
Factors Contributing to Poor Self-Rated Health in Older Adults with Lower Income


Abstract
:1. Introduction
2. Materials and Methods
2.1. Source of Data
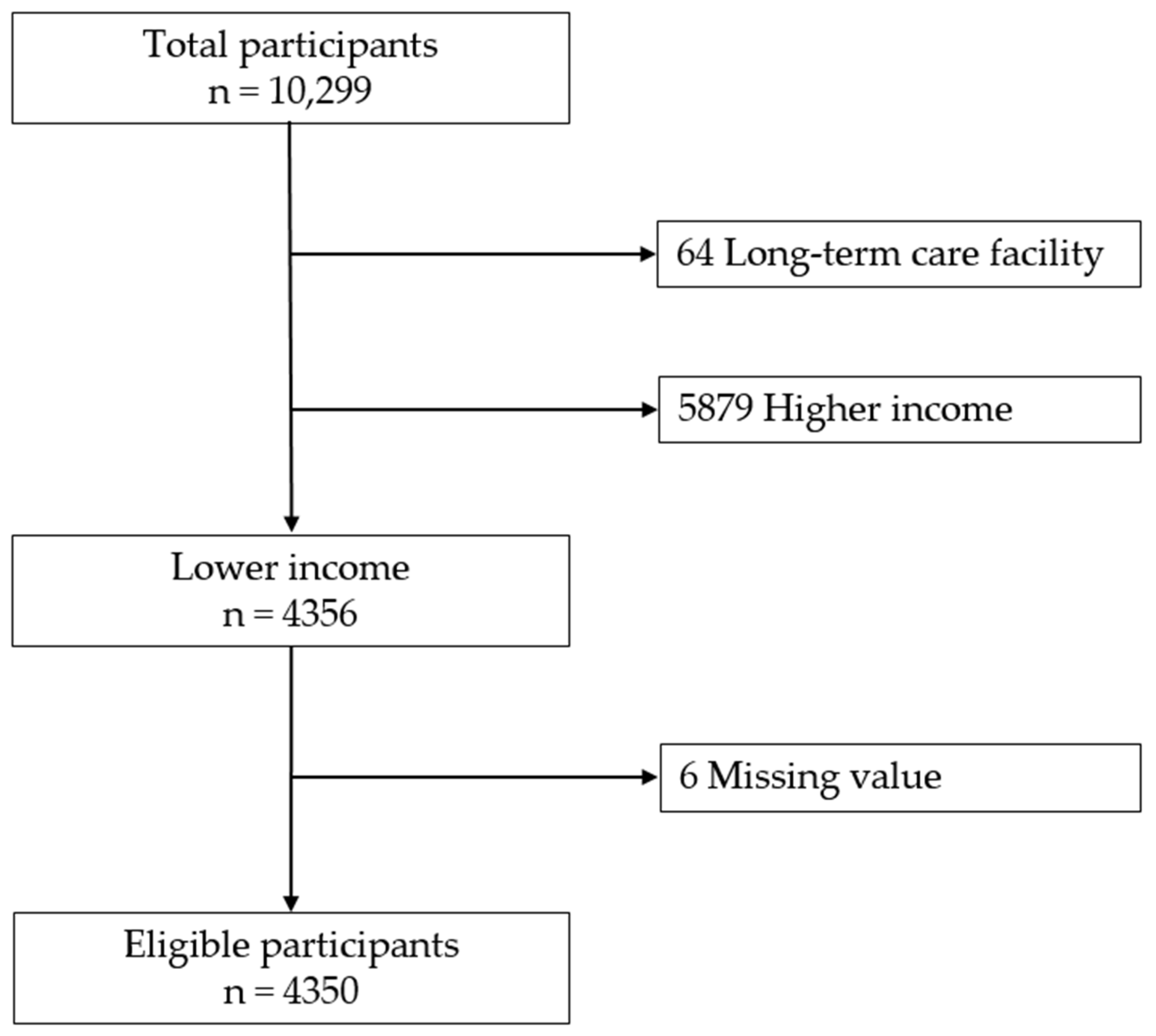
2.2. Participants Selection and Study Design
2.3. Measurements
2.3.1. Subjective Health Assessment
2.3.2. Individual Variables
2.3.3. Physical Variables
2.3.4. Psychological Variables
2.4. Statistical Analysis
3. Results
3.1. Self-Rated Health Status
3.2. Differences in Individual Characteristics between Groups with Good and Poor SRH
3.3. Differences in Physical and Psychological Factors between Good and Poor SRH Groups
3.4. Multivariable Logistic Regression Analysis of Variables Associated with Poor SRH in Low-Income Seniors Using Individual-Variable Adjusted Models
4. Discussion
4.1. Healthcare Issues among Low-Income Adults
4.2. Self-Rated Health Status in Low-Income Adults
4.3. Factors Affecting Subjective Health in Low-Income Elderly People
4.4. Strengths and Limitations of Our Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Statistics Korea (KOSTAT). Population Projections for Korea (2017–2067); Statistics Korea (KOSTAT): Daejeon, Korea, 2019.
- Statistics Korea (KOSTAT). 2020 Population and Housing Census; Statistics Korea (KOSTAT): Daejeon, Korea, 2021.
- Arendt, J.N. Income and “Outcomes” for Elderly: DO the Poor have A Poorer Life? Soc. Indic. Res. 2005, 70, 327–347. [Google Scholar] [CrossRef]
- Mossey, J.M.; Shapiro, E. Self-rated health: A predictor of mortality among the elderly. Am. J. Public Health 1982, 72, 800–808. [Google Scholar] [CrossRef] [Green Version]
- Benyamini, Y.; Idler, E.L. Community Studies Reporting Association between Self-Rated Health and Mortality:Additional Studies, 1995 to 1998. Res. Aging 1999, 21, 392–401. [Google Scholar] [CrossRef]
- Bond, J.; Dickinson, H.O.; Matthews, F.; Jagger, C.; Brayne, C. Self-rated health status as a predictor of death, functional and cognitive impairment: A longitudinal cohort study. Eur. J. Ageing 2006, 3, 193–206. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y. The predictive value of self assessed general, physical, and mental health on functional decline and mortality in older adults. J. Epidemiol. Community Health 2000, 54, 123–129. [Google Scholar] [CrossRef] [Green Version]
- Singh-Manoux, A.; Guéguen, A.; Martikainen, P.; Ferrie, J.; Marmot, M.; Shipley, M. Self-rated health and mortality: Short- and long-term associations in the Whitehall II study. Psychosom. Med. 2007, 69, 138–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rohrer, J.E.; Young, R.; Sicola, V.; Houston, M. Overall self-rated health: A new quality indicator for primary care. J. Eval. Clin. Pract. 2007, 13, 150–153. [Google Scholar] [CrossRef] [PubMed]
- Holzhausen, M.; Martus, P. Validation of a new patient-generated questionnaire for quality of life in an urban sample of elder residents. Qual. Life Res. 2013, 22, 131–135. [Google Scholar] [CrossRef]
- Gutman, G.M.; Stark, A.; Donald, A.; Beattie, B.L. Contribution of self-reported health ratings to predicting frailty, institutionalization, and death over a 5-year period. Int. Psychogeriatr. 2001, 13 (Suppl. 1), 223–231. [Google Scholar] [CrossRef] [PubMed]
- Chung, K. National Survey of Older Koreans: Findings and Implications; The Korean Institute for Health and Social Affairs: Seoul, Korea, 2018. [Google Scholar]
- WHO Guidelines Approved by the Guidelines Review Committee. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Allen, J.P. Assessing Alcohol Problems: A Guide for Clinicians and Researchers, 2nd ed.; NIH Publications: Bethesda, MD, USA, 2003.
- Won, C.W.; Yang, K.Y.; Rho, Y.G.; Kim, S.Y.; Lee, E.J.; Yoon, J.L.; Cho, K.H.; Shin, H.C.; Cho, B.R.; Oh, J.R.; et al. The Development of Korean Activities of Daily Living(K-ADL) and Korean Instrumental Activities of Daily Living(K-IADL) Scale. J. Korean Geriatr. Soc. 2002, 6, 107–120. [Google Scholar]
- Dwyer, J. Strategies to Detect and Prevent Malnutrition in the Elderly: The Nutrition Screening Initiative. Nutr. Today 1994, 29, 14–24. [Google Scholar] [CrossRef]
- Cho, M.J.; Bae, J.N.; Suh, G.H.; Hahm, B.J.; Kim, J.K.; Lee, D.W.; Kang, M.H. Validation of Geriatric Depression Scale, Korean Version(GDS) in the Assessment of DSM-III-R Major Depression. J. Korean Neuropsychiatr. Assoc. 1999, 38, 48–63. [Google Scholar]
- Rowland, D.; Lyons, B. Medicare, Medicaid, and the elderly poor. Health Care Financ. Rev. 1996, 18, 61–85. [Google Scholar]
- Marmot, M.G.; Smith, G.D.; Stansfeld, S.; Patel, C.; North, F.; Head, J.; White, I.; Brunner, E.; Feeney, A. Health inequalities among British civil servants: The Whitehall II study. Lancet 1991, 337, 1387–1393. [Google Scholar] [CrossRef]
- Mackenbach, J.P.; Kunst, A.E.; Cavelaars, A.E.; Groenhof, F.; Geurts, J.J. Socioeconomic inequalities in morbidity and mortality in western Europe. The EU Working Group on Socioeconomic Inequalities in Health. Lancet 1997, 349, 1655–1659. [Google Scholar] [CrossRef] [Green Version]
- Cavelaars, A.E.; Kunst, A.E.; Geurts, J.J.; Crialesi, R.; Grötvedt, L.; Helmert, U.; Lahelma, E.; Lundberg, O.; Matheson, J.; Mielck, A.; et al. Differences in self reported morbidity by educational level: A comparison of 11 western European countries. J. Epidemiol. Community Health 1998, 52, 219–227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ebrahimi, Z.; Wilhelmson, K.; Eklund, K.; Moore, C.D.; Jakobsson, A. Health despite frailty: Exploring influences on frail older adults’ experiences of health. Geriatr. Nurs. 2013, 34, 289–294. [Google Scholar] [CrossRef]
- Seo, Y.S. A Study on Health Behaviors and Health Status by Socioeconomic Status of Middle-Aged and Elderly; Graduate School of the Catholic University of Korea: Seoul, Korea, 2011. [Google Scholar]
- Cho, Y.H.; Park, Y.C. The Age, lifestyle and Health Status of the Elderly in a Small City. J. Korea Gerontol. Soc. 2003, 23, 141–153. [Google Scholar]
- Liang, Y.; Welmer, A.K.; Wang, R.; Song, A.; Fratiglioni, L.; Qiu, C. Trends in Incidence of Disability in Activities of Daily Living in Chinese Older Adults: 1993–2006. J. Am. Geriatr. Soc. 2017, 65, 306–312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arends, J.; Baracos, V.; Bertz, H.; Bozzetti, F.; Calder, P.C.; Deutz, N.E.P.; Erickson, N.; Laviano, A.; Lisanti, M.P.; Lobo, D.N.; et al. ESPEN expert group recommendations for action against cancer-related malnutrition. Clin. Nutr. 2017, 36, 1187–1196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, S.H. A Study on the Correlation between Social Support and Depressed in the Elderly: Analysis of the 2014 Survey of Living Conditions and Welfare Needs of Korean Older Persons; Graduate School of Public Health Yonsei University: Seoul, Korea, 2017. [Google Scholar]
- Kim, D.-B.; Sohn, E.-S. A Meta-analysis of the Variables Related to Depression in Elderly. J. Korean Gerontol. Soc. 2005, 25, 167–187. [Google Scholar]
- Chon, J.Y.; Yee, N.H. Depression in the Elderly for the Mediating Effect of Coping Strategies of Family Conflict. J. Korean Gerontol. Soc. 2011, 31, 1169–1187. [Google Scholar]
- Lee, H.J.; Jung, E.H. Socioeconomic Status and Elderly Health in Life Course Perspective: Testing of Multi-mediational Effects of Socioeconomic Status in Early Adult and Middle Aged. Health Soc. Welf. Rev. 2016, 36, 53–84. [Google Scholar]
- Kim, M.H.; Lee, G.Y.; Chung, S. A Path Analysis on Depression among the Elderly. J. Korean Gerontol. Soc. 2000, 20, 211–226. [Google Scholar]
- WHO Commission on Social Determinants of Health, World Health Organization. Closing the Gap in a Generation: Health Equity through Action on the Social Determinants of Health: Commission on Social Determinants of Health Final Report; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]



{kind=link}
{kind=link}
| Individual Variables | Classification | Good SRH | Poor SRH | χ2 | p | |
|---|---|---|---|---|---|---|
| (n = 2284) | (n = 2066) | |||||
| n (%) or | n (%) or | |||||
| M ± SD * | M ± SD * | |||||
| Demographic | Age | 76.1 ± 6.0 | 77.0 ± 6.1 | 4.96 | 0.979 | |
| Sex | Male | 817 (35.8) | 588 (28.5) | 26.51 | <0.001 | |
| Female | 1467 (64.2) | 1478 (71.5) | ||||
| Marital status | Living with spouse | 1120 (49.0) | 918 (44.4) | 9.23 | 0.002 | |
| Living without spouse | 1164 (51.0) | 1148 (55.6) | ||||
| Living status | Alone | 1072 (46.9) | 1042 (50.4) | 7.46 | 0.059 | |
| Living with spouse | 1071 (46.9) | 884 (42.8) | ||||
| Living with children | 98 (4.3) | 99 (4.8) | ||||
| Others | 43 (1.9) | 41 (2.0) | ||||
| Socioeconomic | Education | 0–6 years | 1580 (69.2) | 1626 (78.7) | 52.10 | <0.001 |
| 7–9 years | 345 (15.1) | 224 (10.8) | ||||
| 10–12 years | 280 (12.2) | 176 (8.5) | ||||
| ≥13 years | 79 (3.5) | 40 (1.9) | ||||
| Health status | Disease | Hypertension | 1342 (58.9) | 1392 (67.4) | 34.52 | <0.001 |
| Diabetes | 400 (17.5) | 616 (29.8) | 91.72 | <0.001 | ||
| Dementia | 24 (1.1) | 54 (2.6) | 15.05 | <0.001 | ||
| Arthritis | 605 (26.5) | 955 (46.2) | 183.70 | <0.001 | ||
| BMI ** | Underweight (<18.5) | 80 (3.5) | 125 (6.1) | 34.02 | <0.001 | |
| Normal (≥18.5, <25) | 1636 (71.6) | 1337 (64.7) | ||||
| Overweight (≥25) | 568 (24.9) | 604 (29.2) | ||||
| Number of medication(s) | 0 | 408 (17.9) | 88 (4.3) | 466.82 | <0.001 | |
| 1 | 308 (13.5) | 99 (4.8) | ||||
| 2 | 343 (15.0) | 149 (7.2) | ||||
| ≥3 | 1225 (53.6) | 1730 (83.7) | ||||
| Health-related Behavior | Exercise | None | 628 (27.5) | 899 (43.5) | 167.84 | <0.001 |
| <150 min. a week | 472 (20.7) | 477 (23.1) | ||||
| ≥150 min. a week | 1184 (51.8) | 690 (33.4) | ||||
| Smoking | Never/Past | 207 (9.1) | 150 (7.3) | 4.68 | 0.031 | |
| Current | 2077 (90.9) | 1916 (92.7) | ||||
| Drinking | None | 1712 (74.9) | 1726 (83.5) | 55.16 | <0.001 | |
| ≤1 standard drink/day | 212 (9.3) | 157 (7.6) | ||||
| >1 standard drink/day | 360 (15.8) | 183 (8.9) | ||||
| Physical & Psychological Variables | Classification | Good SRH | Poor SRH | χ2 | p | |
|---|---|---|---|---|---|---|
| (n = 2284) | (n = 2066) | |||||
| n (%) | n (%) | |||||
| Physical | Visual discomfort | No | 1447 (63.4) | 1081 (52.3) | 54.22 | <0.001 |
| Yes | 837 (36.6) | 985 (47.7) | ||||
| Hearing discomfort | No | 1843 (80.7) | 1521 (73.6) | 30.94 | <0.001 | |
| Yes | 441 (19.3) | 545 (26.4) | ||||
| ADL * limitation | No | 2223 (97.3) | 1739 (84.2) | 231.14 | <0.001 | |
| Yes | 61 (2.7) | 327 (15.8) | ||||
| IADL ** limitation | No | 1815 (79.5) | 1110 (53.7) | 326.25 | <0.001 | |
| Yes | 469 (20.5) | 956 (46.3) | ||||
| Nutrition | Good | 1364 (59.7) | 662 (32.0) | 333.96 | <0.001 | |
| Poor | 920 (40.3) | 1404 (68.0) | ||||
| Psychological | Depression | NoYes | 1968 (86.2) | 1103 (53.4) | 561.42 | <0.001 |
| 316 (13.8) | 963 (46.6) | |||||
| Variables | Model I | Model II | Model III | Model IV |
|---|---|---|---|---|
| OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| Visual discomfort | 1.24 (1.08–1.43) *** | 1.23 (1.07–1.42) *** | 1.10 (0.92–1.31) | 1.09 (0.95–1.27) |
| Hearing discomfort | 1.08 (0.91–1.27) | 1.08 (0.91–1.28) | 1.14 (0.98–1.31) | 1.11 (0.93–1.32) |
| ADL * limitation | 3.24 (2.38–4.41) *** | 3.25 (2.38–4.42) *** | 3.11 (2.26–4.27) *** | 2.91 (2.12–4.01) *** |
| IADL ** limitation | 2.05 (1.75–2.40) *** | 1.99 (1.70–2.33) *** | 1.91 (1.61–2.25) *** | 1.80 (1.52–2.13) *** |
| Poor nutrition | 2.10 (1.82–2.41) *** | 2.09 (1.82–2.40) *** | 1.73 (1.50–2.00)*** | 1.76 (1.52–2.04) *** |
| Depression | 3.77 (3.22–4.40) *** | 3.73 (3.19–4.37) *** | 3.80 (3.23–4.48) *** | 3.65 (3.10–4.31) *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Byun, M.; Kim, E.; Ahn, H. Factors Contributing to Poor Self-Rated Health in Older Adults with Lower Income. Healthcare 2021, 9, 1515. https://doi.org/10.3390/healthcare9111515
Byun M, Kim E, Ahn H. Factors Contributing to Poor Self-Rated Health in Older Adults with Lower Income. Healthcare. 2021; 9(11):1515. https://doi.org/10.3390/healthcare9111515
Chicago/Turabian StyleByun, Mikyong, Eunjung Kim, and Heuijune Ahn. 2021. "Factors Contributing to Poor Self-Rated Health in Older Adults with Lower Income" Healthcare 9, no. 11: 1515. https://doi.org/10.3390/healthcare9111515