
Perceived Usefulness of Telerehabilitation of Musculoskeletal Disorders: A Belgium–France Pilot Study during Second Wave of COVID-19 Pandemic

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
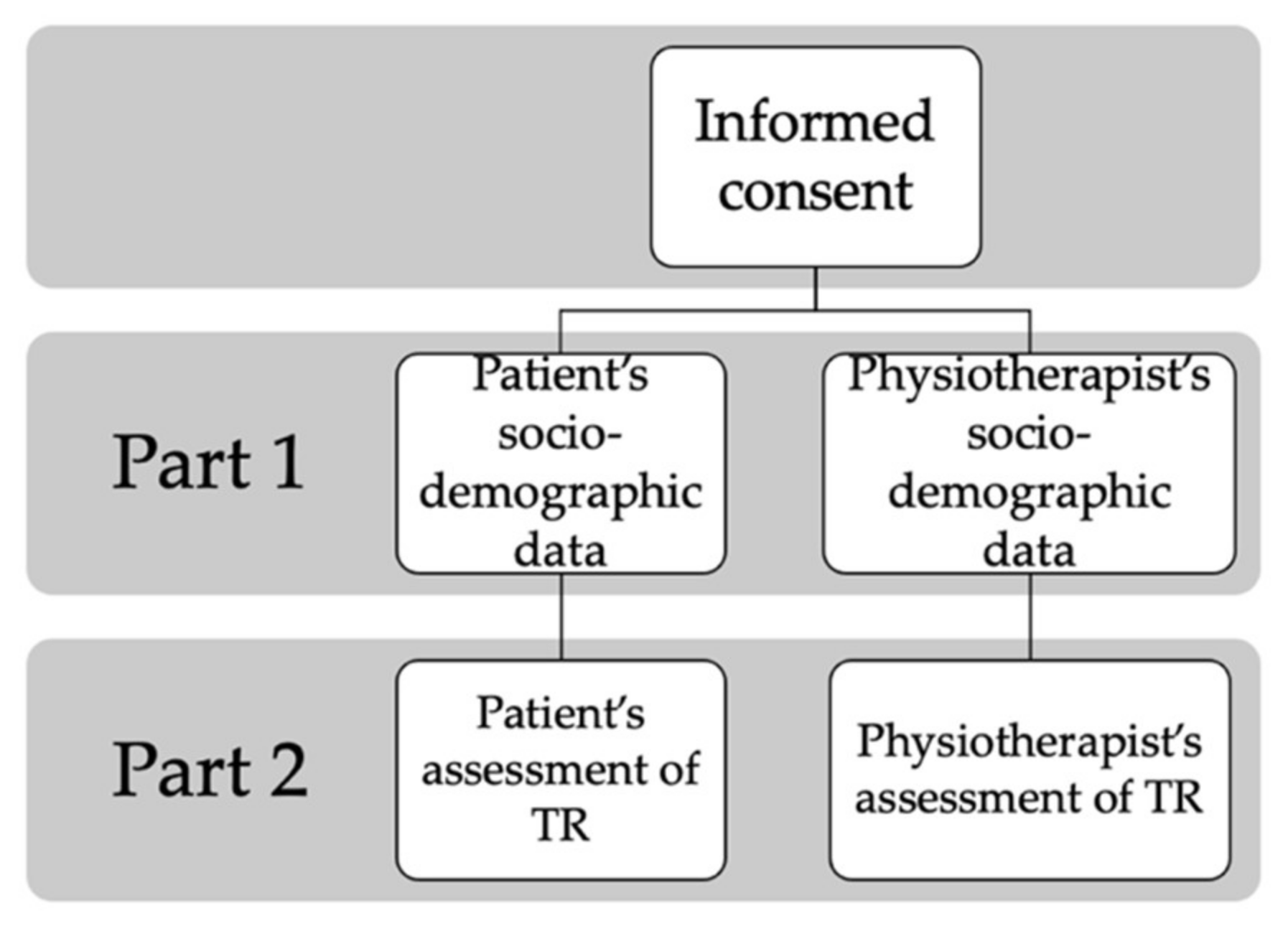
2.1. Questionnaire
- Whether the participant had previously used TR for the management of MSDs and/or other disorders;
- For what reasons it was used: sanitary measures, lack of transport, inability to reach the site or other;
- The modalities used, i.e., phone, smartphone, computer, tablet, or other.
2.2. Population
2.3. Data Analysis
3. Results
3.1. Participants’ Sociodemographic Data
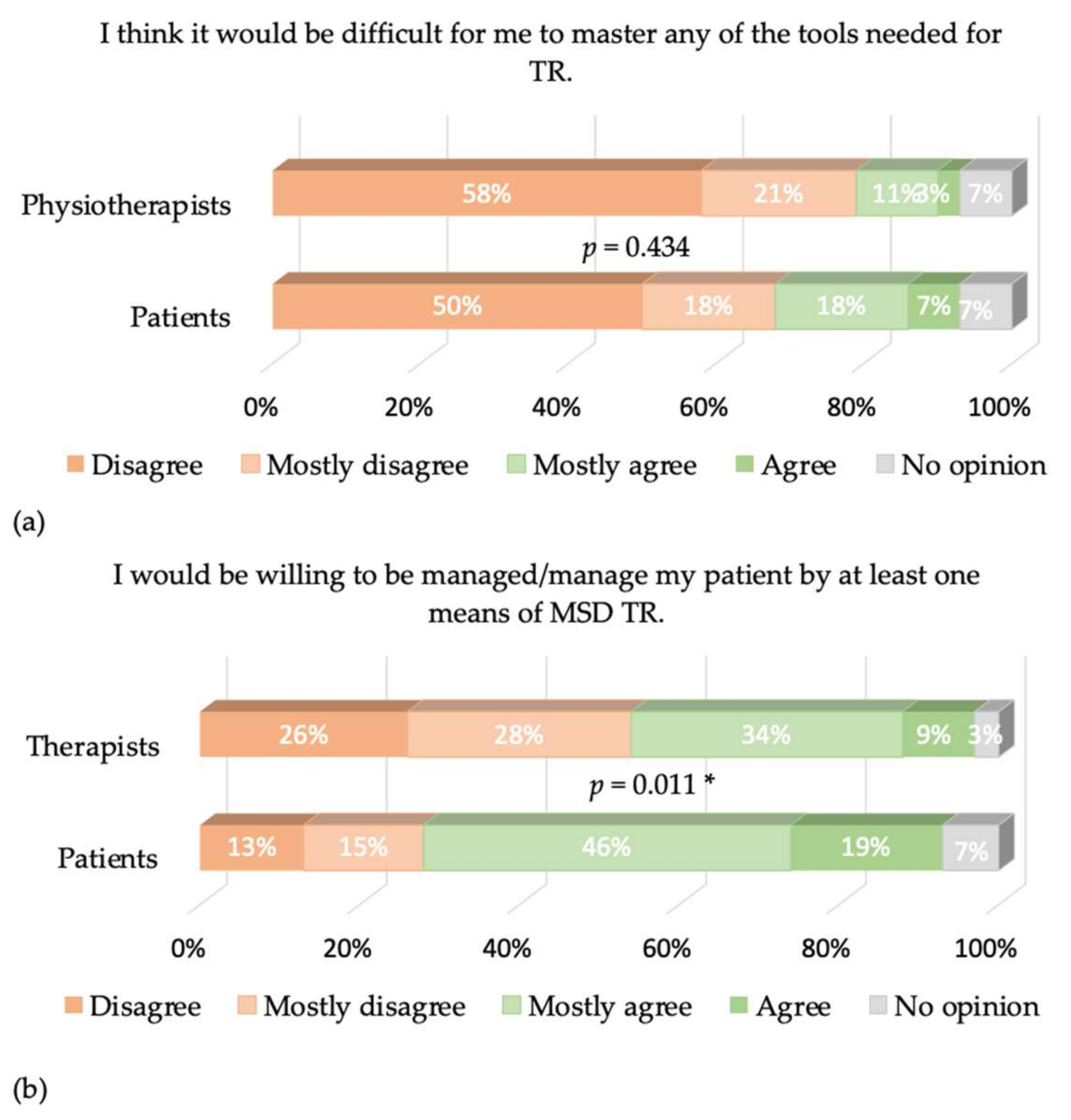
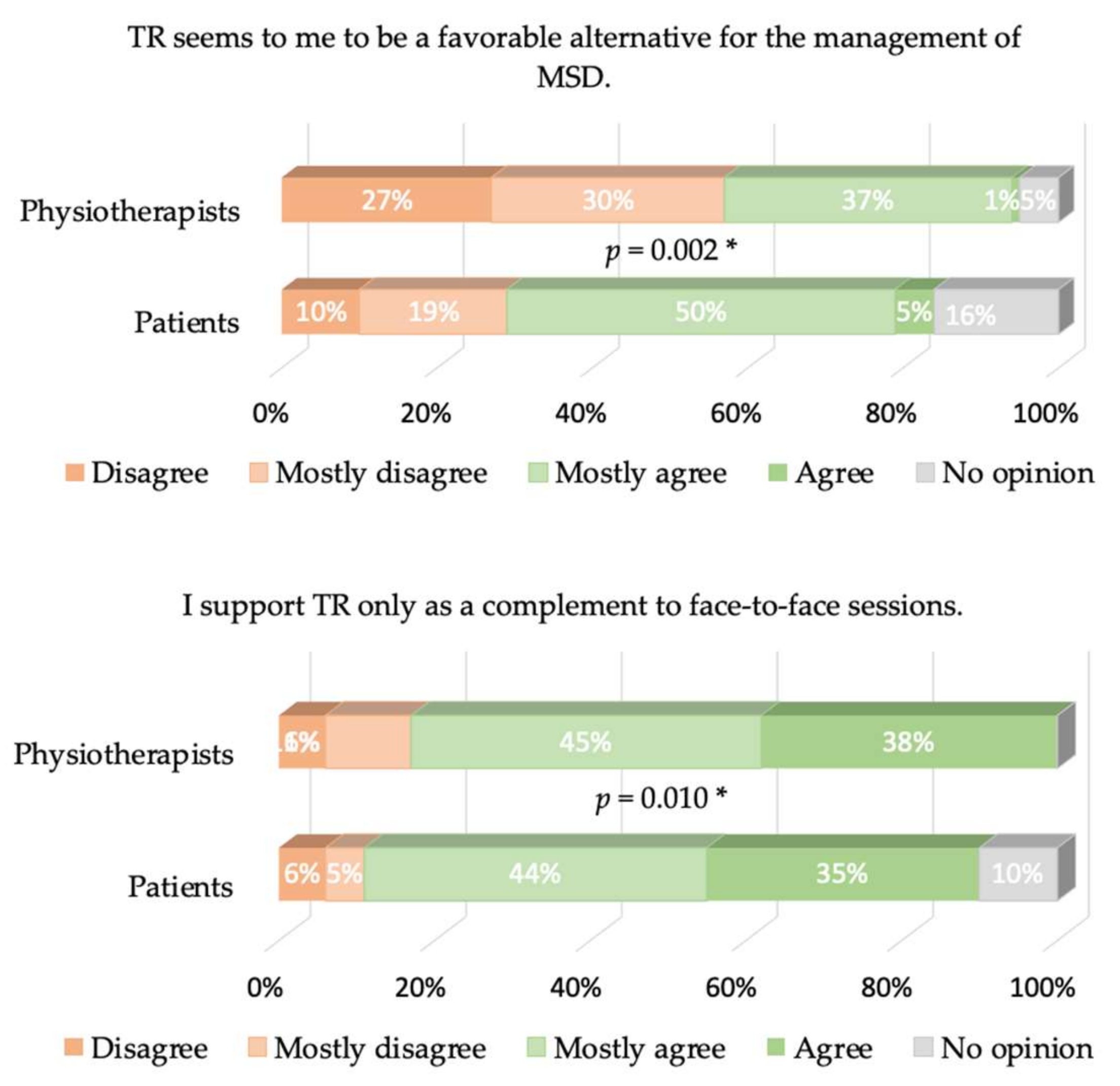
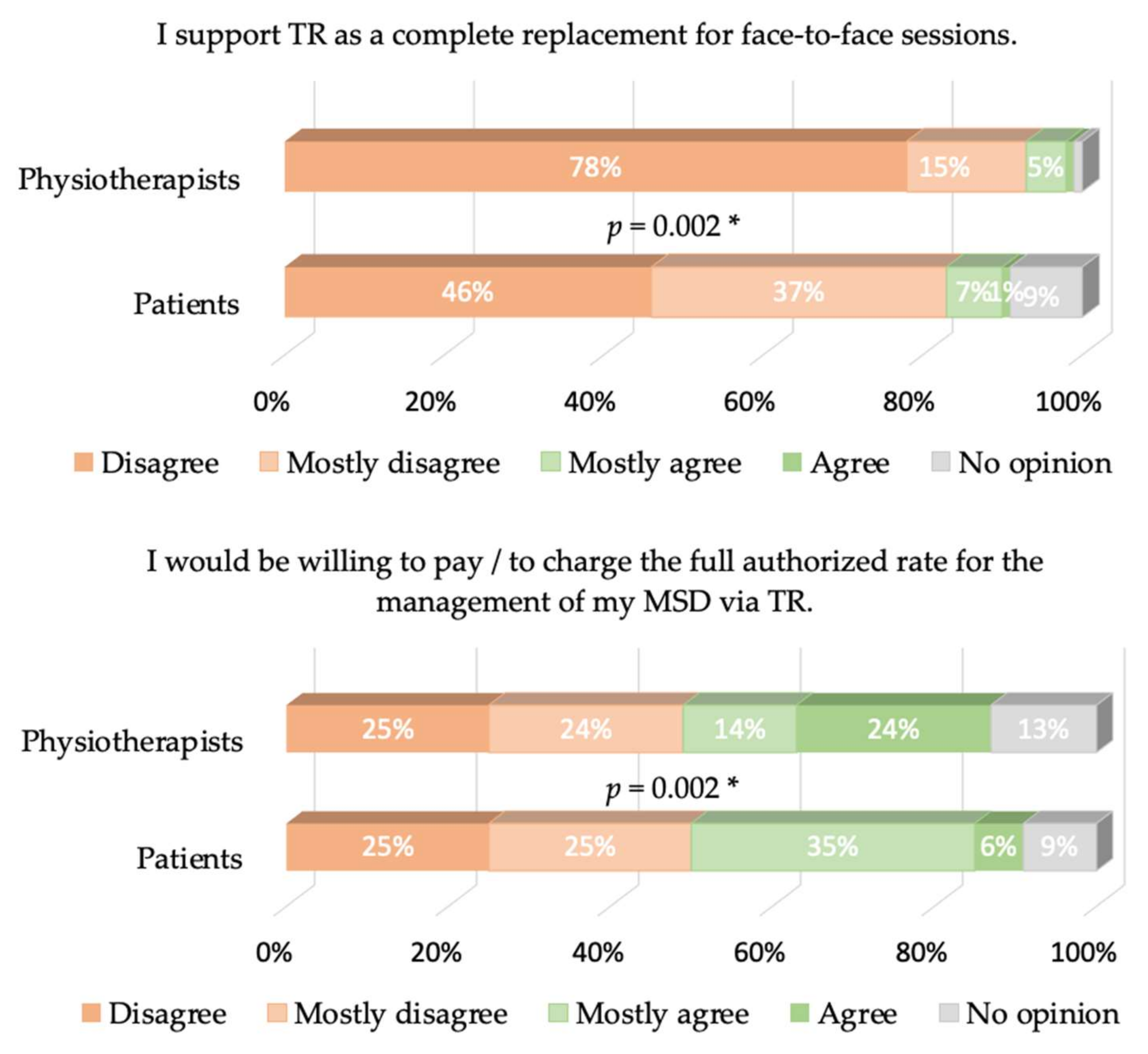
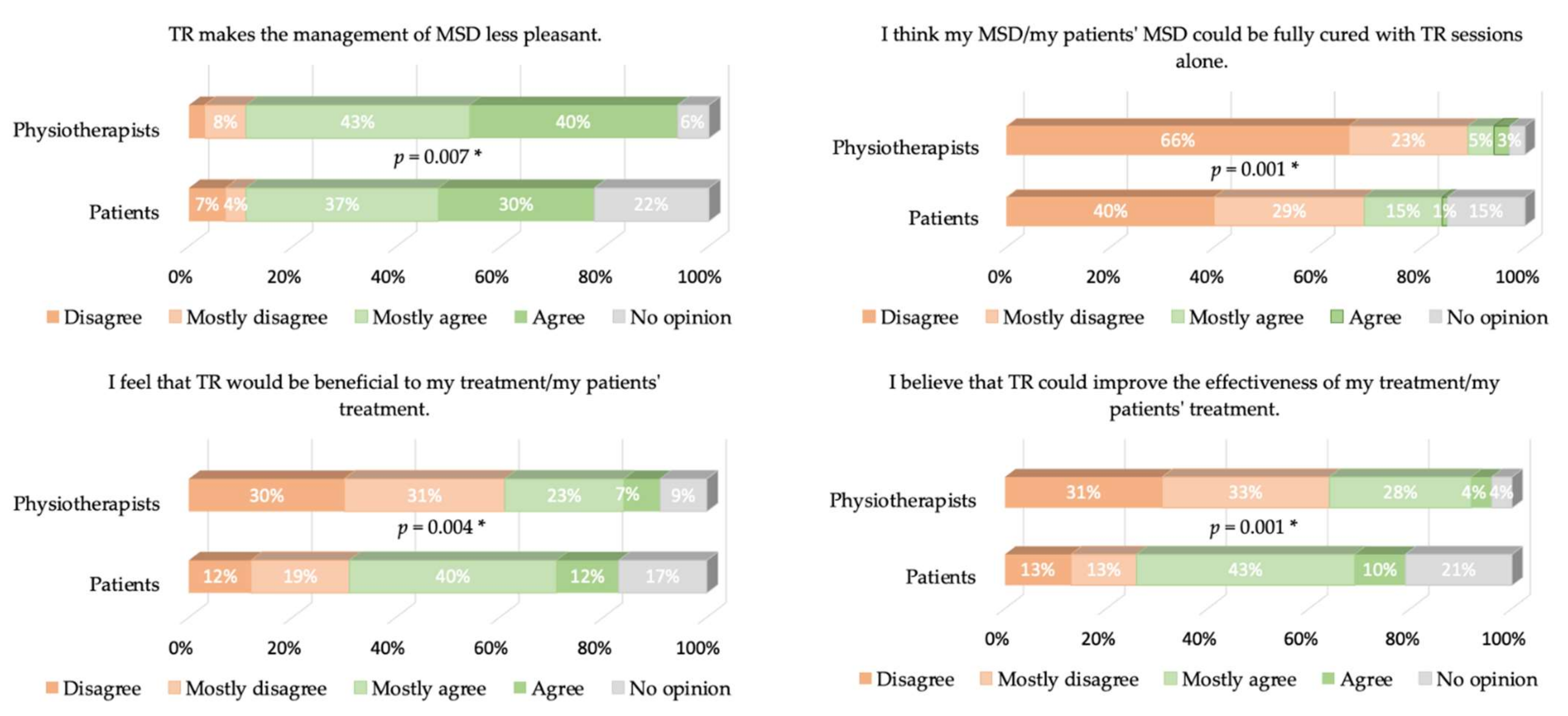
3.2. Patients vs. Physiotherapists
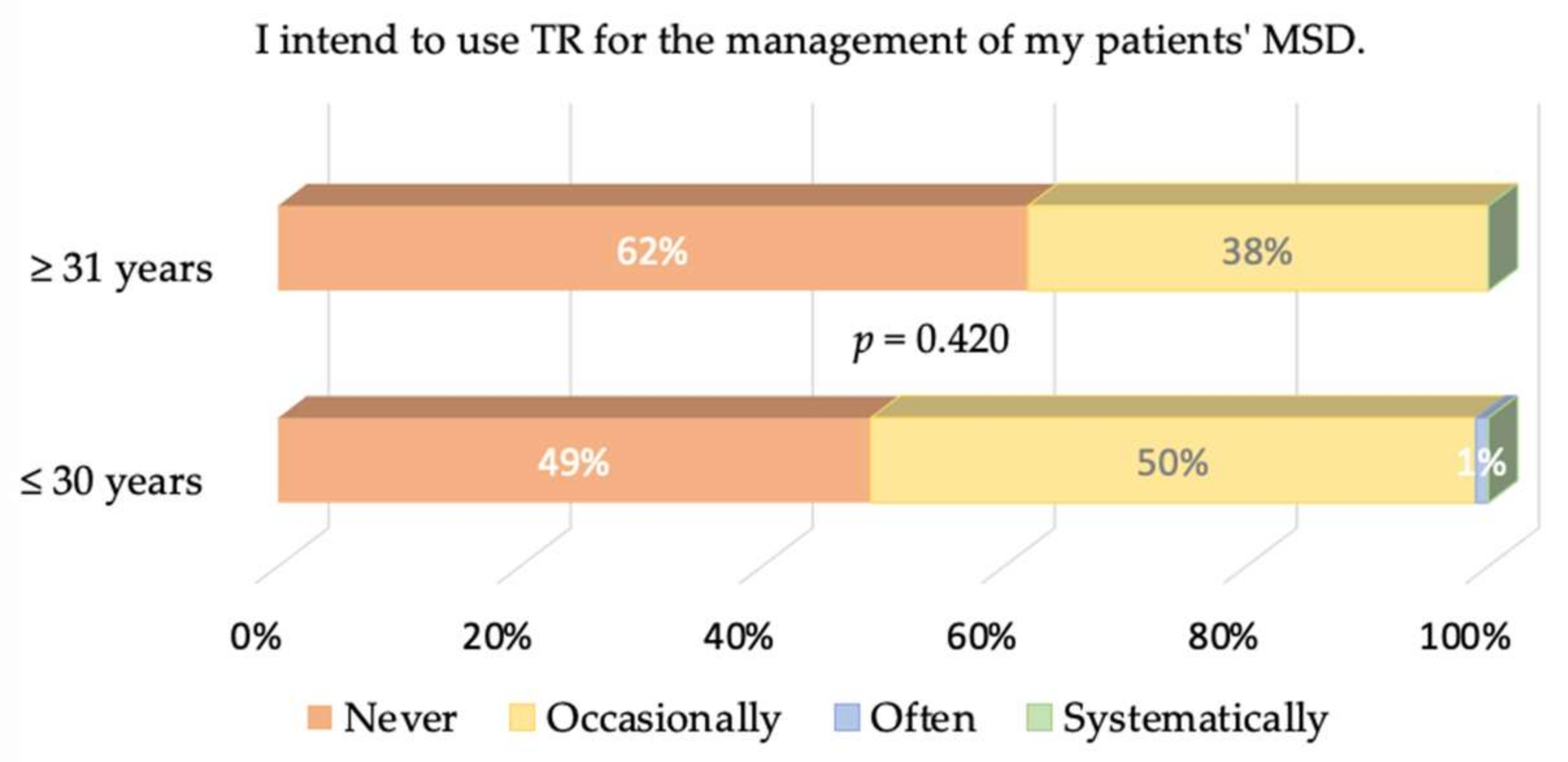
3.3. Young vs. Old Physiotherapists
4. Discussion
5. Concluding Comments
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. List of Items

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| TAM3 | Item |
|---|---|
| Perceived ease-of-use | I think it would be difficult for me to master any of the tools needed for TR. |
| Image | I would be willing to be managed/manage my patient by at least one means of MSD TR. |
| Job relevance | TR seems to me to be a favorable alternative for the management of MSD. |
| I support TR only as a complement to face-to-face sessions. | |
| Output quality | I support TR as a complete replacement for face-to-face sessions. |
| I would be willing to pay/to charge the full authorized rate for the management of my MSD via TR. | |
| Result demonstrability | TR makes the management of MSD less pleasant. |
| I think my MSD/my patient’s MSD could be fully cured with TR sessions alone. | |
| I feel that TR would be beneficial to my treatment/my patient’s treatment. | |
| I believe that TR could improve the effectiveness of my treatment/my patient’s treatment. | |
| Behavioral intention | I intend to use TR for the management of my MSD/my patient’s MSD. |
References
- Cieza, A.; Causey, K.; Kamenov, K.; Hanson, S.W.; Chatterji, S.; Vos, T. Global estimates of the need for rehabilitation based on the Global Burden of Disease study 2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 2006–2017. [Google Scholar] [CrossRef]
- Werneke, M.W.; Deutscher, D.; Grigsby, D.; Tucker, C.A.; Mioduski, J.E.; Hayes, D. Telerehabilitation During the COVID-19 Pandemic in Outpatient Rehabilitation Settings: A Descriptive Study. Phys. Ther. 2021, 101, pzab110. [Google Scholar] [CrossRef]
- Rosen, M.J. Telerehabilitation. Telemed. J. e-Health 2004, 10, 115–117. [Google Scholar] [CrossRef]
- Turolla, A.; Rossettini, G.; Viceconti, A.; Palese, A.; Geri, T. Musculoskeletal Physical Therapy During the COVID-19 Pandemic: Is Telerehabilitation the Answer? Phys. Ther. 2020, 100, 1260–1264. [Google Scholar] [CrossRef] [PubMed]
- Cottrell, M.A.; Galea, O.A.; O’Leary, S.P.; Hill, A.J.; Russell, T.G. Real-time telerehabilitation for the treatment of musculoskeletal conditions is effective and comparable to standard practice: A systematic review and meta-analysis. Clin. Rehabil. 2017, 31, 625–638. [Google Scholar] [CrossRef] [PubMed]
- Les TIC en Chiffres. Available online: https://economie.fgov.be/fr/themes/line/les-tic-en-belgique/les-tic-en-chiffres#:~:text=M%C3%A9nages%20et%20individus%20(2019),pourcentage%20par%20rapport%20%C3%A0%202018 (accessed on 11 May 2021).
- Ménages Français: Accès Internet 2006–2018. Available online: https://fr.statista.com/statistiques/509227/menage-francais-acces-internet/ (accessed on 11 May 2021).
- Statistiques sur L’économie et la Société Numériques—Ménages et particuliers—Statistics Explained. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Digital_economy_and_society_statistics_-_households_and_individuals/fr&oldid=509809 (accessed on 11 May 2021).
- Mani, S.; Sharma, S.; Omar, B.; Paungmali, A.; Joseph, L. Validity and reliability of Internet-based physiotherapy assessment for musculoskeletal disorders: A systematic review. J. Telemed. Telecare 2017, 23, 379–391. [Google Scholar] [CrossRef] [PubMed]
- Bini, S.A.; Mahajan, J. Clinical outcomes of remote asynchronous telerehabilitation are equivalent to traditional therapy following total knee arthroplasty: A randomized control study. J. Telemed. Telecare 2017, 23, 239–247. [Google Scholar] [CrossRef]
- Azma, K.; Rezasoltani, Z.; Rezaeimoghaddam, F.; Dadarkhah, A.; Mohsenolhosseini, S. Efficacy of tele-rehabilitation compared with office-based physical therapy in patients with knee osteoarthritis: A randomized clinical trial. J. Telemed. Telecare 2018, 24, 560–565. [Google Scholar] [CrossRef]
- Van Tilburg, M.L.; Kloek, C.J.J.; Staal, J.B.; Bossen, D.; Veenhof, C. Feasibility of a stratified blended physiotherapy intervention for patients with non-specific low back pain: A mixed methods study. Available online: https://pubmed.ncbi.nlm.nih.gov/32431201/ (accessed on 20 May 2020). [CrossRef]
- Fishbein, M.; Ajzen, I. Attitudes towards objects as predictors of single and multiple behavioral criteria. Psychol. Rev. 1974, 81, 59–74. [Google Scholar] [CrossRef]
- Kamal, S.A.; Shafiq, M.; Kakria, P. Investigating acceptance of telemedicine services through an extended technology acceptance model (TAM). Technol. Soc. 2020, 60, 101212. [Google Scholar] [CrossRef]
- Venkatesh, V.; Davis, F.D. A Theoretical Extension of the Technology Acceptance Model: Four Longitudinal Field Studies. Manag. Sci. 2000, 46, 186–204. [Google Scholar] [CrossRef] [Green Version]
- Venkatesh, V.; Bala, H. Technology Acceptance Model 3 and a Research Agenda on Interventions. Decis. Sci. 2008, 39, 273–315. [Google Scholar] [CrossRef] [Green Version]
- Venkatesh, V. Determinants of Perceived Ease of Use: Integrating Control, Intrinsic Motivation, and Emotion into the Technology Acceptance Model. Inf. Syst. Res. 2000, 11, 342–365. [Google Scholar] [CrossRef] [Green Version]
- Pilotti, A. Étude de la professionnalisation des masseurs-kinésithérapeutes salariés à partir de leurs usages des courriers électroniques. Available online: https://journals.openedition.org/edso/15385 (accessed on 1 May 2021).
- Vonstad, E.; Rennie, L.; Opheim, A. Factors Influencing Physiotherapist’s Intention to Use a Novel Physical Exercise Communication System in NeuroRehabilitation. In Proceedings of the International Congress on Neurotechnology, Electronics and Informatics, Porto, Portugal, 7–8 November 2016; pp. 3–5. [Google Scholar]
- Blumenthal, J.; Wilkinson, A.; Chignell, M. Physiotherapists’ and Physiotherapy Students’ Perspectives on the Use of Mobile or Wearable Technology in Their Practice. Physiother. Can. 2018, 70, 251–261. [Google Scholar] [CrossRef]
- Cranen, K. Acceptance of Telerehabilitation in Chronic Pain: The Patients’ Perspective. Ph.D. Thesis, University of Twente, Enschede, The Netherlands, 2018. [Google Scholar]
- TMS: Définition et Impact. Available online: https://www.ameli.fr/entreprise/sante-travail/risques/troubles-musculosquelettiques-tms/tms-definition-impact (accessed on 11 May 2021).
- Rios, R.A.; Nogueira, T.; Coimbra, D.B.; Lopes, T.J.S.; Abraham, A.; de Mello, R.F. Country transition index based on hierarchical clustering to predict next COVID-19 waves. Sci. Rep. 2021, 11, 1–13. [Google Scholar] [CrossRef]
- Cottrell, M.A.; Russell, T.G. Telehealth for musculoskeletal physiotherapy. Musculoskelet. Sci. Pr. 2020, 48, 102193. [Google Scholar] [CrossRef]
- LaPointe, K. Narrating career, positioning identity: Career identity as a narrative practice. J. Vocat. Behav. 2010, 77, 1–9. [Google Scholar] [CrossRef]
- Roquet, P.; Gatto, F.; Vincent, S. L’identification et la Reconnaissance des Rôles et des Identités des Masseurs-Kinésithérapeutes (Research Report); Conservatoire National des Arts et Métiers (CNAM): Paris, France; Centre de Recherche sur la Formation (CRF): Paris, France, 2015; Available online: https://hal.archives-ouvertes.fr/hal-01291525 (accessed on 11 October 2021).
- Pilotti, A. L’écriture comme analyseur des implications professionnelles du praticien masseur-kinésithérapeute hospitalier. In Mémoire de Maîtrise en Sciences de L’éducation Inédit; Université de Paris VIII: Saint-Denis, France, 2002. [Google Scholar]
- Continuité des Soins de Kinésithérapie: Soins à Distance Pendant les Mesures Covid-19—INAMI. Available online: https://www.inami.fgov.be/fr/covid19/Pages/continuite-soins-kines-prestations-distance.aspx (accessed on 11 May 2021).
- Almojaibel, A.A.; Munk, N.; Goodfellow, L.T.; Fisher, T.F.; Miller, K.K.; Comer, A.R.; Bakas, T.; Justiss, M.D. Health Care Practitioners’ Determinants of Telerehabilitation Acceptance. Int. J. Telerehabilit. 2020, 12, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Cottrell, M.A.; O’Leary, S.P.; Raymer, M.; Hill, A.J.; Comans, T.; Russell, T.G. Does telerehabilitation result in inferior clinical outcomes compared with in-person care for the management of chronic musculoskeletal spinal conditions in the tertiary hospital setting? A non-randomised pilot clinical trial. J. Telemed. Telecare 2019, 27, 444–452. [Google Scholar] [CrossRef] [PubMed]
- Richardson, B.R.; Truter, P.; Blumke, R.; Russell, T.G. Physiotherapy assessment and diagnosis of musculoskeletal disorders of the knee via telerehabilitation. J. Telemed. Telecare 2016, 23, 88–95. [Google Scholar] [CrossRef]
- Hinman, R.S.; Kimp, A.J.; Campbell, P.K.; Russell, T.; Foster, N.E.; Kasza, J.; Harris, A.; Bennell, K.L. Technology versus tradition: A non-inferiority trial comparing video to face-to-face consultations with a physiotherapist for people with knee osteoarthritis. Protocol for the PEAK randomised controlled trial. BMC Musculoskelet. Disord. 2020, 21, 522. [Google Scholar] [CrossRef] [PubMed]
- Slater, H.; Dear, B.F.; Merolli, M.; Li, L.C.; Briggs, A.M. Use of eHealth technologies to enable the implementation of musculoskeletal Models of Care: Evidence and practice. Best Pr. Res. Clin. Rheumatol. 2016, 30, 483–502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandes, L.G.; Devan, H.; Kamper, S.J.; Williams, C.; Saragiotto, B.T. Enablers and barriers of people with chronic musculoskeletal pain for engaging in telehealth interventions: Protocol for a qualitative systematic review and meta-synthesis. Syst. Rev. 2020, 9, 122. [Google Scholar] [CrossRef] [PubMed]
- Fiani, B.; Siddiqi, I.; Lee, S.C.; Dhillon, L. Telerehabilitation: Development, Application, and Need for Increased Usage in the COVID-19 Era for Patients with Spinal Pathology. Cureus 2020, 12, 10563. [Google Scholar] [CrossRef]
- De la Cal, J.M.; Fernández-Sánchez, M.; Matarán-Peñarrocha, G.A.; Hurley, D.A.; Castro-Sánchez, A.M.; Lara-Palomo, I.C. Physical Therapists’ Opinion of E-Health Treatment of Chronic Low Back Pain. Int. J. Environ. Res. Public Health 2021, 18, 1889. [Google Scholar] [CrossRef] [PubMed]
- Bigot, L.; Langeard, A.; Moussay, S.; Gautier, A.; Quarck, G. Activité physique à domicile pour les seniors: Revue de la question et proposition d’une pratique optimisée. Mov. Sport Sci. 2019, 103, 27–37. [Google Scholar] [CrossRef] [Green Version]







| Parameter | Patients | Physiotherapists | p |
|---|---|---|---|
| n | 68 | 107 | |
| Age (years) | 46.6 ± 14.1 | 31.6 ± 10.0 | ≤0.001 * |
| Live or work in (Belgium–France) | 56%–44% | 78%–22% | 0.004 * |
| Adequate Internet connection quality (Yes/No) | 89%–11% | 94%–6% | 0.260 |
| Adequate ease in using the Internet (Yes/No) | 98%–2% | 98%–2% | 0.690 |
| Previous use of TR (Yes/No) | 88%–12% | 76%–24% | 0.065 |
| Number of managed MSD patients per week | 15 [10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dierick, F.; Pierre, A.; Profeta, L.; Telliez, F.; Buisseret, F. Perceived Usefulness of Telerehabilitation of Musculoskeletal Disorders: A Belgium–France Pilot Study during Second Wave of COVID-19 Pandemic. Healthcare 2021, 9, 1605. https://doi.org/10.3390/healthcare9111605
Dierick F, Pierre A, Profeta L, Telliez F, Buisseret F. Perceived Usefulness of Telerehabilitation of Musculoskeletal Disorders: A Belgium–France Pilot Study during Second Wave of COVID-19 Pandemic. Healthcare. 2021; 9(11):1605. https://doi.org/10.3390/healthcare9111605
Chicago/Turabian StyleDierick, Frédéric, Amélie Pierre, Loredana Profeta, Frédéric Telliez, and Fabien Buisseret. 2021. "Perceived Usefulness of Telerehabilitation of Musculoskeletal Disorders: A Belgium–France Pilot Study during Second Wave of COVID-19 Pandemic" Healthcare 9, no. 11: 1605. https://doi.org/10.3390/healthcare9111605