
Sources of Resilience in Frontline Health Professionals during COVID-19

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design, Setting, and Participants
2.2. Procedure
2.3. Data Collection
2.4. Data Management and Analysis
3. Results
3.1. Participant Characteristics
3.2. Qualitative Results
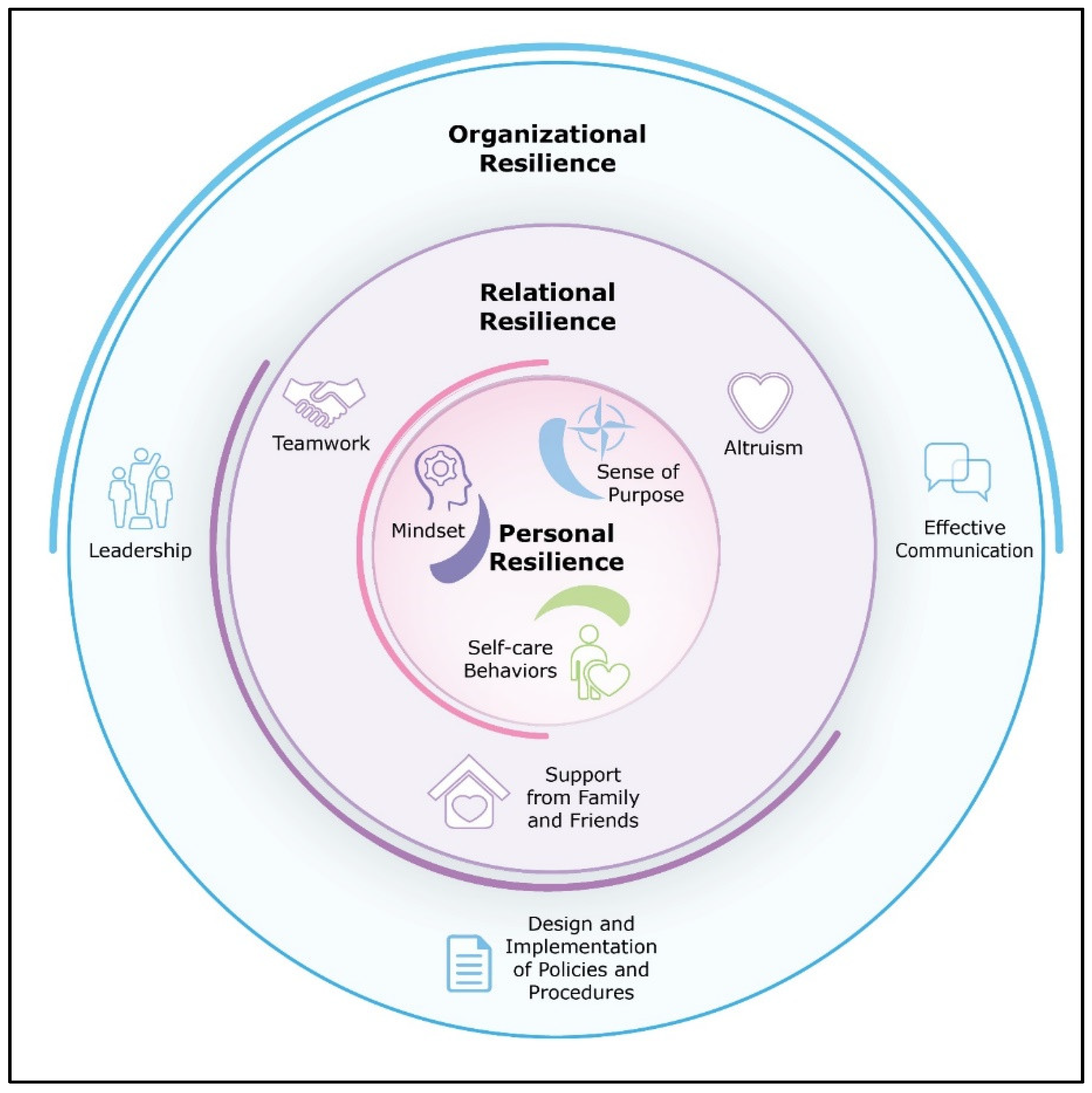
3.2.1. Theme 1: Personal Resilience
Mindset
Finding a Sense of Purpose
Self-Care Behaviours
3.2.2. Theme 2: Relational Resilience
Teamwork
Altruism
Social Support Outside of Work
3.2.3. Theme 3: Organisational Resilience
Design and Implementation of Policies and Procedures
Leadership
Effective Communication
3.2.4. Trust
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bonanno, G.A. Loss, trauma, and humn resilience: Have we underestimated the human capacity to thrive after extremely aversive events? Am. Psychol. 2004, 59, 20–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holmes, E.A.; O’Connor, R.C.; Perry, V.H.; Tracey, I.; Wessely, S.; Arseneault, L.; Ballard, C.; Christensen, H.; Silver, R.C.; Everall, I.; et al. Multidisciplinary research priorities for the COVID-19 pandemic: A call for action for mental health science. Lancet Psychiatry 2020, 7, 547–560. [Google Scholar] [CrossRef]
- West, C.P.; Dyrbye, L.N.; Sinsky, C.; Trockel, M.; Tutty, M.; Nedelec, L.; Carlasare, E.; Shanafelt, T. Resilience and burnout among physicians and the general US working population. JAMA Netw. Open 2020, 3, e209385. [Google Scholar] [CrossRef] [PubMed]
- Holton, S.; Wynter, K.; Trueman, M.; Bruce, S.; Sweeney, S.; Crowe, S.; Dabscheck, A.; Eleftheriou, P.; Booth, S.; Hitch, D.; et al. Psychological well-being of Australian hospital clinical staff during the COVID-19 pandemic. Aust. Health Rev. 2021, 45, 297–305. [Google Scholar] [CrossRef] [PubMed]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Netw. Open 2020, 3, e203976. [Google Scholar] [CrossRef]
- Sumner, R.C.; Kinsella, E.L. Grace Under Pressure: Resilience, Burnout, and Wellbeing in Frontline Workers in the United Kingdom and Republic of Ireland During the SARS-CoV-2 Pandemic. Front. Psychol. 2021, 11, 576229. [Google Scholar] [CrossRef] [PubMed]
- Rieckert, A.; Schuit, E.; Bleijenberg, N.; Cate, D.T.; de Lange, W.; Ginkel, J.M.D.M.-V.; Mathijssen, E.; Smit, L.C.; Stalpers, D.; Schoonhoven, L.; et al. How can we build and maintain the resilience of our health care professionals during COVID-19? Recommendations based on a scoping review. BMJ Open 2021, 11, e043718. [Google Scholar] [CrossRef] [PubMed]
- Roberts, N.J.; McAloney-Kocaman, K.; Lippiett, K.; Ray, E.; Welch, L.; Kelly, C. Levels of resilience, anxiety and depression in nurses working in respiratory clinical areas during the COVID pandemic. Respir. Med. 2021, 176, 106219. [Google Scholar] [CrossRef]
- Banerjee, D.; Rao, T.S.S.; Kallivayalil, R.A.; Javed, A. Psychosocial framework of resilience: Navigating needs and adversities during the pandemic, a qualitative exploration in the Indian frontline physicians. Front. Psychol. 2021, 12, 622132. [Google Scholar] [CrossRef]
- Munawar, K.; Choudhry, F.R. Exploring stress coping strategies of frontline emergency health workers dealing COVID-19 in Pakistan: A qualitative inquiry. Am. J. Infect. Control. 2021, 49, 286–292. [Google Scholar] [CrossRef]
- Ding, S.; Deng, S.; Zhang, Y.; Wang, Q.; Yang, X. Experiences of Front-Line Medical Staffs Fighting Against Coronavirus Disease 2019: A Meta-Synthesis of Qualitative Studies. Available online: https://bmchealthservres.biomedcentral.com/articles/10.1186/s12913-021-06917-z (accessed on 6 September 2021).
- Sun, N.; Wei, L.; Shi, S.; Jiao, D.; Song, R.; Ma, L.; Wang, H.; Wang, C.; Wang, Z.; You, Y. A qualitative study on the psychological experience of caregivers of COVID-19 patients. Am. J. Infect. Control. 2020, 48, 592–598. [Google Scholar] [CrossRef] [PubMed]
- Shanafelt, T.; Ripp, J.; Trockel, M. Understanding and addressing sources of anxiety among health care professionals during the COVID-19 pandemic. JAMA 2020, 323, 2133–2134. [Google Scholar] [CrossRef]
- Liu, Q.; Luo, D.; Haase, J.E.; Guo, Q.; Wang, X.Q.; Liu, S.; Xia, L.; Liu, Z.; Yang, J.; Yang, B.X. The experiences of health-care providers during the COVID-19 crisis in China: A qualitative study. Lancet Glob. Health 2020, 8, e790–e798. [Google Scholar] [CrossRef]
- Vindrola-Padros, C.; Andrews, L.; Dowrick, A.; Djellouli, N.; Fillmore, H.; Gonzales, E.B.; Javadi, D.; Lewis-Jackson, S.; Manby, L.; Mitchinson, L.; et al. Perceptions and experiences of healthcare workers during the COVID-19 pandemic in the UK. BMJ Open 2020, 10, e040503. [Google Scholar] [CrossRef]
- Dzau, V.J.; Kirch, D.; Nasca, T. Preventing a parallel pandemic—A national strategy to protect clinicians’ well-being. N. Engl. J. Med. 2020, 383, 513–515. [Google Scholar] [CrossRef] [PubMed]
- Blake, H.; Bermingham, F.; Johnson, G.; Tabner, A. Mitigating the psychological impact of COVID-19 on healthcare workers: A digital learning package. Int. J. Environ. Res. Public Health 2020, 17, 2997. [Google Scholar] [CrossRef]
- Albott, C.S.; Wozniak, J.R.; McGlinch, B.P.; Wall, M.H.; Gold, B.S.; Vinogradov, S. Battle buddies: Rapid deployment of a psychological resilience intervention for health care workers during the coronavirus disease 2019 pandemic. Anesth. Analg. 2020, 131, 43–54. [Google Scholar] [CrossRef]
- Sheldon, K.M.; King, L. Why positive psychology is necessary. Am. Psychol. 2001, 56, 216. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Castleberry, A.; Nolen, A. Thematic analysis of qualitative research data: Is it as easy as it sounds? Curr. Pharm. Teach. Learn. 2018, 10, 807–815. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 386–396. [Google Scholar] [CrossRef]
- Campbell-Sills, L.; Stein, M.B. Psychometric analysis and refinement of the connor–davidson resilience scale (CD-RISC): Validation of a 10-item measure of resilience. J. Trauma. Stress 2007, 20, 1019–1028. [Google Scholar] [CrossRef] [PubMed]
- Vaismoradi, M.; Turunen, H.; Bondas, T. Content analysis and thematic analysis: Implications for conducting a qualitative descriptive study. Nurs. Health Sci. 2013, 15, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Miyata, H.; Kai, I. Reconsidering evaluation criteria for scientific adequacy in health care research: An integrative framework of quantitative and qualitative criteria. Int. J. Qual. Methods 2009, 8, 64–75. [Google Scholar] [CrossRef]
- Santiago-Delefosse, M.; Gavin, A.; Bruchez, C.; Roux, P.; Stephen, S.L. Quality of qualitative research in the health sciences: Analysis of the common criteria present in 58 assessment guidelines by expert users. Soc. Sci. Med. 2016, 148, 142–151. [Google Scholar] [CrossRef] [PubMed]
- Antonijevic, J.; Binic, I.; Zikic, O.; Manojlovic, S.; Tosic-Golubovic, S.; Popovic, N. Mental health of medical personnel during the COVID-19 pandemic. Brain Behav. 2020, 10, e01881. [Google Scholar] [CrossRef]
- Purvis, T.E.; Saylor, D. Burnout and resilience among neurosciences critical care unit staff. Neurocrit. Care 2019, 31, 406–410. [Google Scholar] [CrossRef]
- Robertson, H.D.; Elliott, A.M.; Burton, C.; Iverson, L.; Murchie, P.; Porteous, T.; Matheson, C. Resilience of primary healthcare professionals: A systematic review. Br. J. Gen. Pract. 2016, 66, e423–e433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santarone, K.; McKenney, M.; Elkbuli, A. Preserving mental health and resilience in frontline healthcare workers during COVID-19. Am. J. Emerg. Med. 2020, 38, 1530–1531. [Google Scholar] [CrossRef]
- Greenberg, N.; Tracy, D. What healthcare leaders need to do to protect the psychological well-being of frontline staff in the COVID-19 pandemic. BMJ Leader 2020, 4, 101–102. [Google Scholar] [CrossRef]
- Labrague, L.J.; De los Santos, J.A.A. COVID-19 anxiety among front-line nurses: Predictive role of organisational support, personal resilience and social support. J. Nurs. Manag. 2020, 28, 1653–1661. [Google Scholar] [CrossRef] [PubMed]
- Lyu, Y.; Yu, Y.; Chen, S.; Lu, S.; Ni, S. Positive functioning at work during COVID-19: Posttraumatic growth, resilience, and emotional exhaustion in Chinese frontline healthcare workers. Appl. Psychol. Health Well-Being 2021, 13, 871–886. [Google Scholar] [CrossRef]
- Zhang, X.; Jiang, X.; Ni, P.; Li, H.; Li, C.; Zhou, Q.; Ou, Z.; Guo, Y.; Co, J. Association between resilience and burnout of front-line nurses at the peak of the COVID-19 pandemic: Positive and negative affect as mediators in Wuhan. Int. J. Ment. Health Nurs. 2021, 30, 939–954. [Google Scholar] [CrossRef]
- Heath, C.; Sommerfield, A.; von Ungern-Sternberg, B. Resilience strategies to manage psychological distress among healthcare workers during the COVID-19 pandemic: A narrative review. Anaesthesia 2020, 75, 1364–1371. [Google Scholar] [CrossRef] [PubMed]
- Moreno, C.; Wykes, T.; Galderisi, S.; Nordentoft, M.; Crossley, N.; Jones, N. How mental health care should change as a consequence of the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 813–824. [Google Scholar] [CrossRef]
- Magnavita, N.; Soave, P.M.; Antonelli, M. A One-Year Prospective Study of Work-Related Mental Health in the Intensivists of a COVID-19 Hub Hospital. Int. J. Environ. Res. Public Health 2021, 18, 9888. [Google Scholar] [CrossRef] [PubMed]
- Magnavita, N.; Soave, P.M.; Antonelli, M. Prolonged Stress Causes Depression in Frontline Workers Facing the COVID-19 Pandemic. A Repeated Cross-Sectional Study. Available online: https://www.preprints.org/manuscript/202105.0129/v1 (accessed on 7 May 2021).
- Sanchez-Gomez, M.; Sadovyy, M.; Breso, E. Health-Care Professionals Amid the COVID-19 Pandemic: How Emotional Intelligence May Enhance Work Performance Traversing the Mediating Role of Work Engagement. J. Clin. Med. 2021, 10, 4077. [Google Scholar] [CrossRef]


{kind=link}
| Variable | N (%) |
|---|---|
| Gender | |
| Female | 16 (80%) |
| Age range | |
| 30–39 | 9 (45%) |
| 40–49 | 8 (40%) |
| 50–59 | 3 (15%) |
| Profession | |
| Nurse | 8 (40%) |
| Allied health | 7 (35%) |
| Doctor | 5 (25%) |
| Hospital setting * | |
| Acute care | 80% |
| Rehabilitation | 20% |
| Aged care | 20% |
| Years in profession | |
| 0–5 | 2 (10%) |
| 6–10 | 1 (5%) |
| 10–15 | 7 (35%) |
| 16+ | 10 (50%) |
| Employment status | |
| Full-time | 14 (70%) |
| Part-time or casual | 6 (30%) |
| PSS | M = 12.7 (SD = 6.2) |
| Resilience | M = 32.1 (SD = 5.3) |
| Individual Level |
|---|
Help healthcare professionals to cultivate a positive mindset (targeted sources of resilience: positive mindset and teamwork)
|
Provide opportunities to reflect on the value and meaning of pandemic work (targeted sources of resilience: finding purpose, altruism, positive mindset, and teamwork)
|
Support healthy lifestyle choices (targeted sources of resilience: healthy lifestyle and teamwork)
|
| Relational Level |
Recognise frontline healthcare professional external social supports (targeted source of resilience: social support)
|
| Organisational Level |
Develop effective policies and procedures (targeted source of resilience: design and implementation of policies and procedures, leadership, and effective organisation-wide communication)
|
Enhance leadership (targeted source of resilience: leadership and effective communication)
|
Invest in hospital-wide communication platforms (targeted source of resilience: effective communication, implementation of policies and procedures, teamwork, and inspiring leadership)
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brown, L.; Haines, S.; Amonoo, H.L.; Jones, C.; Woods, J.; Huffman, J.C.; Morris, M.E. Sources of Resilience in Frontline Health Professionals during COVID-19. Healthcare 2021, 9, 1699. https://doi.org/10.3390/healthcare9121699
Brown L, Haines S, Amonoo HL, Jones C, Woods J, Huffman JC, Morris ME. Sources of Resilience in Frontline Health Professionals during COVID-19. Healthcare. 2021; 9(12):1699. https://doi.org/10.3390/healthcare9121699
Chicago/Turabian StyleBrown, Lydia, Simon Haines, Hermioni L. Amonoo, Cathy Jones, Jeffrey Woods, Jeff C. Huffman, and Meg E. Morris. 2021. "Sources of Resilience in Frontline Health Professionals during COVID-19" Healthcare 9, no. 12: 1699. https://doi.org/10.3390/healthcare9121699