
Cognitive Aid for Anesthetic Preparation in An Emergency Situation: A Simulation-Based Study

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Environment and Conduct of Sessions
2.2.1. First Phase
Briefing
Simulation and Assessment
Debriefing
Anxiety
2.2.2. Second Phase
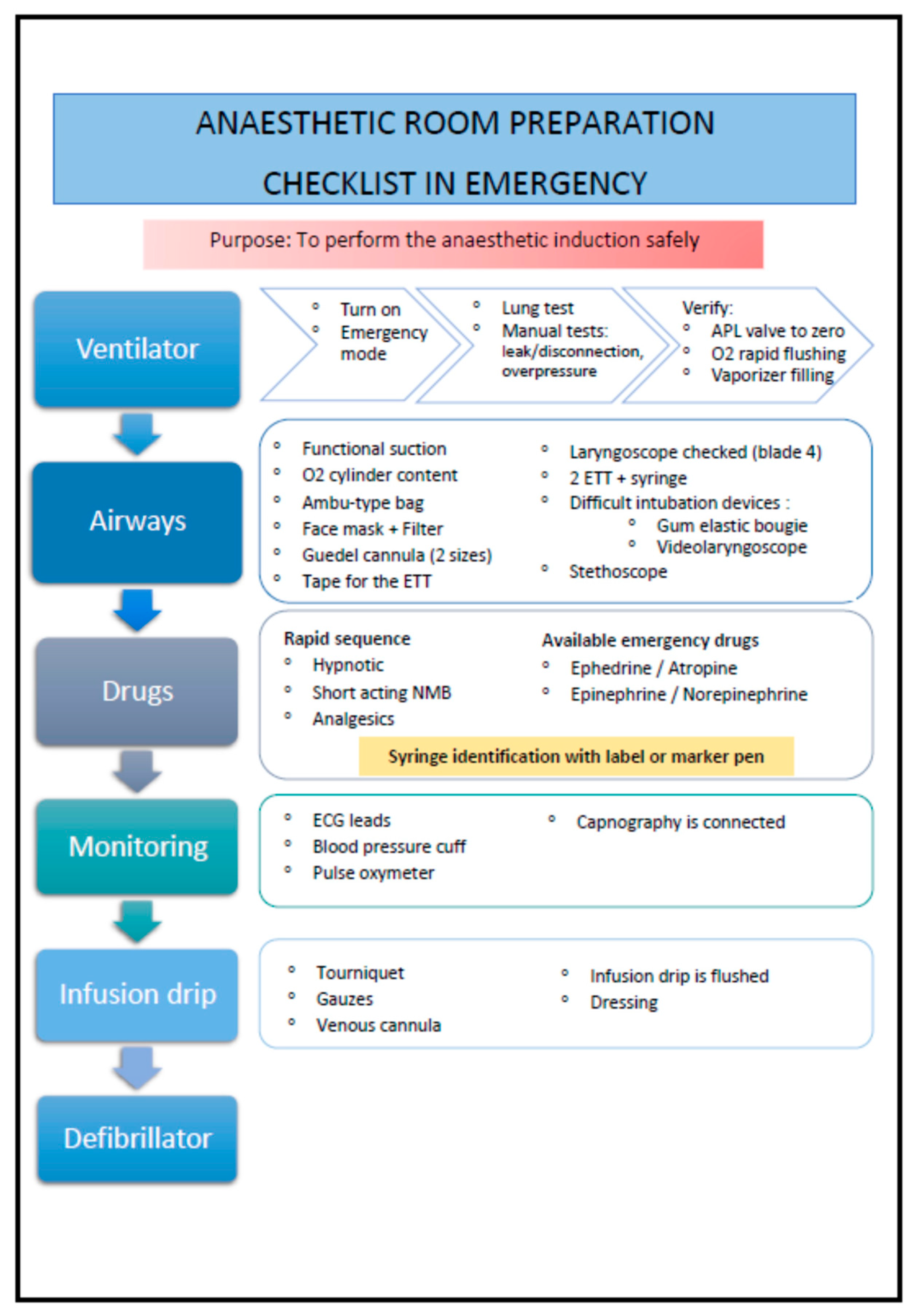
2.3. Exhaustive Checklist and Essential Items
2.4. Outcomes
2.5. Statistical Analysis
3. Results
3.1. Population Characteristics
3.2. Primary Endpoint
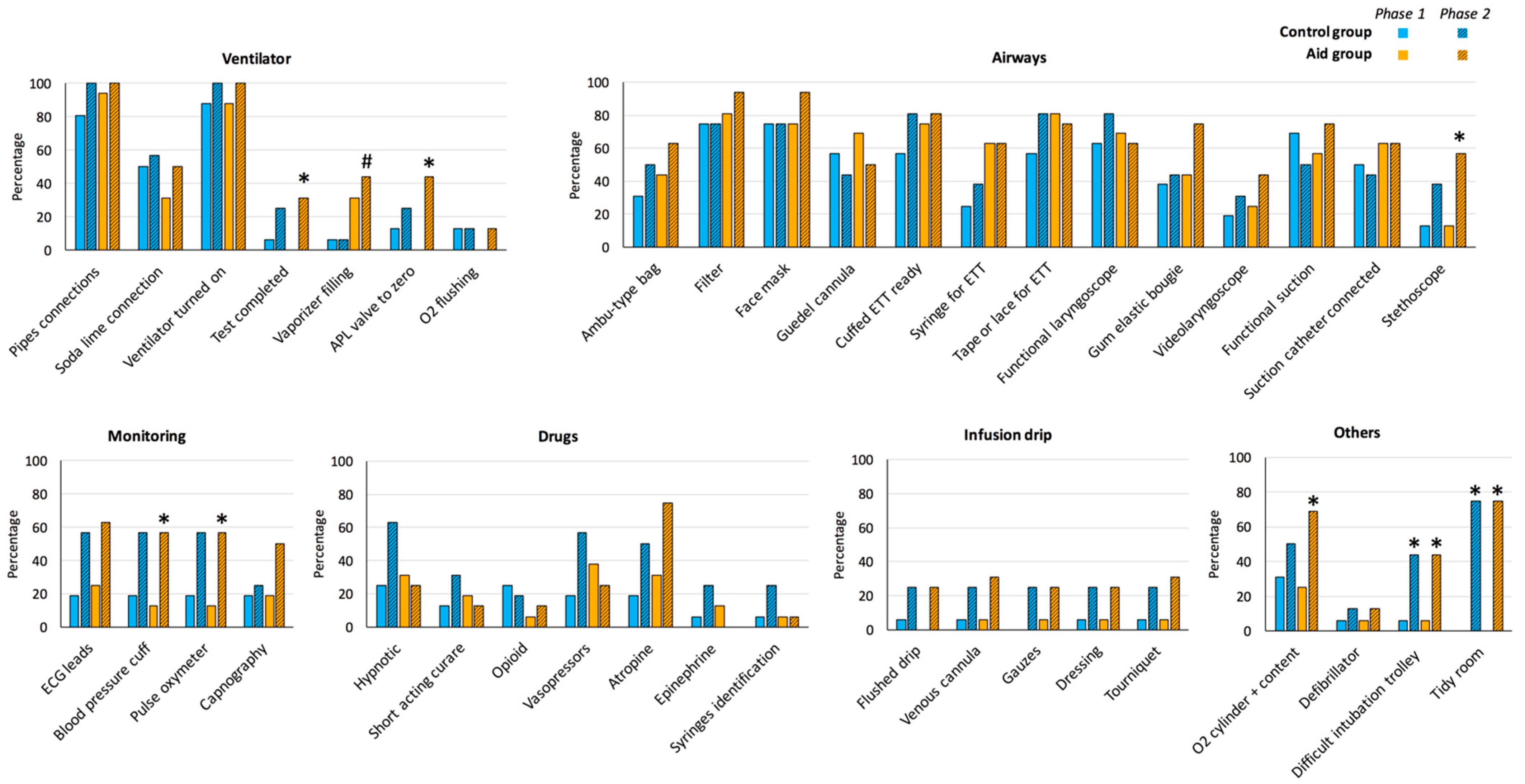
3.3. Number and Details of Completed Items in Both Phases
3.3.1. First Phase
3.3.2. Second Phase
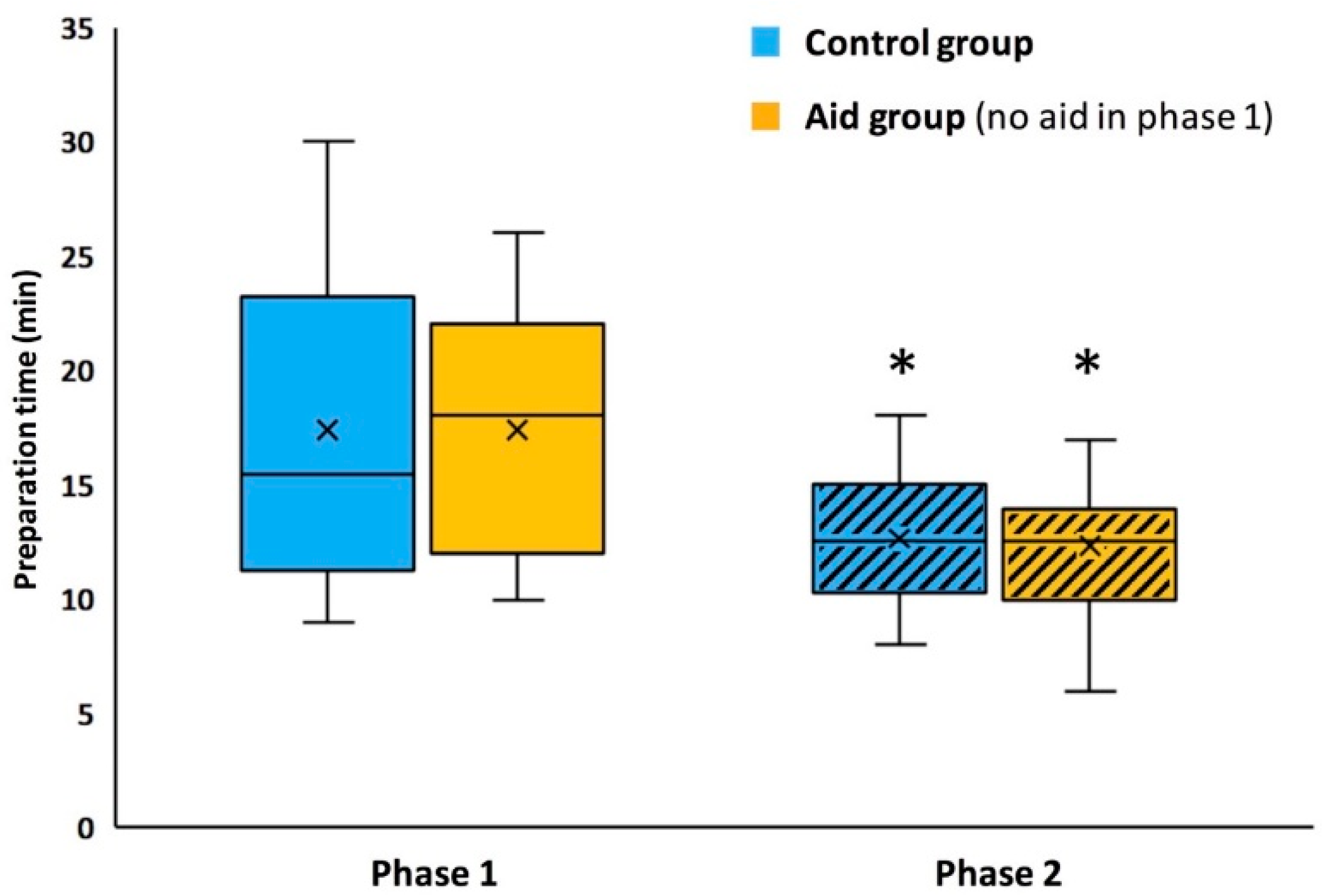
3.4. Duration
3.5. Anxiety
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization; World Alliance for Patient Safety. WHO Guidelines for Safe Surgery 2009; World Health Organization: Geneva, Switzerland, 2009; ISBN 978-92-4-159855-2. [Google Scholar]
- Haynes, A.B.; Weiser, T.G.; Berry, W.R.; Lipsitz, S.R.; Breizat, A.-H.S.; Dellinger, E.P.; Herbosa, T.; Joseph, S.; Kibatala, P.L.; Lapitan, M.C.M.; et al. A Surgical Safety Checklist to Reduce Morbidity and Mortality in a Global Population. N. Engl. J. Med. 2009, 360, 491–499. [Google Scholar] [CrossRef]
- Association of Anaesthetists of Great Britain and Ireland (AAGBI); Hartle, A.; Anderson, E.; Bythell, V.; Gemmell, L.; Jones, H.; McIvor, D.; Pattinson, A.; Sim, P.; Walker, I. Checking Anaesthetic Equipment 2012: Association of Anaesthetists of Great Britain and Ireland. Anaesthesia 2012, 67, 660–668. [Google Scholar] [CrossRef]
- Cassinello, F.; Ariño, J.J.; Bartolomé Ruibal, A.; de la Pinta, J.C.; de la Quintana, F.B.; Espinosa, M.E.; Gilsanz, F.; Gómez-Arnau, J.; González Arévalo, A.; López-Quero, L.; et al. Spanish Society of Anaesthesia (SEDAR) guidelines for pre-anaesthesia checking procedures. Rev. Esp. Anestesiol. Reanim. 2012, 59, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Goneppanavar, U.; Prabhu, M. Anaesthesia machine: Checklist, hazards, scavenging. Indian J. Anaesth. 2013, 57, 533–540. [Google Scholar] [CrossRef] [PubMed]
- Spofford, C.M.; Bayman, E.O.; Szeluga, D.J.; From, R.P. Anesthesia machine checkout and room setup: A randomized, single-blind, comparison of two teaching modalities. J. Educ. Perioper. Med. 2012, 14, E060. [Google Scholar] [PubMed]
- Sexton, J.B.; Thomas, E.J.; Helmreich, R.L. Error, Stress, and Teamwork in Medicine and Aviation: Cross Sectional Surveys. BMJ 2000, 320, 745–749. [Google Scholar] [CrossRef] [Green Version]
- Geeraerts, T.; Le Guen, M. Checklists and Cognitive Aids in Simulation Training and Daily Critical Care Practice: Simple Tools to Improve Medical Performance and Patient Outcome. Anaesth. Crit. Care Pain Med. 2018, 37, 3–4. [Google Scholar] [CrossRef]
- Siddiqui, A.; Ng, E.; Burrows, C.; McLuckie, D.; Everett, T. Impact of Critical Event Checklists on Anaesthetist Performance in Simulated Operating Theatre Emergencies. Cureus 2019, 11, e4376. [Google Scholar] [CrossRef] [Green Version]
- Neal, J.M.; Hsiung, R.L.; Mulroy, M.F.; Halpern, B.B.; Dragnich, A.D.; Slee, A.E. ASRA Checklist Improves Trainee Performance During a Simulated Episode of Local Anesthetic Systemic Toxicity. Reg. Anesth. Pain. Med. 2012, 37, 8–15. [Google Scholar] [CrossRef]
- L’Her, E.; Geeraerts, T.; Desclefs, J.-P.; Benhamou, D.; Blanié, A.; Cerf, C.; Delmas, V.; Jourdain, M.; Lecomte, F.; Ouanes, I.; et al. Simulation-Based Teaching in Critical Care, Anaesthesia and Emergency Medicine. Anaesth. Crit. Care Pain Med. 2020, 39, 311–326. [Google Scholar] [CrossRef]
- Lamé, G.; Dixon-Woods, M. Using Clinical Simulation to Study How to Improve Quality and Safety in Healthcare. BMJ Simul. Technol. Enhanc. Learn. 2020, 6, 87–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, R.; Plahouras, J.; Johnston, B.C.; Scaffidi, M.A.; Grover, S.C.; Walsh, C.M. Virtual Reality Simulation Training in Endoscopy: A Cochrane Review and Meta-Analysis. Endoscopy 2019, 51, 653–664. [Google Scholar] [CrossRef] [PubMed]
- Arriaga, A.F.; Bader, A.M.; Wong, J.M.; Lipsitz, S.R.; Berry, W.R.; Ziewacz, J.E.; Hepner, D.L.; Boorman, D.J.; Pozner, C.N.; Smink, D.S.; et al. Simulation-Based Trial of Surgical-Crisis Checklists. Available online: https://www.nejm.org/doi/10.1056/NEJMsa1204720 (accessed on 27 November 2021).
- Spielberger, C.; Gorsuch, R.; Lushene, R.; Vagg, P.; Jacobs, G. Manual for the State-Trait Anxiety Inventory (Form Y1–Y2); CA: Consulting Psychologists Press: Palo Alto, VA, USA, 1983; Volume IV. [Google Scholar]
- Bauer, C.; Rimmelé, T.; Duclos, A.; Prieto, N.; Cejka, J.-C.; Carry, P.-Y.; Grousson, S.; Friggeri, A.; Secco, J.; Bui-Xuan, B.; et al. Anxiety and Stress among Anaesthesiology and Critical Care Residents during High-Fidelity Simulation Sessions. Anaesth. Crit. Care Pain Med. 2016, 35, 407–416. [Google Scholar] [CrossRef] [PubMed]
- Evain, J.-N.; Zoric, L.; Mattatia, L.; Picard, O.; Ripart, J.; Cuvillon, P. Residual Anxiety after High Fidelity Simulation in Anaesthesiology: An Observational, Prospective, Pilot Study. Anaesth. Crit. Care Pain Med. 2017, 36, 205–212. [Google Scholar] [CrossRef]
- Société Française d’Anesthésie et de Réanimation. L’appareil d’anesthésie et sa vérification avant utilisation-La SFAR. 2015. Available online: https://sfar.org/lappareil-danesthesie-et-sa-verification-avant-utilisation/ (accessed on 27 November 2021).
- Société Française d’Anesthésie et de Réanimation. L’équipement d’un site ou d’un ensemble de sites d’anesthésie-La SFAR. 2015. Available online: https://sfar.org/lequipement-dun-site-ou-dun-ensemble-de-sites-danesthesie/ (accessed on 27 November 2021).
- The Royal College of Anaesthetists. Preparing Your Theatre. Available online: https://www.rcoa.ac.uk/documents/novice-guide/preparing-your-theatre (accessed on 27 November 2021).
- Watkins, S.C.; Anders, S.; Clebone, A.; Hughes, E.; Zeigler, L.; Patel, V.; Shi, Y.; Shotwell, M.S.; McEvoy, M.; Weinger, M.B. Paper or Plastic? Simulation Based Evaluation of Two Versions of a Cognitive Aid for Managing Pediatric Peri-Operative Critical Events by Anesthesia Trainees: Evaluation of the Society for Pediatric Anesthesia Emergency Checklist. J. Clin. Monit. Comput. 2016, 30, 275–283. [Google Scholar] [CrossRef] [PubMed]
- Blanié, A.; Kurrek, M.; Gorse, S.; Baudrier, D.; Benhamou, D. Use of Cognitive Aids: Results from a National Survey among Anaesthesia Providers in France and Canada. Anesthesiol. Res. Pract. 2020, 2020, 1346051. [Google Scholar] [CrossRef] [PubMed]
- Marshall, S. The Use of Cognitive Aids during Emergencies in Anesthesia: A Review of the Literature. Anesth. Analg. 2013, 117, 1162–1171. [Google Scholar] [CrossRef] [Green Version]
- Société Française d’Anesthésie et de Réanimation. Aides Cognitives en Anesthésie Réanimation-La SFAR. Available online: https://sfar.org/espace-professionel-anesthesiste-reanimateur/outils-professionnels/boite-a-outils/aides-cognitives-en-anesthesie-reanimation/ (accessed on 27 November 2021).
- Cook, D.A.; Hatala, R.; Brydges, R.; Zendejas, B.; Szostek, J.H.; Wang, A.T.; Erwin, P.J.; Hamstra, S.J. Technology-Enhanced Simulation for Health Professions Education: A Systematic Review and Meta-Analysis. JAMA 2011, 306, 978–988. [Google Scholar] [CrossRef]
- Lorello, G.R.; Cook, D.A.; Johnson, R.L.; Brydges, R. Simulation-Based Training in Anaesthesiology: A Systematic Review and Meta-Analysis. Br. J. Anaesth. 2014, 112, 231–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hubert, V.; Duwat, A.; Deransy, R.; Mahjoub, Y.; Dupont, H. Effect of Simulation Training on Compliance with Difficult Airway Management Algorithms, Technical Ability, and Skills Retention for Emergency Cricothyrotomy. Anesthesiology 2014, 120, 999–1008. [Google Scholar] [CrossRef] [Green Version]
- Kolawole, H.; Guttormsen, A.B.; Hepner, D.L.; Kroigaard, M.; Marshall, S. Use of Simulation to Improve Management of Perioperative Anaphylaxis: A Narrative Review. Br. J. Anaesth. 2019, 123, e104–e109. [Google Scholar] [CrossRef] [PubMed]
- Hardy, J.-B.; Gouin, A.; Damm, C.; Compère, V.; Veber, B.; Dureuil, B. The Use of a Checklist Improves Anaesthesiologists’ Technical and Non-Technical Performance for Simulated Malignant Hyperthermia Management. Anaesth. Crit. Care Pain Med. 2018, 37, 17–23. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Demographic Data | Control Group (n = 16) | Aid Group (n = 16) | p |
|---|---|---|---|
| Age, year | 27 (25–28) | 27 (26–29) | 0.54 |
| Sex, male | 8 (50%) | 11 (69%) | 0.47 |
| Anesthesia training level, year | 3.5 (2–4) | 3 (2–4) | 0.65 |
| Phase 1 | Phase 2 | Paired Comparison Phase 1 vs. 2 | ||||
|---|---|---|---|---|---|---|
| Control (n = 16) | Aid (n = 16) | Control (n = 16) | Aid (n = 16) | p, Control Group | p, Aid Group | |
| First 5 min | 12 (8–15) | 13 (10–16) | 16 (13–23) | 21 (15–22) | 0.0011 | 0.0003 |
| Without time limit | 30 (24–33) | 30 (27–33) | 32 (29–34) | 34 (29–38) | 0.0381 | 0.0196 |
| Phase 1 | Phase 2 | Paired Comparison Phase 1 vs. 2 | ||||
|---|---|---|---|---|---|---|
| Control (n = 16) | Aid (n = 16) | Control (n = 16) | Aid (n = 16) | p for Control Group | p for Aid Group | |
| STAI YA | 28 (24–32) | 28 (25–38) | 30 (23–34) | 29 (23–32) | 0.84 | 0.37 |
| STAI YB | 33 (31–41) | 36 (30–39) | 35 (31–43) | 33 (31–39) | 0.67 | 0.66 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rineau, E.; Collard, A.; Jean, L.; Guérin, S.; Maunoury, L.; Martin, L.; Lasocki, S.; Léger, M. Cognitive Aid for Anesthetic Preparation in An Emergency Situation: A Simulation-Based Study. Healthcare 2021, 9, 1646. https://doi.org/10.3390/healthcare9121646
Rineau E, Collard A, Jean L, Guérin S, Maunoury L, Martin L, Lasocki S, Léger M. Cognitive Aid for Anesthetic Preparation in An Emergency Situation: A Simulation-Based Study. Healthcare. 2021; 9(12):1646. https://doi.org/10.3390/healthcare9121646
Chicago/Turabian StyleRineau, Emmanuel, Anna Collard, Lorine Jean, Sarah Guérin, Louise Maunoury, Ludovic Martin, Sigismond Lasocki, and Maxime Léger. 2021. "Cognitive Aid for Anesthetic Preparation in An Emergency Situation: A Simulation-Based Study" Healthcare 9, no. 12: 1646. https://doi.org/10.3390/healthcare9121646