
Agreement between 3D Motion Analysis and Tele-Assessment Using a Video Conferencing Application for Telerehabilitation

Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Sample Size Calculation
2.3. Experimental Exercise Procedures
2.4. Tele-Assessment Using Video Conference Application
2.5. Three-Dimensional Motion Analysis
2.6. Exercise Components Analysis
2.7. Statistical Analysis
3. Results
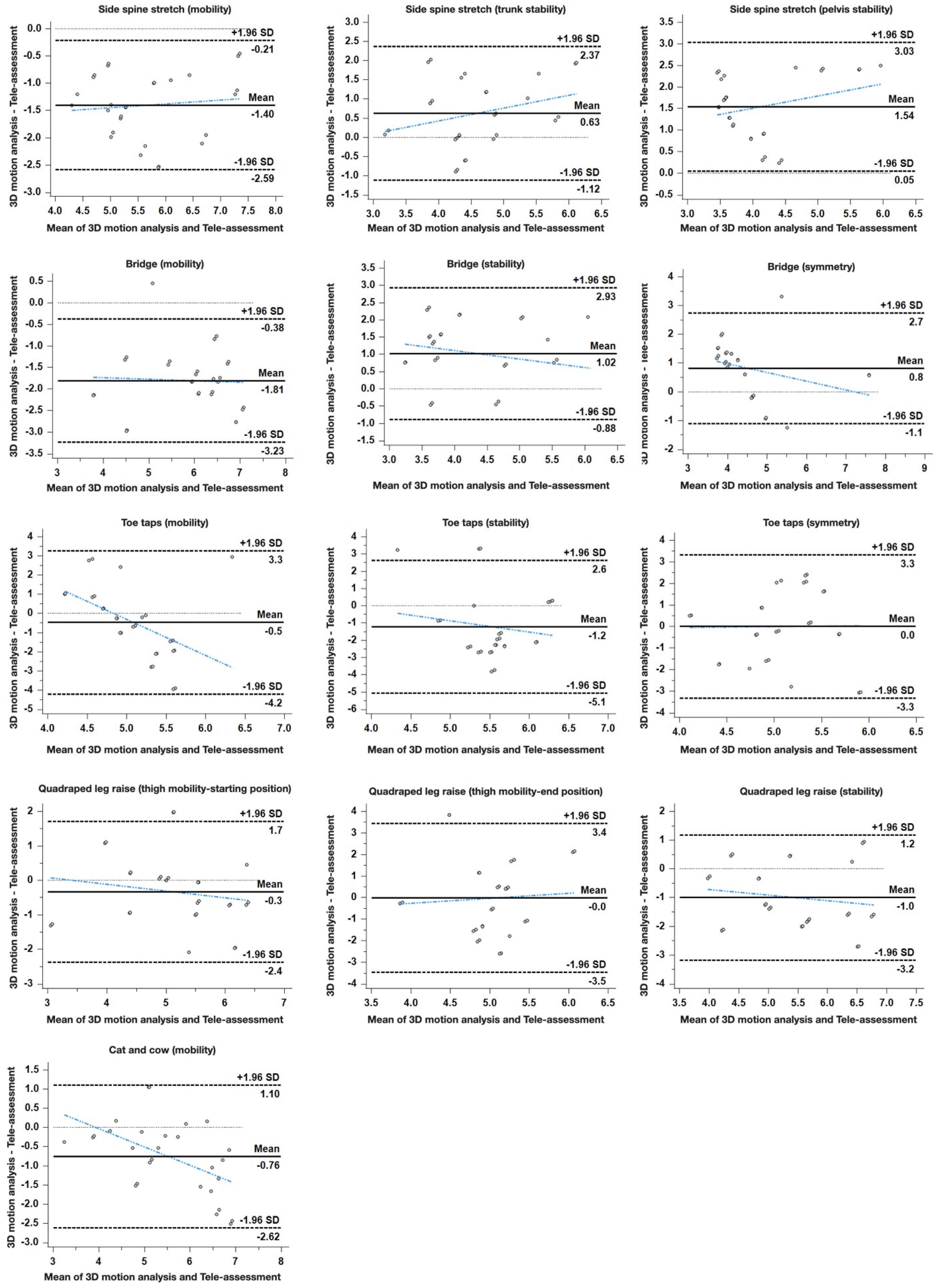
3.1. Concurrent Validity of the Kinematic Parameters for Subjects Using the 3D Motion Analysis System and Tele-Assessment Using a Video Conference Application
3.2. Inter-Rater Reliability of the Raters in Tele-Assessment Using Video Conference Application
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fiani, B.; Siddiqi, I.; Lee, S.C.; Dhillon, L. Telerehabilitation: Development, application, and need for increased usage in the COVID-19 era for patients with spinal pathology. Cureus 2020, 12, e10563. [Google Scholar] [CrossRef]
- Turolla, A.; Rossettini, G.; Viceconti, A.; Palese, A.; Geri, T. Musculoskeletal physical therapy during the COVID-19 pandemic: Is telerehabilitation the answer? Phys. Ther. 2020, 100, 1260–1264. [Google Scholar] [CrossRef]
- Mani, S.; Sharma, S.; Omar, B.; Paungmali, A.; Joseph, L. Validity and reliability of internet-based physiotherapy assessment for musculoskeletal disorders: A systematic review. J. Telemed. Telecare. 2017, 23, 379–391. [Google Scholar] [CrossRef]
- Russell, T.G.; Blumke, R.; Richardson, B.; Truter, P. Telerehabilitation mediated physiotherapy assessment of ankle disorders. Physiother Res. Int. 2010, 15, 167–175. [Google Scholar] [CrossRef]
- Seelman, K.D.; Hartman, L.M. Telerehabilitation: Policy issues and research tools. Int. J. Telerehabil. 2009, 1, 47–58. [Google Scholar] [CrossRef] [Green Version]
- Theodoros, D.; Russell, T. Telerehabilitation: Current perspectives. Stud. Health Technol. Inform. 2008, 131, 191–209. [Google Scholar]
- Galea, M.D. Telemedicine in rehabilitation. Phys. Med. Rehabil. Clin. N. Am. 2019, 30, 473–483. [Google Scholar] [CrossRef]
- Howard, I.M.; Kaufman, M.S. Telehealth applications for outpatients with neuromuscular or musculoskeletal disorders. Muscle Nerve 2018, 58, 475–485. [Google Scholar] [CrossRef]
- Tenforde, A.S.; Hefner, J.E.; Kodish-Wachs, J.E.; Iaccarino, M.A.; Paganoni, S. Telehealth in physical medicine and rehabilitation: A narrative review. PM&R 2017, 9, S51–S58. [Google Scholar]
- Venkataraman, K.; Amis, K.; Landerman, L.R.; Caves, K.; Koh, G.C.; Hoenig, H. Teleassessment of gait and gait aids: Validity and interrater reliability. Phys. Ther. 2020, 100, 708–717. [Google Scholar] [CrossRef]
- Hoenig, H.; Tate, L.; Dumbleton, S.; Montgomery, C.; Morgan, M.; Landerman, L.R.; Caves, K. A quality assurance study on the accuracy of measuring physical function under current conditions for use of clinical video telehealth. Arch. Phys. Med. Rehabil. 2013, 94, 998–1002. [Google Scholar] [CrossRef]
- Walter, S.D.; Eliasziw, M.; Donner, A. Sample size and optimal designs for reliability studies. Stat. Med. 1998, 17, 101–110. [Google Scholar] [CrossRef]
- Lai, B.; Chiu, C.Y.; Pounds, E.; Tracy, T.; Mehta, T.; Young, H.J.; Riser, E.; Rimmer, J. COVID-19 modifications for remote teleassessment and teletraining of a complementary alternative medicine intervention for people with multiple sclerosis: Protocol for a randomized controlled trial. JMIR Res. Protoc. 2020, 9, e18415. [Google Scholar] [CrossRef]
- Cook, R. Introducing: Telehealth and telecare. Br. J. Community Nurs. 2007, 12, 307. [Google Scholar] [CrossRef]
- Stowe, S.; Harding, S. Telecare, telehealth and telemedicine. European Geriatr. Med. 2010, 1, 193–197. [Google Scholar] [CrossRef]
- Cabrera-Martos, I.; Ortiz-Rubio, A.; Torres-Sanchez, I.; Lopez-Lopez, L.; Rodriguez-Torres, J.; Carmen Valenza, M. Agreement between face-to-face and tele-assessment of upper limb functioning in patients with parkinson disease. PM&R 2019, 11, 590–596. [Google Scholar]
- Yozbatiran, N.; Harness, E.T.; Le, V.; Luu, D.; Lopes, C.V.; Cramer, S.C. A tele-assessment system for monitoring treatment effects in subjects with spinal cord injury. J. Telemed. Telecare. 2010, 16, 152–157. [Google Scholar] [CrossRef]
- Botsis, T.; Hartvigsen, G. Current status and future perspectives in telecare for elderly people suffering from chronic diseases. J. Telemed. Telecare. 2008, 14, 195–203. [Google Scholar] [CrossRef]
- Piron, L.; Turolla, A.; Agostini, M.; Zucconi, C.; Cortese, F.; Zampolini, M.; Zannini, M.; Dam, M.; Ventura, L.; Battauz, M.; et al. Exercises for paretic upper limb after stroke: A combined virtual-reality and telemedicine approach. J. Rehabil. Med. 2009, 41, 1016–1102. [Google Scholar] [CrossRef] [Green Version]
- Burdea, G.; Popescu, V.; Hentz, V.; Colbert, K. Virtual reality-based orthopedic telerehabilitation. IEEE Trans. Rehabil. Eng. 2000, 8, 430–432. [Google Scholar] [CrossRef] [Green Version]
- Giallauria, F.; Lucci, R.; Pilerci, F.; De Lorenzo, A.; Manakos, A.; Psaroudaki, M.; Dagostino, M.; Vitelli, A.; Maresca, L.; Del Forno, D.; et al. Efficacy of telecardiology in improving the results of cardiac rehabilitation after acute myocardial infarction. Monaldi. Arch. Chest. Dis. 2006, 66, 8–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giladi, N. Mobility and exercise in movement disorders. Parkinsonism Relat. Disord. 2009, 15 (Suppl. 3), S46–S48. [Google Scholar] [CrossRef]
- Okada, T.; Huxel, K.C.; Nesser, T.W. Relationship between core stability, functional movement, and performance. J. Strength Cond. Res. 2011, 25, 252–261. [Google Scholar] [CrossRef] [PubMed]
- Lomaglio, M.J.; Eng, J.J. Muscle strength and weight-bearing symmetry relate to sit-to-stand performance in individuals with stroke. Gait Posture 2005, 22, 126–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lade, H.; McKenzie, S.; Steele, L.; Russell, T.G. Validity and reliability of the assessment and diagnosis of musculoskeletal elbow disorders using telerehabilitation. J. Telemed. Telecare. 2012, 18, 413–418. [Google Scholar] [CrossRef] [PubMed]
- Russell, T.G.; Jull, G.A.; Wootton, R. The diagnostic reliability of internet-based observational kinematic gait analysis. J. Telemed. Telecare. 2003, 9 (Suppl. 2), S48–S51. [Google Scholar] [CrossRef]
- Chanlalit, C.; Kongmalai, P. Validation of the telemedicine-based goniometry for measuring elbow range of motion. J. Med. Assoc. Thai. 2012, 95 (Suppl. 12), S113–S117. [Google Scholar]
- Russell, T.; Truter, P.; Blumke, R.; Richardson, B. The diagnostic accuracy of telerehabilitation for nonarticular lower-limb musculoskeletal disorders. Telemed. J. E. Health 2010, 16, 585–594. [Google Scholar] [CrossRef]
- Chan, H.; Zheng, H.; Wang, H.; Newell, D. Assessment of gait patterns of chronic low back pain patients: A smart mobile phone based approach. 2015 IEEE. BIBM 2015, 1016–1023. [Google Scholar]
- Truter, P.; Russell, T.; Fary, R. The validity of physical therapy assessment of low back pain via telerehabilitation in a clinical setting. Telemed. J. E. Health 2014, 20, 161–167. [Google Scholar] [CrossRef]
- Steele, L.; Lade, H.; McKenzie, S.; Russell, T.G. Assessment and diagnosis of musculoskeletal shoulder disorders over the internet. Int. J. Telemed. Appl. 2012, 2012, 945745. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Exercises | Components | 3D Motion Analysis | Tele-Assessment Using Video Conferencing Application |
|---|---|---|---|
| Side spine stretch | Mobility (angle) | Angle of trunk motion | Was there a fine movement of the trunk? |
| Trunk stability (angle) | Angle of forward and backward motion of trunk | Was there a forward and backward movement of the trunk? | |
| Pelvis stability (angle) | Angle of left-and-right motion of pelvis | Was there a left-and-right movement of the trunk? | |
| Symmetry (angle) | Angle difference of trunk motion between left and right | Was there a left-and-right symmetry in movement? | |
| Bridge | Mobility (angle) | Angle of trunk extension | Did legs and trunk move in a line? |
| Stability (mm) | Distance of leg sway | Were there any movements of the legs? | |
| Symmetry (angle) | Angle of left-and-right motion of pelvis | Was there a tilting of the pelvis to the sides? | |
| Toe taps | Mobility (angle) | Angle of knee joint motion | Was there a fine movement of the hip joint while controlling knee joint movement? (reverse coded) |
| Stability (angle) | Angle of the pelvis | Was there a sway of the pelvis? | |
| Symmetry (mm) | Distance between the knees | Was the distance between the knees constant? | |
| Quadruped leg raise | Thigh mobility—starting position (angle) | Angle of thigh | Was the femur aligned vertically after coming back to the starting position? |
| Thigh mobility—end position (angle) | Angle of thigh | Were the femur and lower leg parallel when they were lifted at the end position? | |
| Stability (mm) | Distance of femur sway | Was there any sway in the supporting leg? | |
| Symmetry (angle) | Angle difference of hip joints | Was there a left-and-right movement symmetry in the legs? | |
| Cat and cow | Mobility (angle) | Angle of pelvis motion | Was there a fine movement of the pelvis? |
| Hip joint stability (angle) | Angle of femur | Did the supporting leg maintain at 90°? (reverse coded) | |
| Leg stability (mm) | Distance of femur sway | Was there any sway in the supporting leg? |
| Exercise | Components | 3D Motion Analysis | Tele-Assessment | ICC (95% CI) | CV% | 95% LOA | ||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||||
| Side spine stretch | Mobility | 13.95 | 5.97 | 6.39 | 0.90 | 0.884 | 33.80 | 0.757~0.945 |
| Trunk stability | 5.15 | 1.60 | 4.32 | 0.75 | 0.668 | 24.82 | 0.303~0.842 | |
| Pelvis stability | 5.25 | 4.43 | 3.40 | 0.75 | 0.763 | 59.80 | 0.503~0.887 | |
| Symmetry | 1.02 | 0.50 | 6.61 | 0.52 | 0.396 | 13.28 | −0.267~0.712 | |
| Mobility | 171.80 | 6.06 | 6.72 | 1.09 | 0.820 | 4.01 | 0.622~0.914 | |
| Bridge | Stability | 156.97 | 58.14 | 3.92 | 1.12 | 0.753 | 36.83 | 0.481~0.882 |
| Symmetry | 1.10 | 1.25 | 4.17 | 1.25 | 0.667 | 47.35 | 0.301~0.841 | |
| Mobility | 26.44 | 12.46 | 5.26 | 1.26 | 0.573 | 43.26 | 0.252~0.761 | |
| Toe taps | Stability | 1.00 | 0.42 | 6.03 | 1.28 | 0.628 | 24.13 | 0.351~0.804 |
| Symmetry | 249.67 | 68.60 | 5.16 | 0.98 | 0.564 | 27.30 | 0.262~0.768 | |
| Thigh mobility—starting position | 70.41 | 7.99 | 5.37 | 1.12 | 0.668 | 12.03 | 0.303~0.842 | |
| Quadruped leg raise | Thigh mobility—end position | 7.16 | 5.62 | 5.07 | 0.97 | 0.544 | 53.86 | 0.234~0.753 |
| Stability | 9874.67 | 1702.60 | 5.98 | 1.11 | 0.611 | 17.24 | 0.183~0.815 | |
| Symmetry | 2.67 | 1.78 | 5.28 | 1.10 | −0.387 | 36.25 | −1.915~0.339 | |
| Mobility | 42.09 | 10.57 | 5.83 | 1.40 | 0.811 | 24.98 | 0.603~0.910 | |
| Cat and cow | Hip joint stability | 47.24 | 20.08 | 6.70 | 0.81 | −0.045 | 38.73 | −1.197~0.502 |
| Leg stability | 466.03 | 185.16 | 5.48 | 0.73 | 0.193 | 39.42 | −0.694~0.616 | |
| Exercise | Components | R1 | R2 | R3 | R4 | R5 | R6 | R7 | R8 | ICC (95% CI) | 95% LOA |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Side spine stretch | Mobility (angle) | 5.87 | 9.67 | 6.87 | 5.33 | 7.60 | 4.93 | 4.47 | 7.00 | 0.541 | 0.793~0.821 |
| Trunk stability (angle) | 2.60 | 1.47 | 4.53 | 5.27 | 5.60 | 5.20 | 5.60 | 5.27 | 0.181 | −0.302~0.622 | |
| Pelvis stability (angle) | 3.53 | 1.07 | 4.00 | 4.67 | 1.60 | 4.67 | 4.27 | 2.80 | 0.271 | −0.116~0.651 | |
| Symmetry (angle) | 6.27 | 9.13 | 6.80 | 4.67 | 6.73 | 6.13 | 6.53 | 7.33 | 0.145 | −0.292~0.554 | |
| Bridge | Mobility (angle) | 7.00 | 9.73 | 7.80 | 3.93 | 7.93 | 5.20 | 5.47 | 7.47 | 0.560 | 0.234~0.807 |
| Stability (mm) | 3.87 | 4.27 | 3.67 | 4.27 | 2.00 | 5.27 | 4.13 | 2.67 | 0.634 | 0.319~0.850 | |
| Symmetry (angle) | 4.20 | 2.60 | 5.73 | 4.53 | 2.60 | 4.73 | 4.80 | 2.93 | 0.551 | 0.179~0.814 | |
| Mobility (angle) | 5.80 | 9.20 | 3.87 | 3.27 | 5.47 | 5.20 | 4.00 | 6.80 | 0.583 | 0.261~0.820 | |
| Toe taps | Stability (angle) | 6.60 | 8.53 | 4.53 | 4.33 | 6.73 | 5.60 | 5.87 | 7.33 | 0.711 | 0.437~0.882 |
| Symmetry (mm) | 4.80 | 4.33 | 4.33 | 4.33 | 5.53 | 5.80 | 7.00 | 6.60 | 0.423 | −0.013~0.754 | |
| Thigh mobility—starting position (angle) | 5.00 | 5.67 | 4.87 | 4.13 | 6.53 | 5.73 | 5.67 | 6.47 | 0.639 | 0.314~0.854 | |
| Quadruped leg raise | Thigh mobility—end position (angle) | 5.53 | 4.40 | 5.13 | 4.40 | 5.80 | 4.60 | 5.60 | 6.27 | 0.478 | 0.009~0.789 |
| Stability (mm) | 6.80 | 6.00 | 6.00 | 6.80 | 6.73 | 5.60 | 3.93 | 6.07 | 0.537 | 0.143~0.810 | |
| Symmetry (angle) | 6.13 | 4.60 | 4.60 | 4.20 | 5.40 | 5.73 | 6.27 | 6.20 | 0.678 | 0.388~0.870 | |
| Mobility (angle) | 6.27 | 8.00 | 4.67 | 4.47 | 7.67 | 5.33 | 4.40 | 4.87 | 0.801 | 0.575~0.923 | |
| Cat and cow | Hip joint stability (angle) | 7.20 | 8.47 | 5.73 | 5.13 | 7.80 | 6.40 | 6.13 | 6.53 | 0.574 | 0.249~0.817 |
| Leg stability (mm) | 6.13 | 8.20 | 4.93 | 4.53 | 4.33 | 6.00 | 4.20 | 4.73 | 0.242 | −0.135~0.628 | |
| Total | 0.744 | 0.694~0.789 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, K. Agreement between 3D Motion Analysis and Tele-Assessment Using a Video Conferencing Application for Telerehabilitation. Healthcare 2021, 9, 1591. https://doi.org/10.3390/healthcare9111591
Lee K. Agreement between 3D Motion Analysis and Tele-Assessment Using a Video Conferencing Application for Telerehabilitation. Healthcare. 2021; 9(11):1591. https://doi.org/10.3390/healthcare9111591
Chicago/Turabian StyleLee, Kyeongjin. 2021. "Agreement between 3D Motion Analysis and Tele-Assessment Using a Video Conferencing Application for Telerehabilitation" Healthcare 9, no. 11: 1591. https://doi.org/10.3390/healthcare9111591