
Impact of the COVID-19 Pandemic on Patients with Gastrointestinal Cancer Undergoing Active Cancer Treatment in an Ambulatory Therapy Center: The Patients’ Perspective

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, C.; Horby, P.W.; Hayden, F.G.; Gao, G.F. A novel coronavirus outbreak of global health concern. Lancet 2020, 395, 470–473. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization Coronavirus Disease (COVID-19) Pandemic. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 2 August 2021).
- Looi, M.K. COVID-19: Japan Ends State of Emergency but Warns of “New Normal”. BMJ 2020, 369, m2100. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labor and Welfare of Japan. Novel Coronavirus (COVID-19). Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000164708_00001.html (accessed on 2 August 2021).
- Centers for Disease Control and Prevention Coronavirus Disease 2019 (COVID-19). Available online: https://www.cdc.gov/coronavirus/2019-ncov/index.html (accessed on 2 August 2021).
- Vecchione, L.; Stintzing, S.; Pentheroudakis, G.; Douillard, J.-Y.; Lordick, F. ESMO management and treatment adapted recommendations in the COVID-19 era: Colorectal cancer. ESMO Open 2020, 5 (Suppl. 3), e000826. [Google Scholar] [CrossRef] [PubMed]
- European Society for Medical Oncology Cancer Patient Management during the COVID-19 Pandemic. Available online: https://www.esmo.org/guidelines (accessed on 2 August 2021).
- Lou, E.; Beg, S.; Bergsland, E.; Eng, C.; Khorana, A.; Kopetz, S.; Lubner, S.; Saltz, L.; Shankaran, V.; Zafar, S.Y. Modifying Practices in GI Oncology in the Face of COVID-19: Recommendations from Expert Oncologists on Minimizing Patient Risk. JCO Oncol. Pr. 2020, 16, 383–388. [Google Scholar] [CrossRef]
- Erdem, D.; Karaman, I. Awareness and perceptions related to COVID-19 among cancer patients: A survey in oncology department. Eur. J. Cancer Care 2020, 29, e13309. [Google Scholar] [CrossRef] [PubMed]
- Lou, E.; Teoh, D.; Brown, K.; Blaes, A.; Holtan, S.G.; Jewett, P.; Parsons, H.; Mburu, E.W.; Thomaier, L.; Hui, J.Y.C.; et al. Perspectives of cancer patients and their health during the COVID-19 pandemic. PLoS ONE 2020, 15, e0241741. [Google Scholar] [CrossRef] [PubMed]
- Qian, K.; Yahara, T. Mentality and behavior in COVID-19 emergency status in Japan: Influence of personality, morality and ideology. PLoS ONE 2020, 15, e0235883. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 2 August 2021).
- González-Sanguino, C.; Ausín, B.; Castellanos, M.Á.; Saiz, J.; López-Gómez, A.; Ugidos, C.; Muñoz, M. Mental health consequences during the initial stage of the 2020 Coronavirus pandemic (COVID-19) in Spain. Brain Behav. Immun. 2020, 87, 172–176. [Google Scholar] [CrossRef]
- Klaiber, P.; Wen, J.H.; DeLongis, A.; Sin, N.L. The Ups and Downs of Daily Life during COVID-19: Age Differences in Affect, Stress, and Positive Events. J. Gerontol. Ser. B 2021, 76, e30–e37. [Google Scholar] [CrossRef]
- Van Tilburg, T.G.; Steinmetz, S.; Stolte, E.; van der Roest, H.; de Vries, D.H. Loneliness and mental health during the COVID-19 pandemic: A study among Dutch older adults. J. Gerontol. B Psychol. Sci. Soc. Sci. 2020, 76, e249–e255. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.E.; Bangen, K.J.; Avanzino, J.A.; Hou, B.; Ramsey, M.; Eglit, G.; Liu, J.; Tu, X.M.; Paulus, M.; Jeste, D.V. Outcomes of Randomized Clinical Trials of Interventions to Enhance Social, Emotional, and Spiritual Components of Wisdom: A Systematic Review and Meta-analysis. JAMA Psychiatry 2020, 77, 925–935. [Google Scholar] [CrossRef]
- Czeisler, M.É.; Lane, R.I.; Petrosky, E.; Wiley, J.F.; Christensen, A.; Njai, R.; Weaver, M.D.; Robbins, R.; Facer-Childs, E.R.; Barger, L.K.; et al. Mental Health, Substance Use, and Suicidal Ideation During the COVID-19 Pandemic—United States, June 24–30, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1049–1057. [Google Scholar] [CrossRef]
- Gebhard, C.; Regitz-Zagrosek, V.; Neuhauser, H.K.; Morgan, R.; Klein, S.L. Impact of sex and gender on COVID-19 outcomes in Europe. Biol. Sex Differ. 2020, 11, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Haitao, T.; Vermunt, J.V.; Abeykoon, J.; Ghamrawi, R.; Gunaratne, M.; Jayachandran, M.; Narang, K.; Parashuram, S.; Suvakov, S.; Garovic, V.D. COVID-19 and Sex Differences: Mechanisms and Biomarkers. Mayo Clin. Proc. 2020, 95, 2189–2203. [Google Scholar] [CrossRef] [PubMed]
- Pivonello, R.; Auriemma, R.S.; Pivonello, C.; Isidori, A.M.; Corona, G.; Colao, A.; Millar, R.P. Sex disparities in COVID-19 severity and outcome: Are men weaker or women stronger? Neuroendocrinology 2020, 111, 1066–1085. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Demographics | Options | n | (%) |
|---|---|---|---|
| Sex | Male | 27 | 64 |
| Female | 15 | 36 | |
| Age (years) | <40 | 0 | 0 |
| 40–50 | 5 | 10 | |
| 50–60 | 10 | 21 | |
| 60–70 | 13 | 27 | |
| 70–80 | 14 | 29 | |
| ≧80 | 6 | 13 | |
| Type of cancer | Colorectal cancer | 21 | 48 |
| Gastric cancer | 15 | 34 | |
| Esophageal cancer | 6 | 14 | |
| Small intestinal cancer | 2 | 5 | |
| With whom they speak about their condition | Attending physician | 35 | 73 |
| (with overlap) | Family | 21 | 44 |
| Friends | 4 | 8 | |
| Nurse | 1 | 2 |
| Questions | Before the Pandemic | During the Pandemic | p-Value |
|---|---|---|---|
| Median (IQR) | Median (IQR) | ||
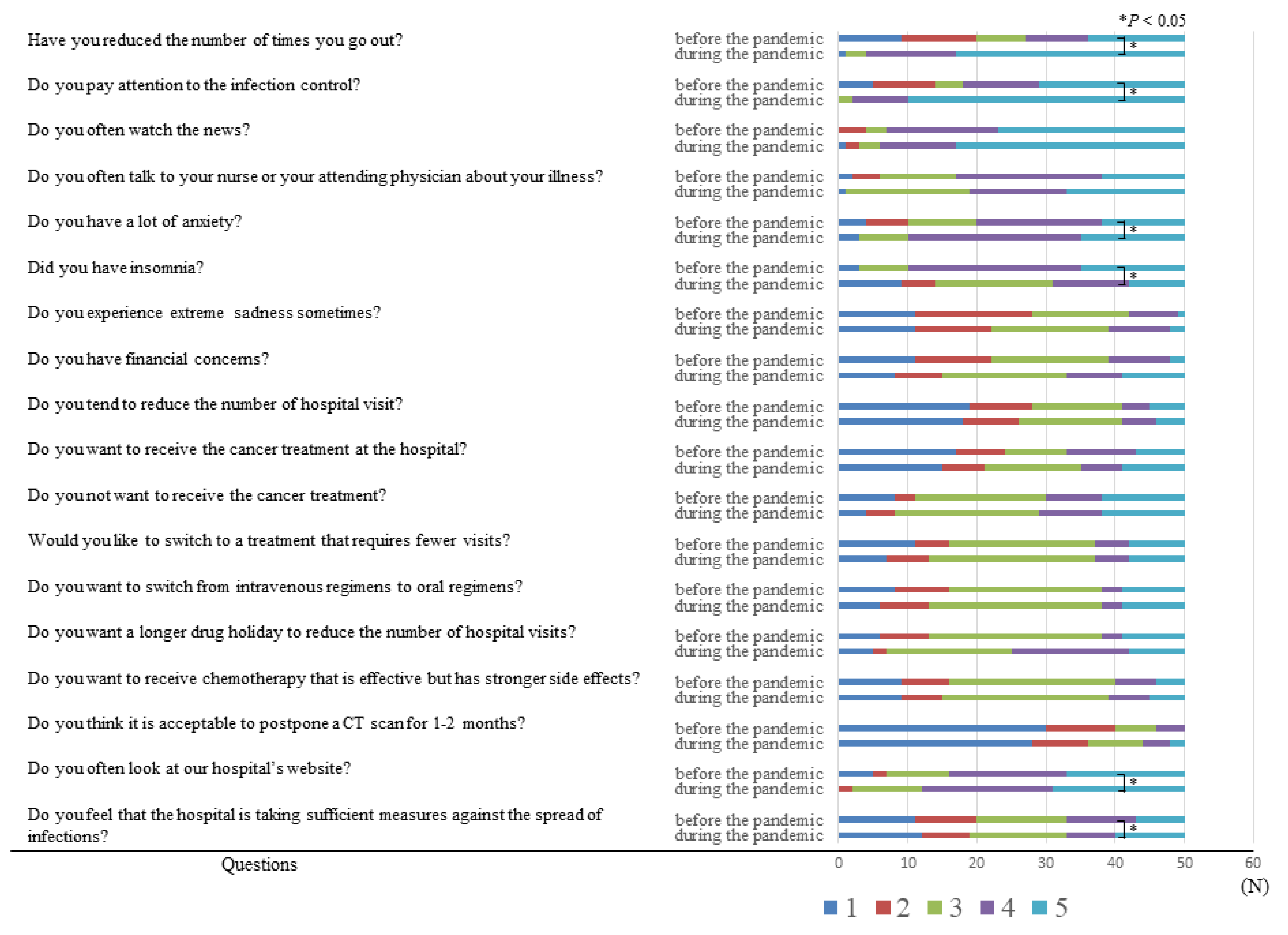
| Have you reduced the number of times you go out? | 3 (2–5) | 5 (4–5) | <0.001 |
| Do you pay attention to the infection control? | 4 (3–5) | 5 (5–5) | <0.001 |
| Do you often watch the news? | 5 (4–5) | 5 (4–5) | 0.444 |
| Do you often talk to your nurse or your attending physician about your illness? | 4 (3–4) | 4 (3–5) | 0.307 |
| Do you have a lot of anxiety? | 4 (3–4) | 4 (4–5) | 0.008 |
| Did you have insomnia? | 4 (3–4) | 4 (4–5) | 0.008 |
| Do you experience extreme sadness sometimes? | 2 (2–3) | 3 (2–3) | 0.08 |
| Do you have financial concerns? | 3 (2–4) | 3 (2–4) | 0.322 |
| Do you tend to reduce the number of hospital visit? | 3 (2–3.75) | 3 (2–4) | 0.057 |
| Do you want to receive the cancer treatment at the hospital? | 2 (1–3) | 2 (1–3) | 0.735 |
| Do you not want to receive the cancer treatment? | 3 (1–4) | 3 (1–4) | 0.44 |
| Would you like to switch to a treatment that requires fewer visits? | 3 (3–4) | 3 (3–4) | 0.371 |
| Do you want to switch from intravenous regimens to oral regimens? | 3 (2–3.75) | 3 (2.25–3.75) | 0.227 |
| Do you want a longer drug holiday to reduce the number of hospital visits? | 2 (2–3) | 2 (2–3) | 0.652 |
| Do you want to receive chemotherapy that is effective but has stronger side effects? | 4 (3–5) | 4 (4–5) | 0.214 |
| Do you think it is acceptable to postpone a CT scan for 1–2 months? | 3 (2–3) | 3 (2–3) | 0.444 |
| Do you often look at our hospital’s website? | 1 (1–2) | 1 (1–3) | 0.018 |
| Do you feel that the hospital is taking sufficient measures against the spread of infections? | 4 (3–5) | 4 (4–5) | 0.005 |
| <70 Years | ≥70 Years | |||||
|---|---|---|---|---|---|---|
| Before the Pandemic Median (IQR) | During the Pandemic Median (IQR) | p-Value | Before the Pandemic Median (IQR) | During the Pandemic Median (IQR) | p-Value | |
| Have you reduced the number of times you go out? | 3 (2–4) | 5 (4–5) | <0.001 | 4.5 (2–5) | 5 (4–5) | 0.013 |
| Do you pay attention to the infection control? | 4 (2.75–5) | 5 (5–5) | 0.001 | 5 (3.75 –5) | 5 (4.75 –5) | 0.034 |
| Do you often watch the news? | 4.5 (4–5) | 5 (4–5) | 0.573 | 5 (4–5) | 5 (4.75–5) | 1 |
| Do you often talk to your nurse or your attending physician about your illness? | 4 (3–4) | 4 (3–5) | 0.246 | 4 (4–5) | 4 (3–5) | 0.681 |
| Do you have a lot of anxiety? | 4 (2.75–4) | 4 (4–4.25) | 0.042 | 4 (3–5) | 4 (3.5–5) | 0.174 |
| Did you have insomnia? | 3 (2–4) | 3 (3–4) | 0.037 | 2 (1–3) | 3 (1–4) | 0.181 |
| Do you experience extreme sadness sometimes? | 3 (2–3.5) | 3 (3–4) | 0.073 | 2 (1–3) | 2 (1–3) | 1 |
| Do you have financial concerns? | 3 (2.5–4) | 3 (3–4) | 0.265 | 2 (1–4) | 2 (1–4) | 1 |
| Do you tend to reduce the number of hospital visit? | 3 (2–3.25) | 3 (2.75–4) | 0.187 | 3 (1–3.25) | 3 (1.75–4.25) | 0.281 |
| Do you want to receive the cancer treatment at the hospital? | 2 (1–3) | 2.5 (1–3) | 1 | 1.5 (1–3.25) | 2 (1–3.25) | 0.71 |
| Do you not want to receive the cancer treatment? | 2.5 (1.75–4) | 3 (2–3.25) | 0.691 | 3 (1–4) | 3 (1–4) | 0.481 |
| Would you like to switch to a treatment that requires fewer visits? | 3 (2.75–4) | 3 (3–4) | 0.573 | 3 (3–5) | 3.5(3–5) | 0.481 |
| Do you want to switch from intravenous regimens to oral regimens? | 3 (2–4) | 3 (2.75–3) | 0.523 | 3 (2.75–3) | 3 (2.00–3.25) | 0.577 |
| Do you want a longer drug holiday to reduce the number of hospital visits? | 3 (2–3.25) | 3 (2.75–3) | 0.702 | 3 (1.5–4) | 3 (2–5) | 0.235 |
| Do you want to receive chemotherapy that is effective but has stronger side effects? | 3 (3–4) | 3 (3–4) | 0.425 | 3 (2–4) | 4 (3–4.5) | 0.261 |
| Do you think it is acceptable to postpone a CT scan for 1–2 months? | 3 (2–3) | 3 (2–3) | 0.255 | 3 (2–4) | 3 (2–4) | 1 |
| Do you often look at our hospital’s website? | 1 (1–2) | 1.5 (1–3) | 0.054 | 1 (1–2) | 1 (1–2) | 0.346 |
| Do you feel that the hospital is taking sufficient measures against the spread of infections? | 4 (3–5) | 4 (3–5) | 0.018 | 4 (4–5) | 4 (3.75–5) | 0.11 |
| Male | Female | |||||
|---|---|---|---|---|---|---|
| Before the Pandemic Median (IQR) | During the Pandemic Median (IQR) | p-Value | Before the Pandemic Median (IQR) | During the Pandemic Median (IQR) | p-Value | |
| Have you reduced the number of times you go out? | 3 (2–4.5) | 5 (4–5) | <0.001 | 4 (3.5–5) | 5(4.5–5) | 0.034 |
| Do you pay attention to the infection control? | 4 (2–5) | 5 (4.5 –5) | 0.002 | 5(4–5) | 5(5–5) | 0.041 |
| Do you often watch the news? | 4 (4–5) | 5 (4–5) | 0.49 | 5(4–5) | 5(4–5) | 0.67 |
| Do you often talk to your nurse or your attending physician about your illness? | 4 (3.5–4) | 4 (3.5–5) | 0.118 | 4 (3–4) | 3 (3–4) | 0.189 |
| Do you have a lot of anxiety? | 4 (3–4) | 4 (3.25–4.75) | 0.086 | 4 (3.5–4) | 4 (4–5) | 0.098 |
| Did you have insomnia? | 3 (1–3) | 3 (3–4) | 0.02 | 3 (2–4) | 3 (2–4) | 0.384 |
| Do you experience extreme sadness sometimes? | 2 (2–4) | 3 (1–4) | 0.417 | 2 (2–3) | 2 (2–3) | 0.384 |
| Do you have financial concerns? | 3 (3–4) | 3 (3–5) | 0.161 | 2 (2–3) | 2 (1.5–3) | 1 |
| Do you tend to reduce the number of hospital visit? | 3 (1–3) | 3 (2–4) | 0.094 | 3 (2–3.5) | 3 (2–4) | 0.271 |
| Do you want to receive the cancer treatment at the hospital? | 3 (1–3) | 3 (1–3) | 0.846 | 2 (1–3) | 2 (1–3) | 0.334 |
| Do you not want to receive the cancer treatment? | 2 (1–4) | 3 (1–4) | 0.527 | 3 (2–4) | 3 (2.5–4.5) | 0.582 |
| Would you like to switch to a treatment that requires fewer visits? | 3 (2.5–4) | 3 (3–4) | 0.574 | 3 (3–4.5) | 3 (3–4) | 0.582 |
| Do you want to switch from intravenous regimens to oral regimens? | 3 (2.5–3.5) | 3 (2–3) | 0.265 | 3 (2–3) | 3 (2.5–3) | 0.164 |
| Do you want a longer drug holiday to reduce the number of hospital visits? | 3 (2–3) | 3 (2.25–3) | 0.587 | 3 (2–4) | 3 (2–3.5) | 0.582 |
| Do you want to receive chemotherapy that is effective but has stronger side effects? | 3 (2–4) | 4 (3–4) | 0.294 | 4 (3–4) | 4 (3–4) | 0.855 |
| Do you think it is acceptable to postpone a CT scan for 1–2 months? | 3 (3–4) | 3 (3–4) | 1 | 3 (2–3) | 3 (2–3) | 0.334 |
| Do you often look at our hospital’s website? | 1 (1–2) | 1 (1–2) | 0.212 | 1 (1–2) | 1 (1–2.5) | 0.164 |
| Do you feel that the hospital is taking sufficient measures against the spread of infections? | 4 (4–5) | 5 (4–5) | 0.031 | 4 (3–4.5) | 4 (3–4) | 0.433 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Taira, K.; Nagahara, H.; Tanaka, H.; Kimura, A.; Nakata, A.; Iseki, Y.; Fukuoka, T.; Shibutani, M.; Toyokawa, T.; Lee, S.; et al. Impact of the COVID-19 Pandemic on Patients with Gastrointestinal Cancer Undergoing Active Cancer Treatment in an Ambulatory Therapy Center: The Patients’ Perspective. Healthcare 2021, 9, 1688. https://doi.org/10.3390/healthcare9121688
Taira K, Nagahara H, Tanaka H, Kimura A, Nakata A, Iseki Y, Fukuoka T, Shibutani M, Toyokawa T, Lee S, et al. Impact of the COVID-19 Pandemic on Patients with Gastrointestinal Cancer Undergoing Active Cancer Treatment in an Ambulatory Therapy Center: The Patients’ Perspective. Healthcare. 2021; 9(12):1688. https://doi.org/10.3390/healthcare9121688
Chicago/Turabian StyleTaira, Koichi, Hisashi Nagahara, Hiroaki Tanaka, Akie Kimura, Akinobu Nakata, Yasuhito Iseki, Tatsunari Fukuoka, Masatsune Shibutani, Takahiro Toyokawa, Shigeru Lee, and et al. 2021. "Impact of the COVID-19 Pandemic on Patients with Gastrointestinal Cancer Undergoing Active Cancer Treatment in an Ambulatory Therapy Center: The Patients’ Perspective" Healthcare 9, no. 12: 1688. https://doi.org/10.3390/healthcare9121688