
Factors That Influence Mortality in Critically Ill Patients with SARS-CoV-2 Infection: A Multicenter Study in the Kingdom of Saudi Arabia

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Setting
2.2. Sample Selection and Subjects
2.3. Data Source and Instruments
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Salata, C.; Calistri, A.; Parolin, C.; Palù, G. Coronaviruses: A paradigm of new emerging zoonotic diseases. Pathog. Dis. 2019, 77, ftaa006. [Google Scholar] [CrossRef] [Green Version]
- Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). Coronavirus COVID-19 Global Cases by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). 2020. Available online: https://coronavirus.jhu.edu/map-faq (accessed on 4 August 2021).
- Yezli, S.; Khan, A. COVID-19 social distancing in the Kingdom of Saudi Arabia: Bold measures in the face of political, economic, social and religious challenges. Travel Med. Infect. Dis. 2020, 37, 101692. [Google Scholar] [CrossRef] [PubMed]
- Al-Tawfiq, J.A.; Memish, Z.A. COVID-19 in the Eastern Mediterranean region and Saudi Arabia: Prevention and therapeutic strategies. Int. J. Antimicrob. Agents 2020, 55, 105968. [Google Scholar] [CrossRef]
- Ministry of Health, Kingdom of Saudi Arabia. COVID-19 Statistics. 2021. Available online: https://covid19.moh.gov.sa/ (accessed on 4 August 2021).
- BaHammam, A.S.; Bindayna, K.M.; Joji, R.M.; Jahrami, H.; Faris, M.A.E.; Bragazzi, N.L. Outcomes of COVID-19 in the Eastern Mediterranean Region in the first 4 months of the pandemic. Saudi Med. J. 2020, 41, 907–915. [Google Scholar] [CrossRef]
- Shi, C.; Wang, L.; Ye, J.; Gu, Z.; Wang, S.; Xia, J.; Xie, Y.; Li, Q.; Xu, R.; Lin, N. Predictors of mortality in patients with coronavirus disease 2019: A systematic review and meta-analysis. BMC Infect. Dis. 2021, 21, 663. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, N.T.; Chinn, J.; De, F.M.; Kirby, K.A.; Hohmann, S.F.; Amin, A. Male gender is a predictor of higher mortality in hospitalized adults with COVID-19. PLoS ONE 2021, 16, e0254066. [Google Scholar] [CrossRef]
- Al-Jarallah, M.; Rajan, R.; Al Saber, A.; Pan, J.; Al-Sultan, A.T.; Abdelnaby, H.; Alroomi, M.; Dashti, R.; Aboelhassan, W.; Almutairi, F.; et al. In-hospital mortality in SARS-CoV-2 stratified by hemoglobin levels: A retrospective study. EJHaem 2021, 2, 335–339. [Google Scholar] [CrossRef] [PubMed]
- Martinot, M.; Eyriey, M.; Gravier, S.; Bonijoly, T.; Kayser, D.; Ion, C.; Mohseni-Zadeh, M.; Camara, S.; Dubois, J.; Haerrel, E.; et al. Predictors of mortality, ICU hospitalization, and extrapulmonary complications in COVID-19 patients. Infect. Dis. Now. 2021, 51, 518–525. [Google Scholar] [CrossRef]
- Mehta, H.B.; Li, S.; Goodwin, J.S. Risk factors associated with SARS-CoV-2 infections, hospitalization, and mortality among US nursing home residents. JAMA Netw. Open. 2021, 4, e216315. [Google Scholar] [CrossRef] [PubMed]
- Alswaidi, F.M.; Assiri, A.M.; Alhaqbani, H.H.; Alalawi, M.M. Characteristics and outcome of COVID-19 cases in Saudi Arabia: Review of six-months of data (March–August 2020). Saudi Pharm. J. 2021, 29, 682–691. [Google Scholar] [CrossRef] [PubMed]
- Alsofayan, Y.M.; Althunayyan, S.M.; Khan, A.A.; Hakawi, A.M.; Assiri, A.M. Clinical characteristics of COVID-19 in Saudi Arabia: A national retrospective study. J. Infect. Public Health 2020, 13, 920–925. [Google Scholar] [CrossRef] [PubMed]
- Faqihi, F.; Alharthy, A.; Abdulaziz, S.; Balhamar, A.; Alomari, A.; AlAseri, Z.; Tamim, H.; Alqahtani, S.A.; Kutsogiannis, D.J.; Brindley, P.G.; et al. Therapeutic plasma exchange in patients with life-threatening COVID-19: A randomised controlled clinical trial. Int. J. Antimicrob. Agents 2021, 57, 106334. [Google Scholar] [CrossRef] [PubMed]
- Amer, M.; Kamel, A.M.; Bawazeer, M.; Maghrabi, K.; Butt, A.; Dahhan, T.; Kseibi, E.; Khurshid, S.M.; Abujazar, M.; Alghunaim, R.; et al. Clinical characteristics and outcomes of critically ill mechanically ventilated COVID-19 patients receiving interleukin-6 receptor antagonists and corticosteroid therapy: A preliminary report from a multinational registry. Eur. J. Med. Res. 2021, 26, 1–12. [Google Scholar] [CrossRef]
- Liu, S.; Yao, N.; Qiu, Y.; He, C. Predictive performance of SOFA and qSOFA for in-hospital mortality in severe novel coronavirus disease. Am. J. Emerg. Med. 2020, 38, 2074–2080. [Google Scholar] [CrossRef] [PubMed]
- Pierce, C.B.; Muñoz, A.; Ng, D.K.; Warady, B.A.; Furth, S.L.; Schwartz, G.J. Age- and sex-dependent clinical equations to estimate glomerular filtration rates in children and young adults with chronic kidney disease. Kidney Int. 2021, 99, 948–956. [Google Scholar] [CrossRef]
- Zappitelli, M.; Parikh, C.R.; Kcan-Arikan, A.; Washburn, K.K.; Moffett, B.S.; Goldstein, S.L. Ascertainment and epidemiology of acute kidney injury varies with definition interpretation. Clin. J. Am. Soc. Nephrol. 2008, 3, 948–954. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, R.A.; Kane, A.D.; Cook, T.M. Outcomes from intensive care in patients with COVID-19: A systematic review and meta-analysis of observational studies. Anaesthesia 2020, 75, 1340–1349. [Google Scholar] [CrossRef]
- The African COVID-19 Critical Care Outcomes Study (ACCCOS) Investigators. Patient care and clinical outcomes for patients with COVID-19 infection admitted to African high-care or intensive care units (ACCCOS): A multicentre, prospective, observational cohort study. Lancet 2021, 397, 1885–1894. [Google Scholar] [CrossRef]
- Elhadi, M.; Alsoufi, A.; Abusalama, A.; Alkaseek, A.; Abdeewi, S.; Yahya, M.; Mohammed, A.; Abdelkabir, M.; Huwaysh, M.; Amkhatirah, E.; et al. Epidemiology, outcomes, and utilization of intensive care unit resources for critically ill COVID-19 patients in Libya: A prospective multi-center cohort study. PLoS ONE 2021, 16, e0251085. [Google Scholar] [CrossRef]
- Murthy, S.; Archambault, P.M.; Atique, A.; Carrier, F.M.; Cheng, M.P.; Codan, C.; Daneman, N.; Dechert, W.; Douglas, S.; Fiest, K.M.; et al. Characteristics and outcomes of patients with COVID-19 admitted to hospital and intensive care in the first phase of the pandemic in Canada: A national cohort study. CMAJ Open 2021, 9, E181–E188. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Li, H.; Zhang, Z.; Liang, W.; Zhang, T.; Tong, Z.; Guo, X.; Qi, X. Risk factors for mortality of coronavirus disease 2019 (COVID-19) patients during the early outbreak of COVID-19: A systematic review and meta-analysis. Ann. Palliat. Med. 2021, 10, 5069–5083. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.Y.; Li, H.Y.; Xu, X.B.; Zheng, K.X.; Qi, X.S.; Guo, X.Z. Clinical features and outcome of treatment for novel coronavirus pneumonia: A meta-analysis. Zhonghua Gan Zang Bing Za Zhi 2020, 28, 240–246. [Google Scholar] [CrossRef]
- Hu, Y.; Sun, J.; Dai, Z.; Deng, H.; Li, X.; Huang, Q.; Wu, Y.; Sun, L.; Xu, Y. Prevalence and severity of corona virus disease 2019 (COVID-19): A systematic review and meta-analysis. J. Clin. Virol. 2020, 127, 104371. [Google Scholar] [CrossRef]
- AlFattani, A.; AlMeharish, A.; Nasim, M.; AlQahtani, K.; AlMudraa, S. Ten public health strategies to control the Covid-19 pandemic: The Saudi Experience. IJID Regions 2021, 1, 12–19. [Google Scholar] [CrossRef]
- Taylor, E.H.; Marson, E.J.; Elhadi, M.; Macleod, K.D.M.; Yu, J.C.; Davids, R.; Boden, R.; Overmeyer, R.C.; Ramakrishnan, R.; Thomson, D.A.; et al. Factors associated with mortality in patients with COVID-19 admitted to intensive care: A systematic review and meta-analysis. Anaesthesia 2021, 76, 1224–1232. [Google Scholar] [CrossRef]
- Hofmeyr, R.; Earle, E.; Boden, R.; Nejthardt, M.; Torborg, A.; Van der Spuy, K.; Kabambi, K.; Isaacs, M.; Usenbo, A.; Chen, A.; et al. Risk factors and interventions associated with mortality or survival in adult COVID-19 patients admitted to critical care: A systematic review and meta-analysis. South. Afr. J. Anaesth. Analg. 2020, 26, 116–127. [Google Scholar] [CrossRef]
- Ruiz-Sánchez, J.G.; Núñez-Gil, I.J.; Cuesta, M.; Rubio, M.A.; Mauron-Eid, C.; Arroyo-Espliguero, R.; Romero, R.; Becerra-Muñoz, V.M.; Uribarri, A.; Feltes, G.; et al. Prognostic Impact of Hyponatremia and Hypernatremia in COVID-19 Pneumonia. A HOPE-COVID-19 (Health Outcome Predictive Evaluation for COVID-19) Registry Analysis. Front. Endocrinol. (Lausanne) 2020, 11, 599255. [Google Scholar] [CrossRef]
- Sjöström, A.; Rysz, S.; Sjöström, H.; Höybye, C. Electrolyte and acid-base imbalance in severe COVID-19. Endocr. Connect. 2021, 10, 805–814. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.; Wu, D.; Chen, H.; Yan, W.; Yang, D.; Chen, G.; Ma, K.; Xu, D.; Yu, H.; Wang, H.; et al. Clinical characteristics of 113 deceased patients with coronavirus disease 2019: Retrospective study. BMJ. 2020, 368, m1091. [Google Scholar] [CrossRef] [Green Version]
- Lanini, S.; Montaldo, C.; Nicastri, E.; Vairo, F.; Agrati, C.; Petrosillo, N.; Scognamiglio, P.; Antinori, A.; Puro, V.; Di Caro, A.; et al. COVID-19 disease-Temporal analyses of complete blood count parameters over course of illness, and relationship to patient demographics and management outcomes in survivors and non-survivors: A longitudinal descriptive cohort study. PLoS ONE 2020, 15, e0244129. [Google Scholar] [CrossRef]
- Gutiérrez-Abejón, E.; Martín-García, D.; Tamayo, E.; Álvarez, F.J.; Herrera-Gómez, F. Clinical profile, pharmacological treatment, and predictors of death among hospitalized COVID-19 patients with acute kidney injury: A population-based registry analysis. Front. Med. 2021, 8, 657977. [Google Scholar] [CrossRef] [PubMed]
- Alfano, G.; Ferrari, A.; Fontana, F.; Mori, G.; Magistroni, R.; Meschiari, M.; Franceschini, E.; Menozzi, M.; Cuomo, G.; Orlando, G.; et al. Incidence, risk factors and outcome of acute kidney injury (AKI) in patients with COVID-19. Clin. Exp. Nephrol. 2021, 25, 1203–1214. [Google Scholar] [CrossRef] [PubMed]
- Neves, P.D.M.D.M.; Sato, V.A.H.; Mohrbacher, S.; Ferreira, B.M.C.; Oliveira, É.S.; Pereira, L.V.B.; Bales, A.M.; Nardotto, L.L.; Ferreira, J.N.; Machado, D.J.; et al. Acute kidney injury due to COVID-19 in intensive care unit: An analysis from a Latin-American center. Front. Med. 2021, 8, 620050. [Google Scholar] [CrossRef]
- Gasparini, M.; Khan, S.; Patel, J.M.; Parekh, D.; Dangash, M.N.; Stümpfle, R.; Shah, A.; Baharlo, B.; Soni, S.; Brett, S.; et al. Renal impairment and its impact on clinical outcomes in patients who are critically ill with COVID-19: A multicentre observational study. Anaesthesia 2021, 76, 320–326. [Google Scholar] [CrossRef] [PubMed]
- de Souza, F.S.H.; Hojo-Souza, N.S.; Batista, B.D.O.; da Silva, C.M.; Guidoni, D.L. On the analysis of mortality risk factors for hospitalized COVID-19 patients: A data-driven study using the major Brazilian database. PLoS One 2021, 16, e0248580. [Google Scholar] [CrossRef] [PubMed]
- De Lorenzo, A.; Kasal, D.A.; Tura, B.R.; Lamas, C.C.; Rey, H.C. Acute cardiac injury in patients with COVID-19. Am. J. Cardiovasc. Dis. 2020, 10, 28–33. [Google Scholar]
- Habets, M.A.W.; Sturkenboom, H.N.; Tio, R.A.; Belfroid, E.; Hoogervorst-Schilp, J.; Siebelink, H.J.; Jansen, C.W.; Smits, P.C. How often and to what extent do admitted COVOD-19 patients have sign of cardiac injury? Neth. Heart J. 2021, 29 (Suppl. 1), 5–12. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Estimate |
|---|---|
| Age (years), mean (SD) | 52.8 (16.6) |
| Male sex, n (%) | 184 (80.4) |
| Saudi nationality, n (%) | 59 (25.8) |
| Body mass index, mean (SD) | 29.1 (13.9) |
| Contact with COVID-19, n (%) | 80 (34.9) |
| Recent travel *, n (%) | 5 (2.2) |
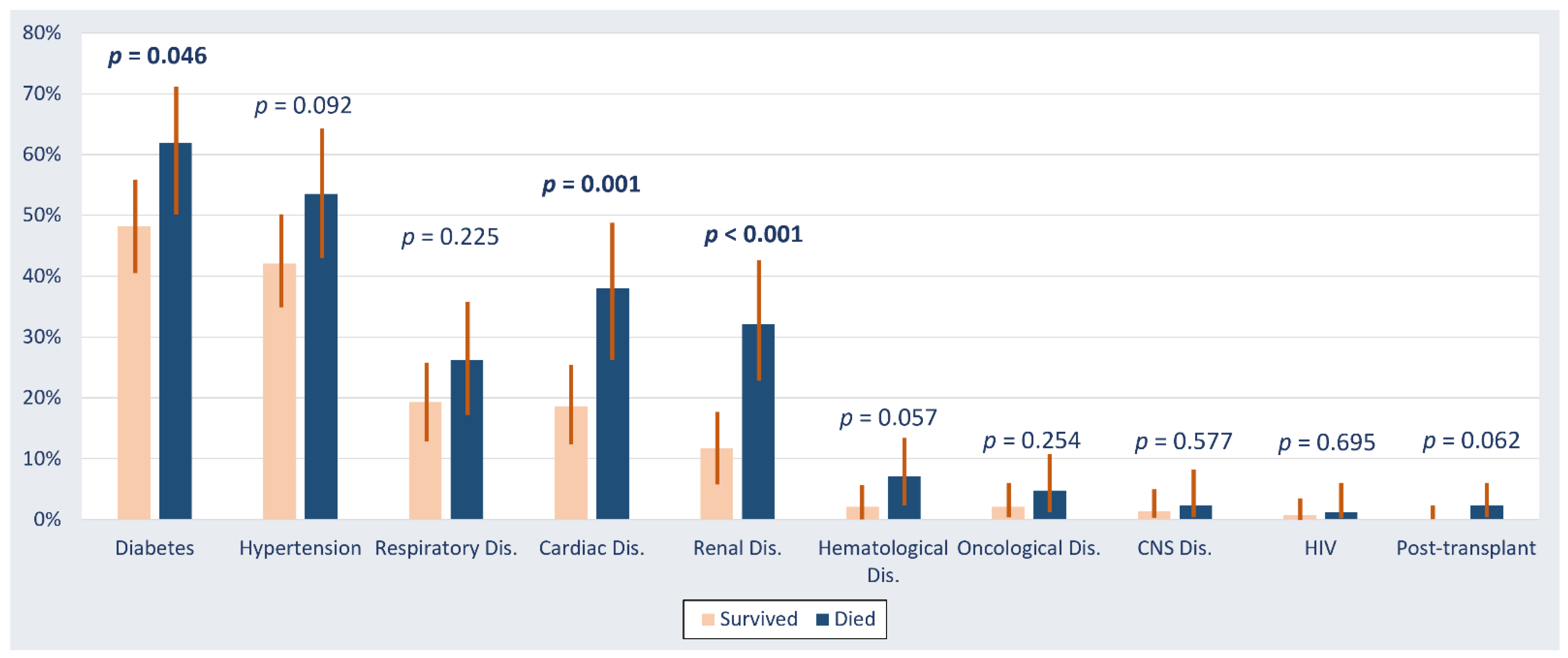
| Comorbidities, n (%) | |
| Diabetes mellitus | 122 (53.3) |
| Hypertension | 106 (46.3) |
| Renal disease | 44 (19.2) |
| Cardiac disease | 59 (25.8) |
| Respiratory disease | 50 (21.8) |
| Hematology disorder | 9 (3.9) |
| Oncology disorder | 7 (3.1) |
| Postsolid organ transplant | 2 (0.9) |
| CNS disorder | 4 (1.8) |
| HIV infection | 2 (0.9) |
| Investigation | Survivors (n = 145) | Nonsurvivors (n = 84) | p-Value |
|---|---|---|---|
| Chest radiography, n (%) | |||
| Normal | 9 (6.3) | 3 (3.7) | 0.225 |
| Mild consolidation | 42 (29.4) | 19 (23.2) | |
| Severe consolidation | 66 (46.2) | 36 (43.9) | |
| ARDS | 26 (18.2) | 24 (29.3) | |
| ECG abnormality, n (%) | 57 (54.3) | 39 (65.0) | 0.180 |
| Low GFR (<90 mL/min/1.73 m2), n (%) | 76 (52.4) | 76 (90.5) | <0.001 |
| Hypernatremia, n (%) | 50 (35.5) | 59 (70.2) | <0.001 |
| Hyponatremia, n (%) | 8 (5.7) | 1 (1.2) | 0.097 |
| Hyperkalemia, n (%) | 53 (37.6) | 61 (72.6) | <0.001 |
| Anemia, n (%) | 51 (37.8) | 58 (70.7) | <0.001 |
| Leukocytosis, n (%) | 91 (67.4) | 75 (91.5) | <0.001 |
| Leukopenia, n (%) | 19 (14.1) | 18 (22.0) | 0.135 |
| Thrombocytopenia, n (%) | 32 (25.4) | 58 (69.1) | <0.001 |
| High aPTT, n (%) | 92 (71.3) | 81 (96.4) | <0.001 |
| High INR, n (%) | 33 (25.6) | 54 (64.3) | <0.001 |
| High D-dimer, n (%) | 112 (97.4) | 84 (100) | 0.136 |
| Acidosis, n (%) | 41 (35.0) | 62 (84.9) | <0.001 |
| High troponin, n (%) | 50 (49.0) | 66 (84.6) | <0.001 |
| High ferritin, n (%) | 32 (27.4) | 73 (86.9) | <0.001 |
| High LDH, n (%) | 126 (96.9) | 83 (100) | 0.107 |
| Abnormal liver enzyme levels, n (%) | 98 (73.7) | 62 (75.6) | 0.753 |
| Characteristics | Crude Estimate | Adjusted Estimate | ||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Age (year) | 1.02 (1.00, 1.04) | 0.049 | 1.00 (0.97, 1.04) | 0.888 |
| Sex | 0.75 (0.38, 1.45) | 0.390 | 0.74 (0.20, 2.79) | 0.655 |
| Diabetes | 1.74 (1.01, 3.01) | 0.047 | 0.82 (0.20, 3.33) | 0.786 |
| Cardiac disease | 2.69 (1.47, 4.94) | 0.001 | 1.41 (0.38, 5.21) | 0.608 |
| Renal disease | 3.57 (1.80, 7.06) | <0.001 | 1.08 (0.24, 4.91) | 0.921 |
| Low GFR * | 8.63 (3.88, 19.16) | <0.001 | 0.90 (0.17, 4.77) | 0.904 |
| Hypernatremia | 4.30 (2.40, 7.68) | <0.001 | 1.16 (0.32, 4.23) | 0.825 |
| Hyperkalemia | 4.40 (2.45, 7.93) | <0.001 | 2.67 (0.73, 9.74) | 0.136 |
| Anemia | 3.98 (2.21, 7.18) | <0.001 | 2.31 (0.63, 8.48) | 0.206 |
| Leukocytosis | 5.18 (2.21, 12.17) | <0.001 | 3.98 (0.86, 18.3) | 0.076 |
| Thrombocytopenia | 6.55 (3.55, 12.09) | <0.001 | 1.36 (0.39, 4.72) | 0.628 |
| High APTT | 10.86 (3.23, 36.6) | <0.001 | 7.44 (1.15, 47.9) | 0.035 |
| High INR | 5.24 (2.88, 9.51) | <0.001 | 4.10 (1.20, 13.8) | 0.025 |
| Acidosis | 10.45 (4.96, 22.0) | <0.001 | 3.75 (1.01, 13.8) | 0.047 |
| High Troponin | 5.72 (2.76, 11.84) | <0.001 | 1.85 (0.40, 8.47) | 0.428 |
| High Ferritin | 17.63 (8.30, 37.4) | <0.001 | 14.4 (4.17, 49.9) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alhasan, K.A.; Shalaby, M.A.; Temsah, M.-H.; Aljamaan, F.; Shagal, R.; AlFaadhel, T.; Alomi, M.; AlMatham, K.; AlHerbish, A.J.; Raina, R.; et al. Factors That Influence Mortality in Critically Ill Patients with SARS-CoV-2 Infection: A Multicenter Study in the Kingdom of Saudi Arabia. Healthcare 2021, 9, 1608. https://doi.org/10.3390/healthcare9121608
Alhasan KA, Shalaby MA, Temsah M-H, Aljamaan F, Shagal R, AlFaadhel T, Alomi M, AlMatham K, AlHerbish AJ, Raina R, et al. Factors That Influence Mortality in Critically Ill Patients with SARS-CoV-2 Infection: A Multicenter Study in the Kingdom of Saudi Arabia. Healthcare. 2021; 9(12):1608. https://doi.org/10.3390/healthcare9121608
Chicago/Turabian StyleAlhasan, Khalid A, Mohamed A Shalaby, Mohamad-Hani Temsah, Fadi Aljamaan, Reem Shagal, Talal AlFaadhel, Mohammed Alomi, Khalid AlMatham, Adi J. AlHerbish, Rupesh Raina, and et al. 2021. "Factors That Influence Mortality in Critically Ill Patients with SARS-CoV-2 Infection: A Multicenter Study in the Kingdom of Saudi Arabia" Healthcare 9, no. 12: 1608. https://doi.org/10.3390/healthcare9121608