
Minimally Invasive Two-Staged Surgery in the Treatment of Large Cystic Lesions of the Jaw

 , and
, and {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
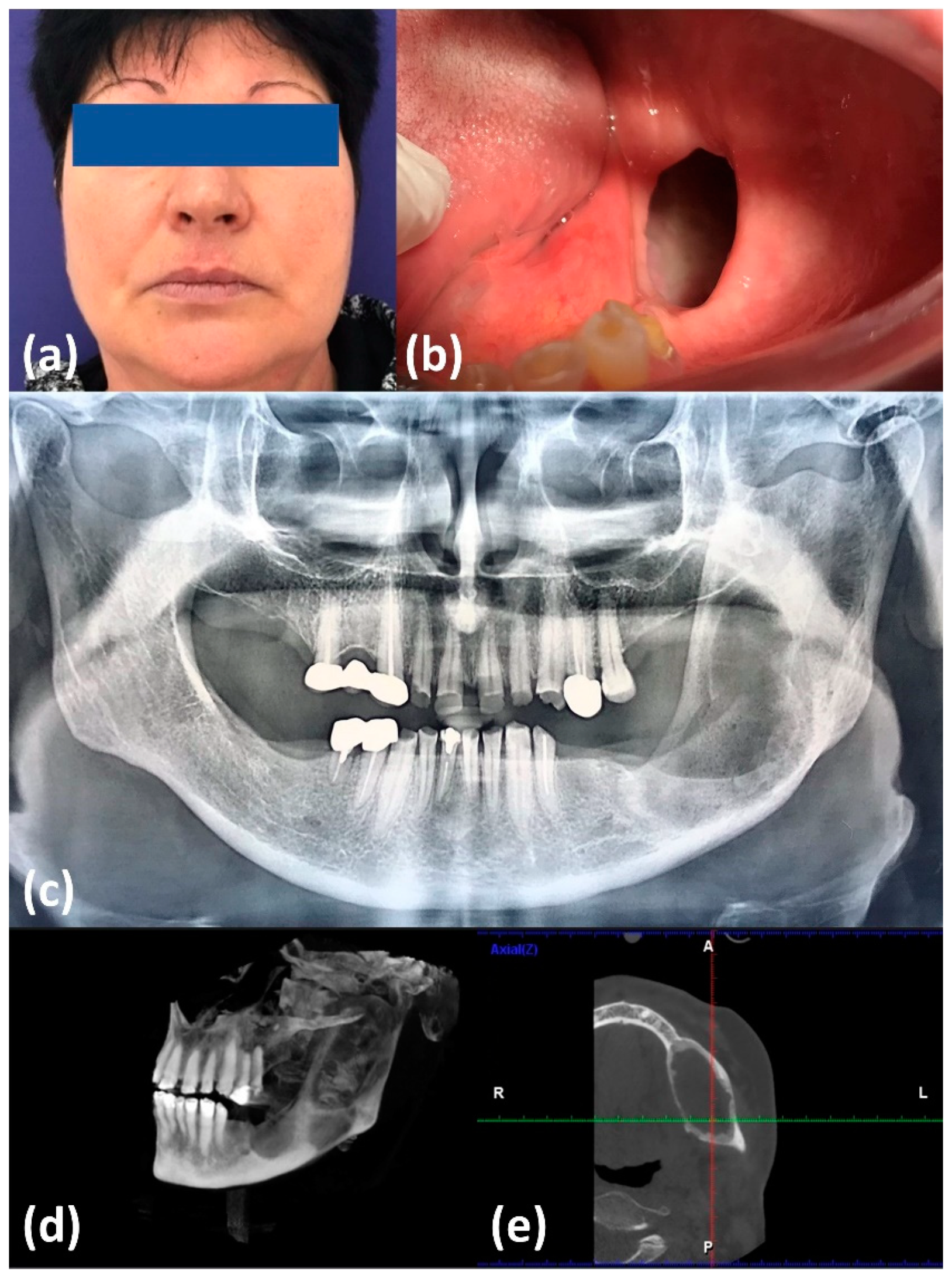
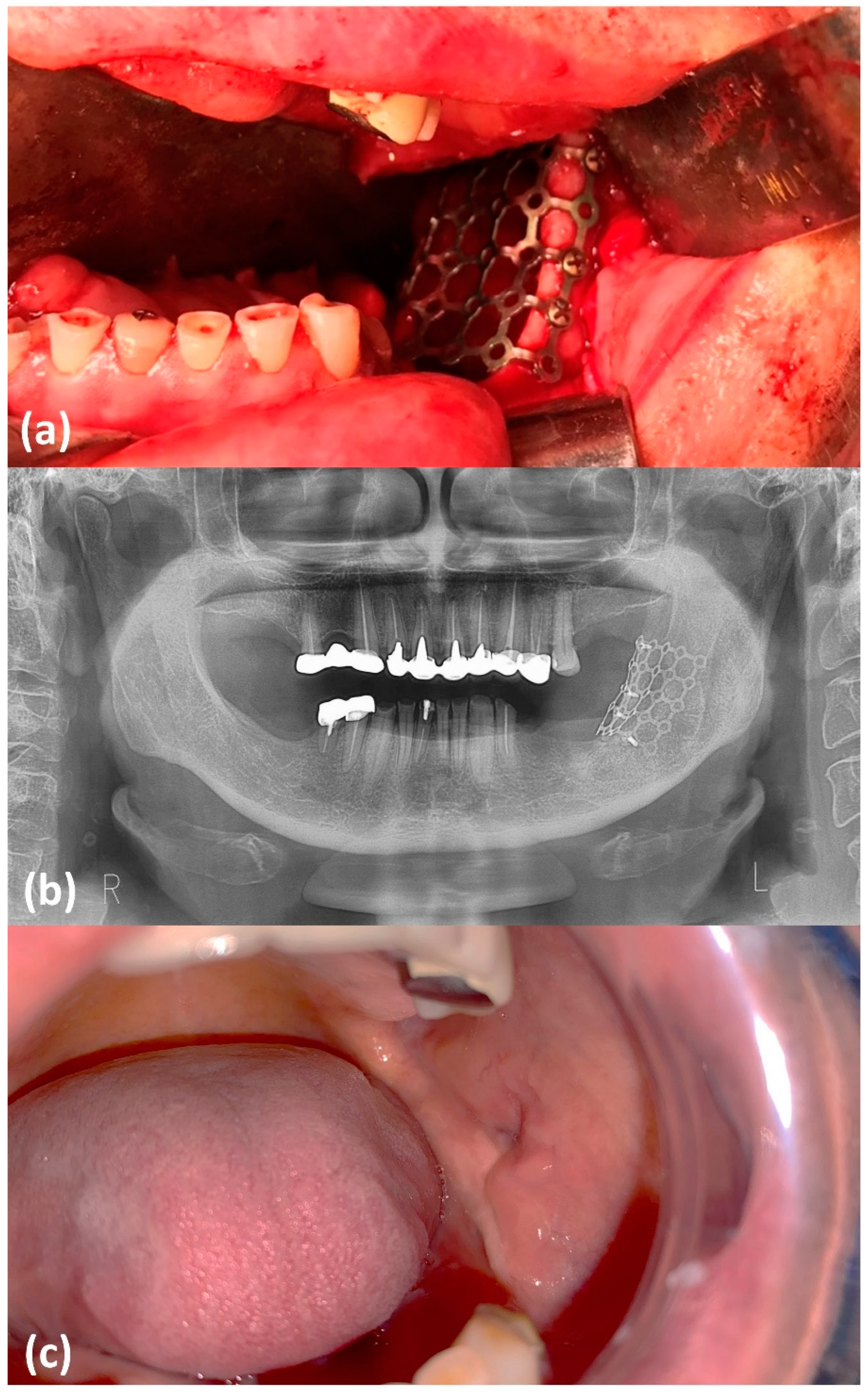
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Barresi, A.; Oteri, G.; Alibrandi, A.; Peditto, M.; Rapisarda, S.; Cardia, R.; Marcianò, A.; Lentini, M. A Comparative Statistical Analysis on the Incidence of Developmental, Inflammatory and Neoplastic Odontogenic Cysts—A Single Center Retrospective Analysis from Italy. Oral 2021, 1, 15–22. [Google Scholar] [CrossRef]
- Singh, J.; Singh, S.; Chandra, S.; Samadi., F.M. Prevalence and Distribution of Odontogenic Cysts and Tumors in North Indian Population: A Database Study with Systematic Review. Int. J. Appl. Biol. Pharm. Technol. 2020, 11, 46–59. [Google Scholar]
- Xiao, X.; Dai, J.-W.; Li, Z.; Zhang, W. Pathological Fracture of the Mandible Caused by Radicular Cyst: A Case Report and Literature Review. Medicine 2018, 97, e13529. [Google Scholar] [CrossRef] [PubMed]
- Boffano, P.; Roccia, F.; Gallesio, C.; Berrone, S. Pathological Mandibular Fractures: A Review of the Literature of the Last Two Decades. Dent. Traumatol. 2013, 29, 185–196. [Google Scholar] [CrossRef] [PubMed]
- Kubota, Y.; Yamashiro, T.; Oka, S.; Ninomiya, T.; Ogata, S.; Shirasuna, K. Relation between Size of Odontogenic Jaw Cysts and the Pressure of Fluid Within. Br. J. Oral Maxillofac. Surg. 2004, 42, 391–395. [Google Scholar] [CrossRef] [PubMed]
- Ward, J.P.; Magar, V.; Franks, S.J.; Landini, G. A Mathematical Model of the Dynamics of Odontogenic Cyst Growth. Anal. Quant. Cytol. Histol. 2004, 26, 39–46. [Google Scholar]
- Stokke, T. Osmotic Pressure in Odontogenic Cysts. Acta Odontol. Scand. 1956, 14, 65–78. [Google Scholar] [CrossRef]
- Singh, H.; Shetty, D.; Kumar, A.; Chavan, R.; Shori, D.; Mali, J. A Molecular Insight into the Role of Inflammation in the Behavior and Pathogenesis of Odontogenic Cysts. Ann. Med. Health Sci. Res. 2013, 3, 523–528. [Google Scholar] [CrossRef]
- Loxha, M.P.; Salihu, S.; Kryeziu, K.; Loxha, S.; Agani, Z.; Hamiti, V.; Rexhepi, A. Epidermoid Cyst of Mandible Ramus: Case Report. Med. Arch. 2016, 70, 238–240. [Google Scholar] [CrossRef] [Green Version]
- Sullivan, M.; Gallagher, G.; Noonan, V. The Root of the Problem: Occurrence of Typical and Atypical Periapical Pathoses. J. Am. Dent. Assoc. 2016, 147, 646–649. [Google Scholar] [CrossRef]
- Boos Lima, F.B.D.J.; Viana, A.P.C.; Lima, L.H.F.; Ribeiro, B.C.; Dutra, C.E.A.; Stabile, G.A.V.; Junior, S.M.L. A Rare Case of Gorlin-Goltz Syndrome in Children. Case Rep. Dent. 2019, 2019, 1608783. [Google Scholar] [CrossRef] [Green Version]
- Ritschl, L.M.; Mücke, T.; Hart, D.; Unterhuber, T.; Kehl, V.; Wolff, K.-D.; Fichter, A.M. Retrospective Analysis of Complications in 190 Mandibular Resections and Simultaneous Reconstructions with Free Fibula Flap, Iliac Crest Flap or Reconstruction Plate: A Comparative Single Centre Study. Clin. Oral Investig. 2021, 25, 2905–2914. [Google Scholar] [CrossRef]
- Handschel, J.; Hassanyar, H.; Depprich, R.A.; Ommerborn, M.A.; Sproll, K.C.; Hofer, M.; Kübler, N.R.; Naujoks, C. Nonvascularized Iliac Bone Grafts for Mandibular Reconstruction—Requirements and Limitations. In Vivo 2011, 25, 795–799. [Google Scholar]
- Consolo, U.; Bellini, P.; Melini, G.M.; Ferri, A.; Lizio, G. Analysis of Marsupialization of Mandibular Cysts in Improving the Healing of Related Bone Defects. J. Oral Maxillofac. Surg. 2020, 78, 1355.e1–1355.e11. [Google Scholar] [CrossRef]
- Marini, E.; Marini, L.; Messina, A.M. Treatment of Giant Maxillary Dentigerous Cyst and Ectopic Third Molar with Piezoelectric Surgery. Ital. J. Dent. Med. 2017, 2, 131–136. [Google Scholar]
- Tabrizi, R.; Hosseini Kordkheili, M.R.; Jafarian, M.; Aghdashi, F. Decompression or Marsupialization; Which Conservative Treatment Is Associated with Low Recurrence Rate in Keratocystic Odontogenic Tumors? A Systematic Review. J. Dent. 2019, 20, 145–151. [Google Scholar] [CrossRef]
- Tortorici, S.; Amodio, E.; Massenti, M.F.; Buzzanca, M.L.; Burruano, F.; Vitale, F. Prevalence and Distribution of Odontogenic Cysts in Sicily: 1986–2005. J. Oral Sci. 2008, 50, 15–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, Y.; Li, R.-F.; Sun, Y.-F.; Liu, B.; Jia, J. Pathological Fractures of the Mandible: A Report of 27. Clin. Surg. 2017, 2, 1839. [Google Scholar]
- Sanghai, S.; Chatterjee, P. A Concise Textbook of Oral and Maxillofacial Surgery; Jay-Pee Brothers Medical Publishers (P) Ltd.: New Delhi, India, 2009; pp. 134–139. [Google Scholar]
- Yamakawa, S.; Hayashida, K. Safety and Efficacy of Secondary Mandibular Reconstruction Using a Free Osteo-Cutaneous Fibula Flap after Segmental Mandibular Resection: A Retrospective Case—Control Study. BMC Surg. 2021, 21, 189. [Google Scholar] [CrossRef]
- Osborn, T.M.; Helal, D.; Mehra, P. Iliac Crest Bone Grafting for Mandibular Reconstruction: 10-Year Experience Outcomes. J. Oral Biol. Craniofac. Res. 2018, 8, 25–29. [Google Scholar] [CrossRef] [Green Version]
- Mayaleh, H.A.; Louis, M.Y. Mandibular Reconstruction Following Cyst Removal by the Autologous Cancellous Bone and Marrow Grafts. Rev. Laryngol. Otol. Rhinol. 2009, 130, 305–306. [Google Scholar]
- Cho, J.-Y.; Kim, J.-W.; Kim, S.-B.; Ryu, J. Decompression of Large Cyst Invading the Mandibular Canal Leading to Reduced Cyst Volume and Increased Mandibular Canal Length. J. Oral Maxillofac. Surg. 2020, 78, 1770–1779. [Google Scholar] [CrossRef] [PubMed]
- Riachi, F.; Khairallah, C.M.; Ghosn, N.; Berberi, A.N. Cyst Volume Changes Measured with a 3D Reconstruction after Decompression of a Mandibular Dentigerous Cyst with an Impacted Third Molar. Clin. Pract. 2019, 9, 1132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- AboulHosn, M.; Noujeim, Z.; Nader, N.; Berberi, A. Decompression and Enucleation of a Mandibular Radicular Cyst, Followed by Bone Regeneration and Implant-Supported Dental Restoration. Case Rep. Dent. 2019, 2019, 9584235. [Google Scholar] [CrossRef] [Green Version]
- Ninomiya, T.; Kubota, Y.; Koji, T.; Shirasuna, K. Marsupialization Inhibits Interleukin-1alpha Expression and Epithelial Cell Proliferation in Odontogenic Keratocysts. J. Oral Pathol. Med. 2002, 31, 526–533. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Liu, B.; Han, Q.-B.; Wang, S.-P.; Wang, Y.-N. Changes in Bone Density and Cyst Volume after Marsupialization of Mandibular Odontogenic Keratocysts (Keratocystic Odontogenic Tumors). J. Oral Maxillofac. Surg. 2011, 69, 1361–1366. [Google Scholar] [CrossRef]
- Pogrel, M.A. Decompression and Marsupialization as a Treatment for the Odontogenic Keratocyst. Oral Maxillofac. Surg. Clin. 2003, 15, 415–427. [Google Scholar] [CrossRef]
- Rajendra Santosh, A.B. Odontogenic Cysts. Dent. Clin. 2020, 64, 105–119. [Google Scholar] [CrossRef]
- Robinson, R.A. Diagnosing the Most Common Odontogenic Cystic and Osseous Lesions of the Jaws for the Practicing Pathologist. Mod. Pathol. 2017, 30, 96–103. [Google Scholar] [CrossRef] [Green Version]
- Goyal, S.; Sharma, S.; Kotru, M.; Gupta, N. Role of FNAC in the Diagnosis of Intraosseous Jaw Lesions. Med. Oral Patol. Oral Cir. Bucal 2015, 20, e284–e291. [Google Scholar] [CrossRef]
- Hallikeri, K.; Babu, B.; Sudhakaran, A.; Monteiro, R. Cell Block and Its Impact in the Diagnosis of Jaw Lesions over Fine Needle Aspiration Cytology. Acta Cytol. 2021, 65, 361–367. [Google Scholar] [CrossRef]
- Jones, A.V.; Franklin, C.D. An Analysis of Oral and Maxillofacial Pathology Found in Adults over a 30-Year Period. J. Oral Pathol. Med. 2006, 35, 392–401. [Google Scholar] [CrossRef]
- Saghravanian, N.; HosseinpourJajarm, H.; Salehinejad, J.; AfzalAghaie, M.; Ghazi, N. A 30-Year Comparison of Clinical and Histopathological Diagnoses in Salivary Gland Lesions, Odontogenic Cysts and Tumors in Mashhad Dental School-Iran. J. Mashhad Dent. Sch. 2010, 34, 299–308. [Google Scholar] [CrossRef]
- Nakamura, N.; Mitsuyasu, T.; Mitsuyasu, Y.; Taketomi, T.; Higuchi, Y.; Ohishi, M. Marsupialization for Odontogenic Keratocysts: Long-Term Follow-up Analysis of the Effects and Changes in Growth Characteristics. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2002, 94, 543–553. [Google Scholar] [CrossRef] [PubMed]
- Alberts, B.; Johnson, A.; Lewis, J.; Raff, M.; Roberts, K.; Walter, P. Fibroblasts and Their Transformations: The Connective-Tissue Cell Family. In Molecular Biology of the Cell; Garland Science: New York, NY, USA, 2002. [Google Scholar]
- Abu-Mostafa, N.; Abbasi, A. Marsupialization of a Large Dentigerous Cyst in the Mandible with Orthodontic Extrusion of Three Impacted Teeth. A Case Report. J. Clin. Exp. Dent. 2017, 9, e1162–e1166. [Google Scholar] [CrossRef] [Green Version]
- Rossi, D.; Borgonovo, A.E.; Vavassori, V.; Poli, P.P.; Santoro, F. Combined Treatment of Odontogenic Keratocysts: Initial Marsupialization and Successive Enucleation with Peripheral Ostectomy plus Carnoy’s Solution Application. A Five-Year Follow-up Experience. Minerva Stomatol. 2012, 61, 101–112. [Google Scholar] [PubMed]
- Neaverth, E.J.; Burg, H.A. Decompression of Large Periapical Cystic Lesions. J. Endod. 1982, 8, 175–182. [Google Scholar] [CrossRef]
- Habibi, A.; Saghravanian, N.; Habibi, M.; Mellati, E.; Habibi, M. Keratocystic Odontogenic Tumor: A 10-Year Retrospective Study of 83 Cases in an Iranian Population. J. Oral Sci. 2007, 49, 229–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pitak-Arnnop, P. Enucleation of Keratocystic Odontogenic Tumours: Study Interpretation, Technical Refinement and Future Research. Clin. Oral Investig. 2010, 14, 719–721. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.L.; Yang, R.; Zhang, L.; Li, W.; MacDonald-Jankowski, D.; Poh, C.F. Dentigerous Cyst: A Retrospective Clinicopathological Analysis of 2082 Dentigerous Cysts in British Columbia, Canada. Int. J. Oral Maxillofac. Surg. 2010, 39, 878–882. [Google Scholar] [CrossRef] [PubMed]
- Enislidis, G.; Fock, N.; Sulzbacher, I.; Ewers, R. Conservative Treatment of Large Cystic Lesions of the Mandible: A Prospective Study of the Effect of Decompression. Br. J. Oral Maxillofac. Surg. 2004, 42, 546–550. [Google Scholar] [CrossRef]
- Fathi AL-Omar, A.; Elmorsy, K.A. Treatment of a Large Maxillary Cyst with Marsupialization (Case Report). Oral Health Care 2018, 3, 1–4. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Irimia, A.; Moraru, L.; Ciubotaru, D.A.; Caruntu, C.; Farcasiu, A.-T.; Caruntu, A. Minimally Invasive Two-Staged Surgery in the Treatment of Large Cystic Lesions of the Jaw. Healthcare 2021, 9, 1531. https://doi.org/10.3390/healthcare9111531
Irimia A, Moraru L, Ciubotaru DA, Caruntu C, Farcasiu A-T, Caruntu A. Minimally Invasive Two-Staged Surgery in the Treatment of Large Cystic Lesions of the Jaw. Healthcare. 2021; 9(11):1531. https://doi.org/10.3390/healthcare9111531
Chicago/Turabian StyleIrimia, Andreea, Liliana Moraru, Diana Alina Ciubotaru, Constantin Caruntu, Alexandru-Titus Farcasiu, and Ana Caruntu. 2021. "Minimally Invasive Two-Staged Surgery in the Treatment of Large Cystic Lesions of the Jaw" Healthcare 9, no. 11: 1531. https://doi.org/10.3390/healthcare9111531