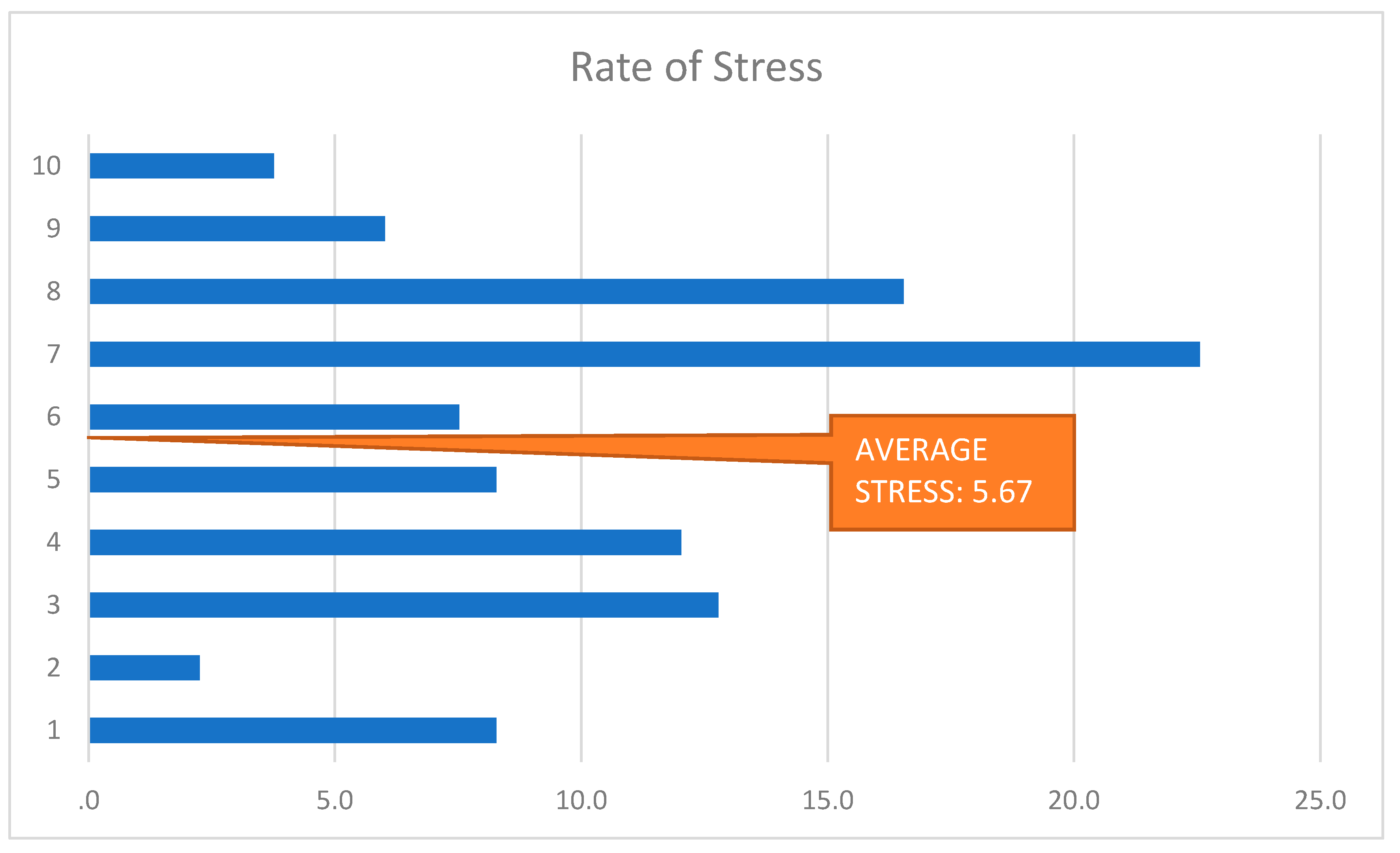
3.3. Mental Impact on Trainees
3.4. Overall Effect
4. Discussion
4.1. Key Findings: Discrimination Nature and Impacts
4.2. Interpretation of Results
- ▪
- A meta-analysis of 25 studies from 1960 to 2003 revealed that suicidal thoughts were 2.3 times higher in female physicians in comparison with the average population and male physicians;
- ▪
- ▪
- A cross-sectional national survey of general surgery residents showed that suicidal thoughts were reported by 4.5% of residents and were reported more frequently by women than by men (5.3% vs. 3.9%) [4].
4.3. Strengths and Limitations
4.4. Strategic Recommendations
4.5. Implications—Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- McMurray, J.E.; Linzer, M.; Konrad, T.R.; Douglas, J.; Shugerman, R.; Nelson, K. SGIM Career Satisfaction Study Group: The work lives of women physicians. J. Gen. Intern. Med. 2000, 1, 372–380. [Google Scholar]
- Nomura, K.; Yamazaki, Y.; Gruppen, L.D.; Horie, S.; Takeuchi, M.; Illing, J. The difficulty of professional continuation among female doctors in Japan: A qualitative study of alumnae of 13 medical schools in Japan. BMJ Open 2015, 5, 3. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.J.; Tanious, A.; Go, C.; Coleman, D.M.; McKinley, S.K.; Eagleton, M.J.; Clouse, W.D.; Conrad, M.F. Gender-based discrimination is prevalent in the integrated vascular trainee experience and serves as a predictor of burnout. J. Vasc. Surg. 2020, 71, 220–227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, Y.Y.; Ellis, R.J.; Hewitt, D.B.; Yang, A.D.; Cheung, E.O.; Moskowitz, J.T.; Potts, J.R., III; Buyske, J.; Hoyt, D.B.; Nasca, T.J.; et al. Discrimination, abuse, harassment, and burnout in surgical residency training. N. Engl. J. Med. 2019, 381, 1741–1752. [Google Scholar] [CrossRef] [PubMed]
- Holliday, E.B.; Siker, M.; Chapman, C.H.; Jagsi, R.; Bitterman, D.S.; Ahmed, A.A.; Winkfield, K.; Kelly, M.; Tarbell, N.J.; Deville, C., Jr. Achieving gender equity in the radiation oncology physician workforce. Adv. Radiat. Oncol. 2018, 3, 478–483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berlingo, L.; Girault, A.; Azria, E.; Goffinet, F.; Le Ray, C. Women and academic careers in obstetrics and gynaecology: Aspirations and obstacles among postgraduate trainees–a mixed-methods study. BJOG Int. J. Obstet. Gynaecol. 2019, 126, 770–777. [Google Scholar] [CrossRef]
- Dar-Odeh, N.; Elsayed, S.A.; Nourwali, I.; Ryalat, S.; Al-Shayyab, M.H.; Abu-Hammad, O. Social factors as career obstacles for female oral and maxillofacial surgeons in three Middle Eastern countries. Int. J. Oral Maxillofac. Surg. 2019, 48, 1504–1508. [Google Scholar] [CrossRef]
- Morrison, W.; Fowler, J. Responding to Bias, Bullying, and Harassment. In Manners, Morals, and Medical Care; Springer: Berlin/Heidelberg, Germany, 2020; pp. 95–124. [Google Scholar]
- Venkatesh, B.; Mehta, S.; Angus, D.C.; Finfer, S.; Machado, F.R.; Marshall, J.; Mitchell, I.; Peake, S.; Zimmerman, J.L. Women in Intensive Care study: A preliminary assessment of international data on female representation in the ICU physician workforce, leadership and academic positions. Crit. Care 2018, 22, 211. [Google Scholar] [CrossRef]
- Butkus, R.; Serchen, J.; Moyer, D.V.; Bornstein, S.S.; Hingle, S.T. Achieving gender equity in physician compensation and career advancement: A position paper of the American College of Physicians. Ann. Intern. Med. 2018, 168, 721–723. [Google Scholar] [CrossRef] [Green Version]
- Dayal, A.; O’Connor, D.M.; Qadri, U.; Arora, V.M. Comparison of male vs female resident milestone evaluations by faculty during emergency medicine residency training. JAMA Intern. Med. 2017, 177, 651–657. [Google Scholar] [CrossRef]
- Van Heest, A.E.; Fishman, F.; Agel, J. A 5-year update on the uneven distribution of women in orthopaedic surgery residency training programs in the United States. JBJS 2016, 98, e64. [Google Scholar] [CrossRef]
- Gerull, K.M.; Loe, M.; Seiler, K.; McAllister, J.; Salles, A. Assessing gender bias in qualitative evaluations of surgical residents. Am. J. Surg. 2019, 217, 306–313. [Google Scholar] [CrossRef] [PubMed]
- Hawker, F.H. Female specialists in intensive care medicine: Job satisfaction, challenges and work-life balance. Crit. Care Resusc. 2016, 18, 125. [Google Scholar] [PubMed]
- Turrentine, F.E.; Dreisbach, C.N.; St Ivany, A.R.; Hanks, J.B.; Schroen, A.T. Influence of gender on surgical residency applicants’ recommendation letters. J. Am. Coll. Surg. 2019, 228, 356–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jagsi, R.; Griffith, K.A.; Jones, R.; Perumalswami, C.R.; Ubel, P.; Stewart, A. Sexual harassment and discrimination experiences of academic medical faculty. JAMA 2016, 315, 2120–2121. [Google Scholar] [CrossRef]
- Rodney, A.C.; Olga, S.; Wayne, W. Family Medicine Graduates’ Perceptions of Intimidation, Harassment, and Discrimination during Residency Training. Available online: https://Bmcmededuc.biomedcentral.com/Articles/10.1186/1472-6920-11-88 (accessed on 22 October 2011).
- Fnais, N.; al-Nasser, M.; Zamakhshary, M.; Abuznadah, W.; Al-Dhukair, S.; Saadeh, M.; Al-Qarni, A.; Bokhari, B.; Alshaeri, T.; Aboalsamh, N.; et al. Prevalence of harassment and discrimination among residents in three training hospitals in Saudi Arabia. Ann. Saudi Med. 2013, 33, 134–139. [Google Scholar] [CrossRef] [Green Version]
- Bruce, A.N.; Battista, A.; Plankey, M.W.; Johnson, L.B.; Marshall, M.B. Perceptions of gender-based discrimination during surgical training and practice. Med. Educ. Online 2015, 20, 25923. [Google Scholar] [CrossRef]
- Jordan, S.; Scott, P. Well-Being in Residency Training: A Survey Examining Resident Physician Satisfaction Both within and Outside of Residency Training and Mental Health in Alberta. Available online: https://Bmcmededuc.biomedcentral.com/Articles/10.1186/1472-6920-5-21 (accessed on 22 October 2005).
- Alshammari, A.N.; Shafiq, M.O.; Altayeb, M.A.; Khaja, A.F.; Ghabban, K.M.; Khoshhal, K.I. Gulf cooperation Council female residents in orthopedics: Influences, barriers, and mental pressures: A cross-sectional study. J. Musculoskelet. Surg. Res. 2018, 2, 51. [Google Scholar] [CrossRef]
- Camargo, A.; Liu, L.; Yousem, D.M. Sexual harassment in radiology. J. Am. Coll. Radiol. 2017, 14, 1094–1099. [Google Scholar] [CrossRef]
- Broad, J.; Matheson, M.; Verrall, F.; Taylor, A.K.; Zahra, D.; Alldridge, L.; Feder, G. Discrimination, harassment and non-reporting in UK medical education. Med. Educ. 2018, 52, 414–426. [Google Scholar] [CrossRef]
- Mathews, B.; Bismark, M.M. Sexual harassment in the medical profession: Legal and ethical responsibilities. Med. J. Aust. 2015, 203, 189–192. [Google Scholar] [CrossRef] [Green Version]
- Stone, L.; Phillips, C.; Douglas, K.A. Sexual assault and harassment of doctors, by doctors: A qualitative study. Med. Educ. 2019, 53, 833–843. [Google Scholar] [CrossRef] [PubMed]
- Chun, S.E.; Lee, J.H.; Lee, J.E.; Lee, S.M.K.; Leem, J.; Kim, H. Impact of gender on the career development of female traditional Korean medicine doctors: A qualitative study. BMJ Open 2019, 9, e030390. [Google Scholar] [CrossRef] [PubMed]
- Hessel, K.; Di Pasco, P.; Kilgore, L.; Shelley, C.; Perry, A.; Wagner, J. Have we come as far as we had hoped? Discrimination in the residency interview. J. Surg. Educ. 2017, 74, 939–945. [Google Scholar] [CrossRef] [PubMed]
- Aljerian, K.; Almadani, A.; Alharbi, S.S. Study on the existence and extent of harassment among medical staff in a Saudi University Hospital. JSS Acad. High. Educ. Res. 2017, 5, 45–55. [Google Scholar] [CrossRef] [Green Version]
- Al-Maddah, E.M.; Al-Dabal, B.K.; Khalil, M.S. Prevalence of sleep deprivation and relation with depressive symptoms among medical residents in King Fahd University Hospital, Saudi Arabia. Sultan Qaboos Univ. Med. J. 2015, 15, e78. [Google Scholar] [PubMed]
- Demir, F.; Ay, P.; Erbas, M.; Ozdii, M.; Yasar, E. The prevalence of depression and its associated factors among resident doctors working in a training hospital in Istanbul. Turk Psikiyatri Dergisi 2007, 18, 31. [Google Scholar]
- Sadiq, M.S.; Morshed, N.M.; Rahman, W.; Chowdhury, N.F.; Arafat, S.Y.; Mullick, M.S. Depression, Anxiety, Stress among Postgraduate Medical Residents: A Cross sectional Observation in Bangladesh. Iran. J. Psychiatry Behav. Sci. 2019, 14, 192. [Google Scholar]
- Levy, A.B.; Nahhas, R.W.; Sampang, S.; Jacobs, K.; Weston, C.; Cerny-Suelzer, C.; Riese, A.; Munetz, M.R.; Shaw, J. Characteristics associated with depression and suicidal thoughts among medical residents: Results from the DEPRESS-Ohio Study. Acad. Psychiatry 2019, 43, 480–487. [Google Scholar] [CrossRef]
- Thommasen, H.V.; Lavanchy, M.; Connelly, I.; Berkowitz, J.; Grzybowski, S. Mental health, job satisfaction, and intention to relocate. Opinions of physicians in rural British Columbia. Can. Fam. Physician 2001, 47, 737–744. [Google Scholar]
- Goebert, D.; Thompson, D.; Takeshita, J.; Beach, C.; Bryson, P.; Ephgrave, K.; Kent, A.; Kunkel, M.; Schechter, J.; Tate, J. Depressive symptoms in medical students and residents: A multischool study. Acad. Med. 2009, 84, 236–241. [Google Scholar] [CrossRef] [PubMed]
- Jennings, M.L.; Slavin, S.J. Resident wellness matters: Optimizing resident education and wellness through the learning environment. Acad. Med. 2015, 90, 1246–1250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sicilia, M.A.; Lytras, M. On the representation of change according to different ontologies of learning. Int. J. Learn. Chang. 2005, 1, 66–79. [Google Scholar] [CrossRef] [Green Version]
- Vargas-Vera, M.; Lytras, M. Exploiting semantic web and ontologies for personalised learning services: Towards semantic web-enabled learning portals for real learning experiences. Int. J. Knowl. Learn. 2008, 4, 1–17. [Google Scholar] [CrossRef]
- Housawi, A.; Al Amoudi, A.; Alsaywid, B.; Lytras, M.; bin Moreba, Y.H.; Abuznadah, W.; Alhaidar, S.A. Evaluation of Key Performance Indicators (KPIs) for Sustainable Postgraduate Medical Training: An Opportunity for Implementing an Innovative Approach to Advance the Quality of Training Programs at the Saudi Commission for Health Specialties (SCFHS). Sustainability 2020, 12, 8030. [Google Scholar] [CrossRef]
- Housawi, A.; Al Amoudi, A.; Alsaywid, B.; Lytras, M.; bin Moreba, Y.H.; Abuznadah, W.; Munshi, F.; Al Haider, S.; Tolah, A.W. A Progressive Model for Quality Benchmarks of Trainees’ Satisfaction in Medical Education: Towards Strategic Enhancement of Residency Training Programs at Saudi Commission for Health Specialties (SCFHS). Sustainability 2020, 12, 10186. [Google Scholar] [CrossRef]
- Drigas, A.; Ioannidou, R.E.; Kokkalia, G.; Lytras, M.D. ICTs, mobile learning and social media to enhance learning for attention difficulties. J. UCS 2014, 20, 1499–1510. [Google Scholar]
- Vossen, G.; Lytras, M.; Koudas, N. Revisiting the (machine) Semantic Web: The missing layers for the human Semantic Web. IEEE Trans. Knowl. Data Eng. 2007, 19, 145. [Google Scholar] [CrossRef]


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Literature Review | |||
|---|---|---|---|
| Author(s) | Title of Article | Key Contribution | Relevance for Our Study |
| Nomura Kyoko; Yamazaki Yuka; Gruppen Larry D; Horie Saki; Takeuchi Masumi; Illing Jan; (2015) [2] | The difficulty of professional continuation among female doctors in Japan: a qualitative study of alumnae of 13 medical schools in Japan. | This study detected higher pressure on female physicians due to their hectic job schedule, taking into account their family responsibilities; they also introduced specific measures towards division of labour in relation to sex. | Work distribution in healthcare units should be redetermined according to the female physicians’ requirements |
| Wang Linda J; Tanious Adam; Go Catherine; Coleman Dawn M; McKinley Sophia K; Eagleton Matthew J; Clouse W Darrin; Conrad Mark F; (2020) [3] | Gender-based discrimination is prevalent in the integrated vascular trainee experience and serves as a predictor of burnout. | Female vascular residents are more likely to experience gender-related discrimination practices than their male colleagues, a fact that corresponds to higher burnout rates and obstructed recruitment. | We want to examine whether these findings can be observed in trainees of other specialties as well. |
| Hu Yue-Yung; Ellis Ryan J; Hewitt D Brock; Yang Anthony D; Cheung Elaine Ooi; Moskowitz Judith T; Potts III John R; Buyske Jo; Hoyt David B; Nasca Thomas J; (2019) [4] | Discrimination, abuse, harassment, and burnout in surgical residency training. | Burnout symptoms as well as suicidal thoughts of female residents in various surgical programs derive from racial discrimination and sexism in the healthcare workplace. | We want to further investigate female residents’ mental health, and possible causal effects of sexism in medicine. |
| Holliday Emma B; Siker Malika; Chapman Christina H; Jagsi Reshma; Bitterman Danielle S; Ahmed Awad A; Winkfield Karen; Kelly Maria; Tarbell Nancy J; Deville Jr Curtiland; (2018) [5] | Achieving gender equity in the radiation oncology physician workforce | Investigated gender inequity’s development in the medical workplace, potent correlation to career impediment and proposed dealing measures. | We are interested in clarifying the relation between sex discrimination and career impediment, as well as proposing more specific courses of action against it. |
| Berlingo L; Girault A; Azria E; Goffinet F; Le Ray C; (2019) [6] | Women and academic careers in obstetrics and gynaecology: aspirations and obstacles among postgraduate trainees—a mixed-methods study | Using mixed methods, this French study pinpointed that 3 times more female residents felt uncertain about their career in obstetrics and gynaecology, than their male colleagues. | Is this uncertainty observed in female trainees of other specialties in Jeddah? |
| Dar-Odeh N; Elsayed SA; Nourwali I; Ryalat S; Al-Shayyab MH; Abu-Hammad O; (2019) [7] | Social factors as career obstacles for female oral and maxillofacial surgeons in three Middle Eastern countries, | Most female oral and maxillofacial surgeons in Egypt, Jordan, and Saudi Arabia deemed sex discrimination, along with their social and personal profile, to be an obstacle in their academic career. | We are interested in examining how sexism affects not only specialized female physicians but also trainees, and how women in medicine can combine social and professional parameters. |
| Morrison Wynne; Fowler Jessica (2020) [8] | Responding to Bias, Bullying, and Harassment. | Female students and physicians are inhibited in terms of mentorship and academic advancement. | There is an evident pathologic hierarchy in medicine that we should address. |
| Venkatesh Bala; Mehta Sangeeta; Angus Derek C; Finfer Simon; Machado Flavia R; Marshall John; Mitchell Imogen; Peake Sandra; Zimmerman Janice L (2018) [9] | Women in Intensive Care study: a preliminary assessment of international data on female representation in the ICU physician workforce, leadership and academic positions. | According to this research, generally speaking women, both trainnes and specialists in the IC workforce, face gender discrimination and cannot advance their studies and position accordingly. | We want to focus on trainning females in all departments and identify how and from whom they receive discriminatory attitudes. |
| Butkus Renee; Serchen Joshua; Moyer Darilyn V; Bornstein Sue S; Hingle Susan Thompson; (2018) [10] | Achieving gender equity in physician compensation and career advancement: a position paper of the American College of Physicians, Annals of internal medicine. | Women in medicine are absent from leadership roles, are deprived of academic guidance and suffer from imposter syndrome—all in all they are operationally isolated in thei workplace. | Sexual harassment in healthcare working environment could be responsible for women’s exclusion from academic achievements |
| Camargo Aline; Liu Li; Yousem David M (2017) [22] | Sexual harassment in radiology, | Training women radiologists experiencing sexual harassment find difficuty in communicating their situation to the authorities (especially in US). | Why do trainees restrain from reporting discrimination incidents, and how is this explained? |
| Stone Louise; Phillips Christine; Douglas Kirsty A (2019) [25] | Sexual assault and harassment of doctors, by doctors: a qualitative study. | The female participants of this research considered complaining about their being discriminated as unprofessional or even harmful to their personal and academic wellbeing. | Which factors led the female doctors to being indifferent to improving their own working conditions? |
| Chun Se Eun; Lee Ju Hyun; Lee Ju Eun; Lee Seung Min Kathy; Leem Jungtae; Kim Hyunho; (2019) [26] | Impact of gender on the career development of female traditional Korean medicine doctors: a qualitative study. | This study indicated there is a stereotypical correlation of Korean female physicians with limited medical specialties (i.e., pediatrics), both from their colleagues and their patients. | We shall look into gender discrimimation in general as an obstacle in choosing residency specialty. |
| Bruce Adrienne N; Battista Alexis; Plankey Michael W; Johnson Lynt B; Marshall M Blair; (2015) [20] | Perceptions of gender-based discrimination during surgical training and practice. | Most questionees had experienced sex-related discrimination at an under-graduate or post-graduate level, and even more in their clinical practice; both women and especially men colleagues constituted a source of harassment. | We shall investigate the source of harassment against female trainees in Jeddah. |
| Key Aspects | Key Findings | Brief Interpretation |
|---|---|---|
| Discrimination Nature |
| Systematic gender discrimination practices are rooted in pathologic hierarchy of the healthcare system. |
| ||
| ||
| Mental Impacts |
| Excessive emotional stress incites female residents to have second thoughts about their career or even their life. |
| ||
| Overall Harm |
| The discrimination in question sets a vicious challenge: residents do not succeed academically nor do they find institutional support. |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yaghmour, A.; Alesa, A.; Anbarserry, E.; Abdullah Binmerdah, M.; Alharbi, A.; Housawi, A.; Almehdar, M.; Lytra, H.; Alsaywid, B.; Lytras, D.M. Challenges and Obstacles Faced by Trainee Female Physicians: An Integrative Research on Gender Discrimination, Stress, Depression and Harassment. Healthcare 2021, 9, 160. https://doi.org/10.3390/healthcare9020160
Yaghmour A, Alesa A, Anbarserry E, Abdullah Binmerdah M, Alharbi A, Housawi A, Almehdar M, Lytra H, Alsaywid B, Lytras DM. Challenges and Obstacles Faced by Trainee Female Physicians: An Integrative Research on Gender Discrimination, Stress, Depression and Harassment. Healthcare. 2021; 9(2):160. https://doi.org/10.3390/healthcare9020160
Chicago/Turabian StyleYaghmour, Aisha, Alaa Alesa, Esraa Anbarserry, Merihan Abdullah Binmerdah, Ahlam Alharbi, Abdulrahman Housawi, Manal Almehdar, Hara Lytra, Basim Alsaywid, and Dimitrios M. Lytras. 2021. "Challenges and Obstacles Faced by Trainee Female Physicians: An Integrative Research on Gender Discrimination, Stress, Depression and Harassment" Healthcare 9, no. 2: 160. https://doi.org/10.3390/healthcare9020160