
Fuzzy Cognitive Scenario Mapping for Causes of Cybersecurity in Telehealth Services

 ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
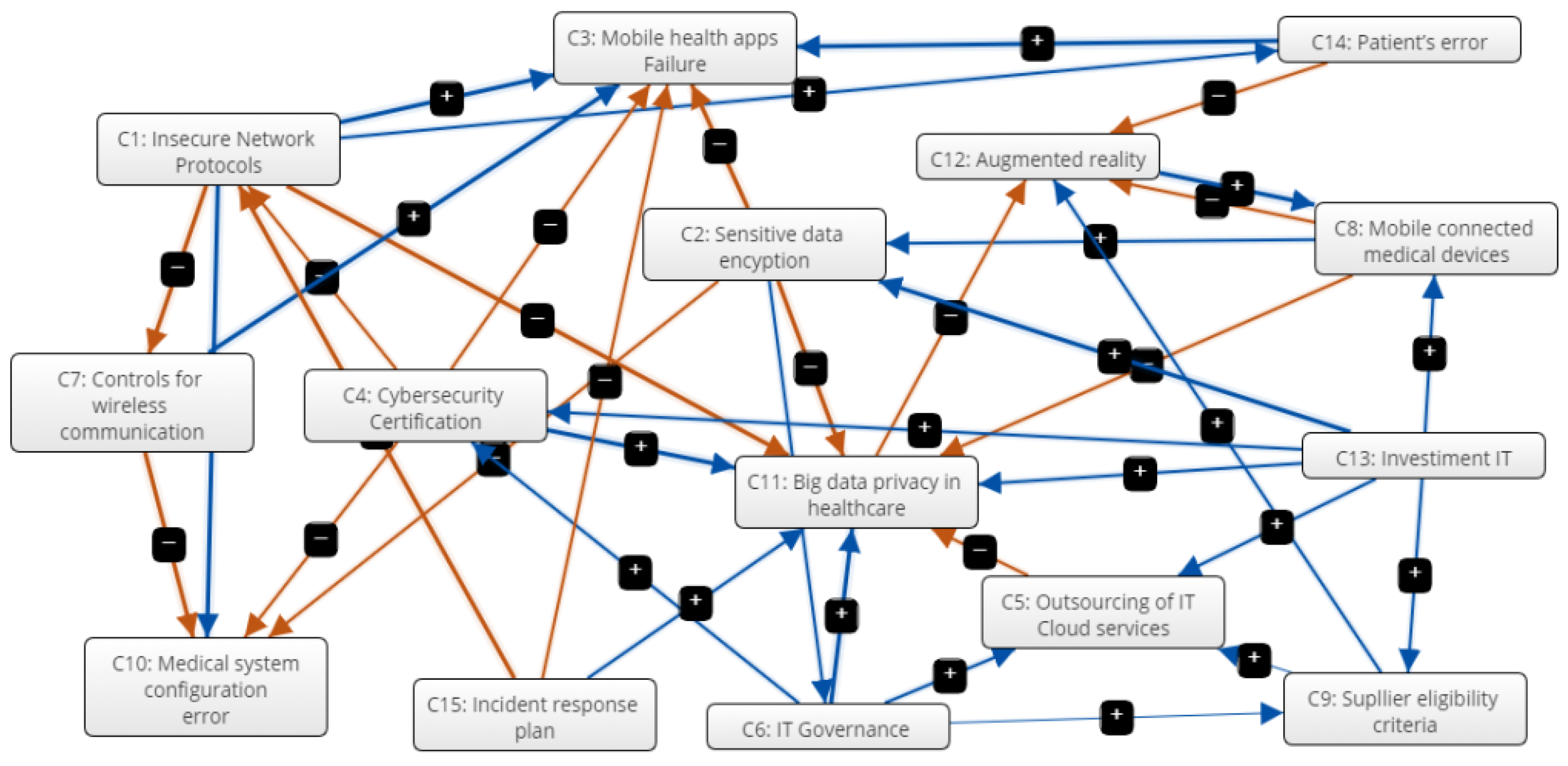
FCM Procedure
- is the value of concept Ci at step k + 1;
- is the value of the concept Cj in step k;
- is the weight of the relationship between Cj and Ci; and
- is a sigmoid threshold function defined by Equation (2):
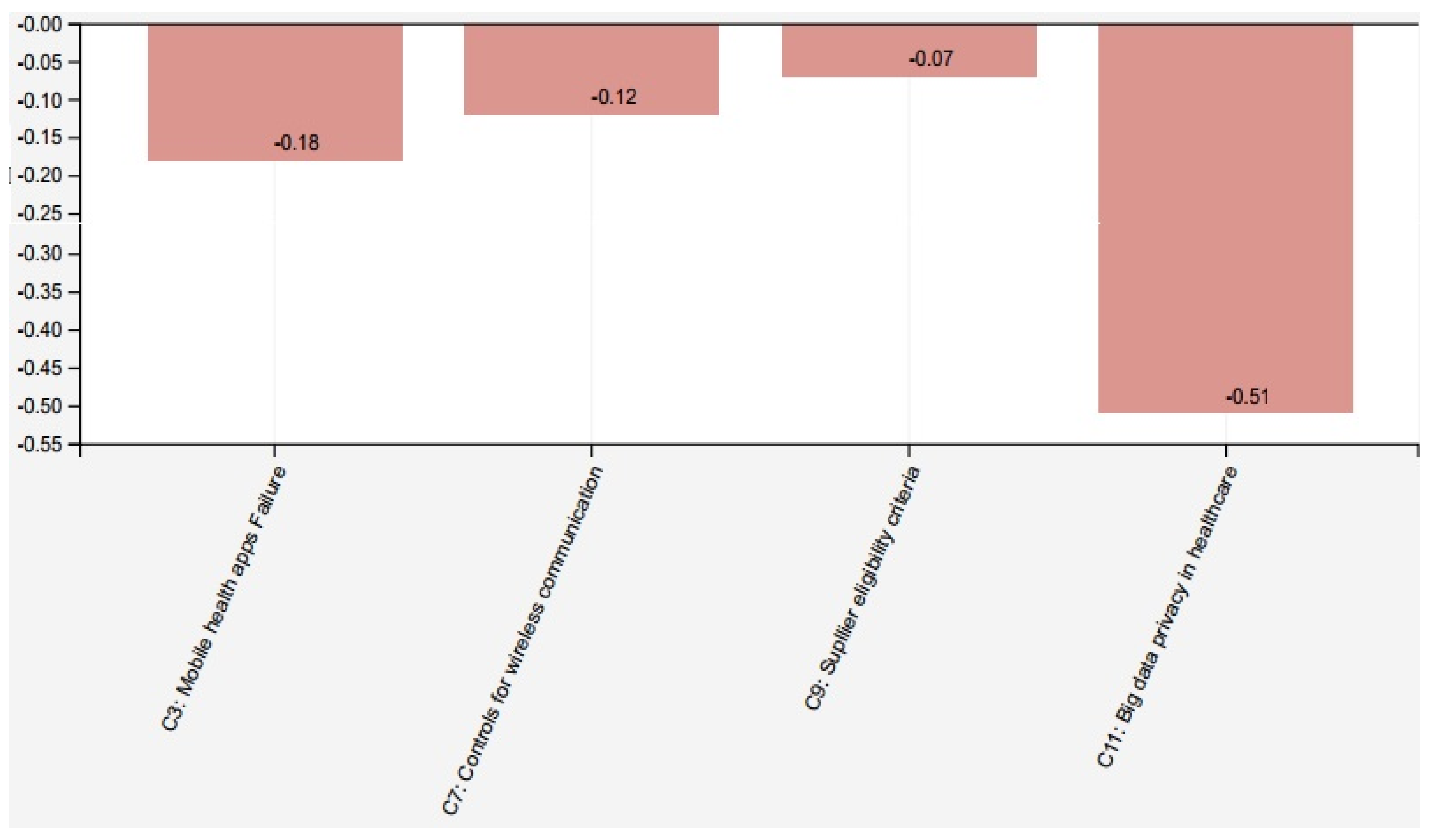
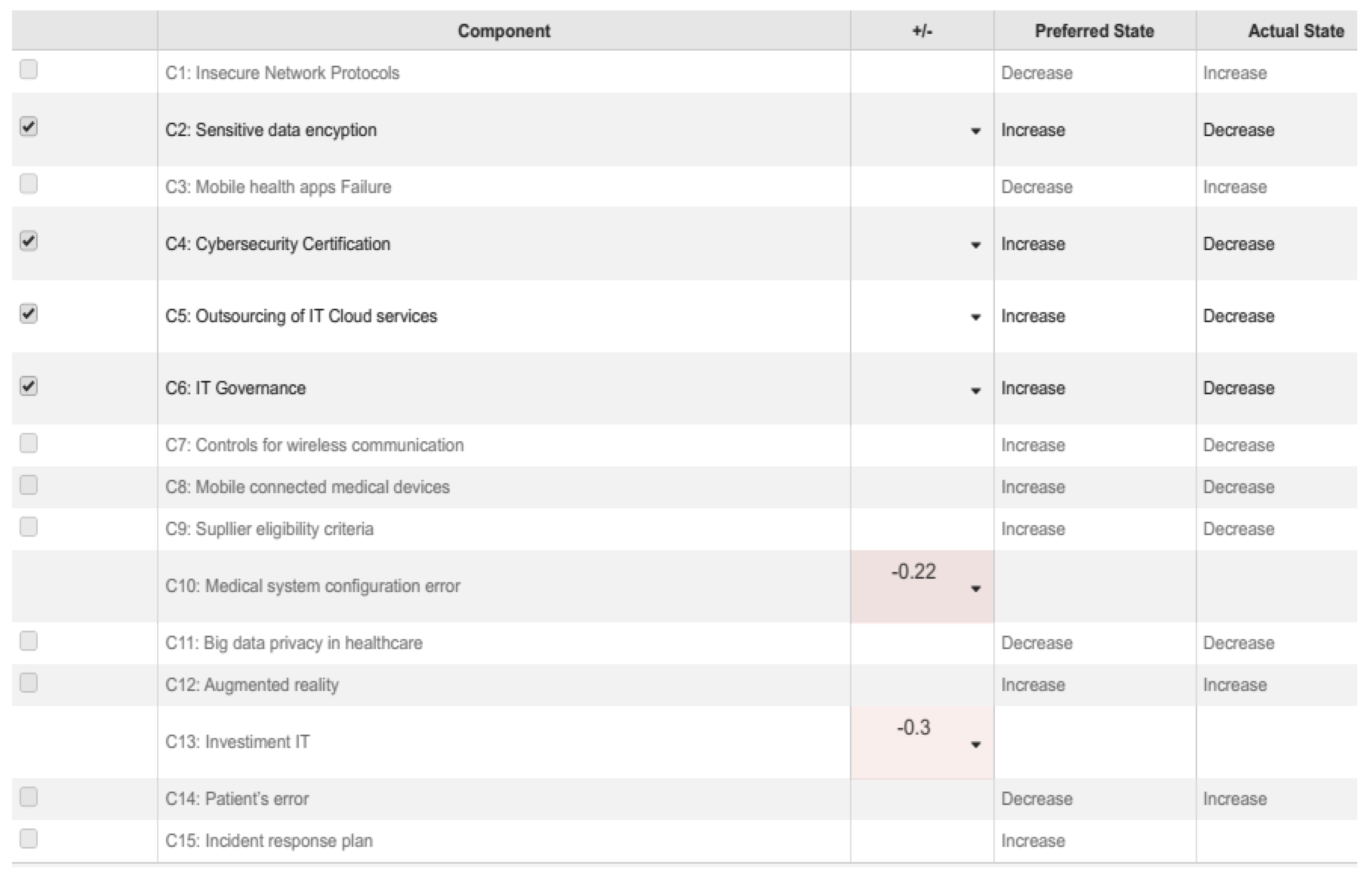
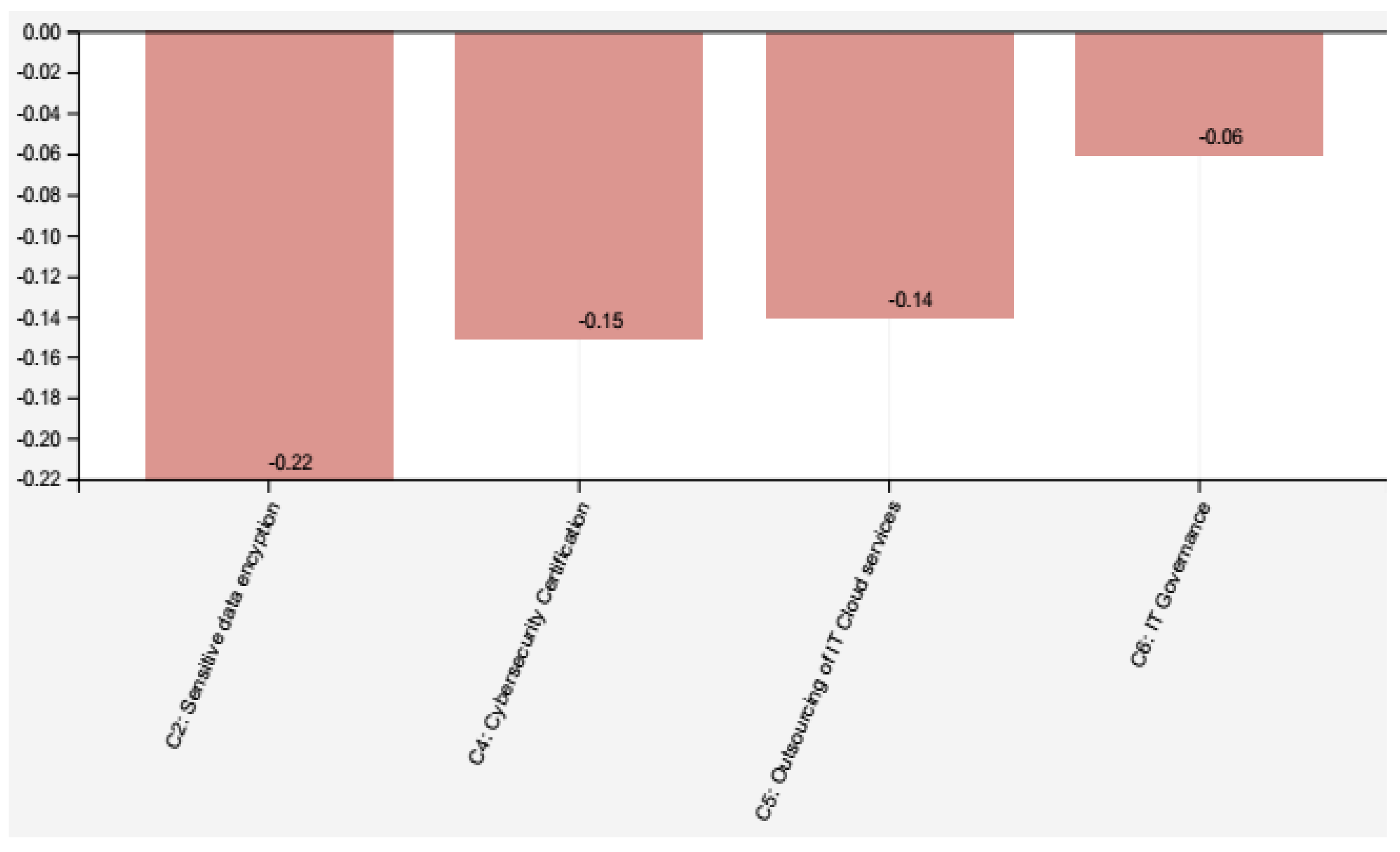
3. Results
Outputs of Scenario Analysis
4. Discussion
4.1. University Hospitals and Telehealth Cyber Security Strategies
4.2. Comparison with Other Methods/Approaches Found in Literature
5. Conceptual and Practical Implications
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bernardes, A.C.F.; Coimbra, L.C.; Serra, H.O. Utilização do Programa Telessaúde no Maranhão como ferramenta para apoiar a Educação Permanente em Saúde. Rev. Panam. Salud Públ. 2018, 42, 1–9. [Google Scholar] [CrossRef]
- Nepomuceno, T.C.C.; Silva, W.M.N.; Nepomuceno, T.C.; Barros, I.K.F. A DEA-Based Complexity of Needs Approach for Hospital Beds Evacuation during the COVID-19 Outbreak. J. Healthc. Eng. 2020, 2020, 1–9. [Google Scholar] [CrossRef]
- Woods, D.W.; Moore, T. Does Insurance Have a Future in Governing Cybersecurity? IEEE Secur. Priv. 2020, 18, 21–27. [Google Scholar] [CrossRef]
- Sokol, R.; Suter, S.; Pierce, B.; Council, L.; Grossman, E.; Roland, L.; Roll, D.; Mintzer, E. A novel transition: Lessons learned during rapid implementation and evolution of telehealth group based opioid treatment (t-GBOT) during the COVID-19 pandemic. Healthcare 2021, 9, 100559. [Google Scholar] [CrossRef]
- Maldonado, J.M.S.d.V.; Marques, A.B.; Cruz, A. Telemedicine: Challenges to dissemination in Brazil. Cad. Saude Publ. 2016, 32, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Kruse, C.S.; Krowski, N.; Rodriguez, B.; Tran, L.; Vela, J.; Brooks, M. Telehealth and patient satisfaction: A systematic review and narrative analysis. BMJ Open 2017, 7, e016242. [Google Scholar] [CrossRef]
- Rubio, J.E.; Alcaraz, C.; Roman, R.; Lopez, J. Current cyber-defense trends in industrial control systems. Comput. Secur. 2019, 87, 101561. [Google Scholar] [CrossRef]
- Sittig, D.F.; Belmont, E.; Singh, H. Improving the safety of health information technology requires shared responsibility: It is time we all step up. Healthcare 2018, 6, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, Y.; Naqvi, S.; Josephs, M. Cybersecurity Metrics for Enhanced Protection of Healthcare IT Systems. In Proceedings of the 2019 13th International Symposium on Medical Information and Communication Technology (ISMICT), Olso, Norway, 8–10 May 2019; pp. 1–9. [Google Scholar]
- Zhou, L.; Thieret, R.; Watzlaf, V.; DeAlmeida, D.; Parmanto, B. A Telehealth Privacy and Security Self-Assessment Questionnaire for Telehealth Providers: Development and Validation. Int. J. Telerehabil. 2019, 11, 3–14. [Google Scholar] [CrossRef] [Green Version]
- Alami, H.; Gagnon, M.; Ali, M.; Ahmed, A.; Fortin, J. Digital health: Cybersecurity is a value creation lever, not only a source of expenditure. Health Policy Technol. 2019, 8, 319–321. [Google Scholar] [CrossRef]
- Mendonça Silva, M.; Poleto, T.; Silva, L.C.E.; Henriques De Gusmao, A.P.; Cabral Seixas Costa, A.P. A grey theory based approach to big data risk management using FMEA. Math. Probl. Eng. 2016, 2016, 1–15. [Google Scholar] [CrossRef] [Green Version]
- De Gusmão, A.P.H.; Silva, E.L.C.; Silva, M.M.; Poleto, T.; Costa, A.P.C.S. Information security risk analysis model using fuzzy decision theory. Int. J. Inf. Manag. 2016, 36, 25–34. [Google Scholar] [CrossRef]
- Silva, M.M.; De Gusmão, A.P.H.; Poleto, T.; Silva, L.C.E.; Costa, A.P.C.S. A multidimensional approach to information security risk management using FMEA and fuzzy theory. Int. J. Inf. Manag. 2014, 34, 733–740. [Google Scholar] [CrossRef]
- De Gusmão, A.P.H.; Silva, M.M.; Poleto, T.; Silva, L.C.; Costa, A.P.C.S. Cybersecurity risk analysis model using fault tree analysis and fuzzy decision theory. Int. J. Inf. Manag. 2018, 43, 248–260. [Google Scholar] [CrossRef]
- Sun, Q.; Zhang, K.; Shi, Y. Resilient Model Predictive Control of Cyber–Physical Systems Under DoS Attacks. IEEE Trans. Ind. Inform. 2020, 16, 4920–4927. [Google Scholar] [CrossRef]
- Nifakos, S.; Chandramouli, K.; Nikolaou, C.K.; Papachristou, P.; Koch, S.; Panaousis, E.; Bonacina, S. Influence of human factors on cyber security within healthcare organisations: A systematic review. Sensors 2021, 21, 5119. [Google Scholar] [CrossRef] [PubMed]
- Zain, J.; Clarke, M. Security in telemedine: Issues in watermarking medical images. In Proceedings of the 3rd International Conference: Sciences of Electronic, Technologies of Information and Telecommunications, Susa, Tunisia, 27–31 March 2005. [Google Scholar]
- Faragallah, O.S.; Afifi, A.; El-Shafai, W.; El-Sayed, H.S.; Naeem, E.A.; Alzain, M.A.; Al-Amri, J.F.; Soh, B.; El-Samie, F.E.A. Investigation of Chaotic Image Encryption in Spatial and FrFT Domains for Cybersecurity Applications. IEEE Access 2020, 8, 42491–42503. [Google Scholar] [CrossRef]
- Lim, E.Y.S. Data Security and Protection for Medical Images. In Biomedical Information Technology; Elsevier: Amsterdam, The Netherlands, 2008; pp. 249–257. [Google Scholar]
- Andriole, K.P. Security of electronic medical information and patient privacy: What you need to know. J. Am. Coll. Radiol. 2014, 11, 1212–1216. [Google Scholar] [CrossRef]
- Nagasubramanian, G.; Sakthivel, R.K.; Patan, R.; Gandomi, A.H.; Sankayya, M.; Balusamy, B. Securing e-health records using keyless signature infrastructure blockchain technology in the cloud. Neural Comput. Appl. 2018, 639–647. [Google Scholar] [CrossRef]
- Poleto, T.; Silva, M.M.; Clemente, T.R.N.; de Gusmão, A.P.H.; Araújo, A.P.d.B.; Costa, A.P.C.S. A Risk Assessment Framework Proposal Based on Bow-Tie Analysis for Medical Image Diagnosis Sharing within Telemedicine. Sensors 2021, 21, 2426. [Google Scholar] [CrossRef]
- Barney, J.B.; Hesterly, W.S. Strategic Management and Competitive Advantage: Concepts and Cases; Pearson: Essex, UK, 2015. [Google Scholar]
- Kosko, B. Fuzzy cognitive maps. Int. J. Man. Mach. Stud. 1986, 24, 65–75. [Google Scholar] [CrossRef]
- Tsadiras, A.K. Comparing the inference capabilities of binary, trivalent and sigmoid fuzzy cognitive maps. Inf. Sci. 2008, 178, 3880–3894. [Google Scholar] [CrossRef]
- Kim, H.S.; Lee, K.C. Fuzzy implications of fuzzy cognitive map with emphasis on fuzzy causal relationship and fuzzy partially causal relationship. Fuzzy Sets Syst. 1998, 97, 303–313. [Google Scholar] [CrossRef]
- Gray, S.; Zanre, E.; Gray, S. Fuzzy Cognitive Maps as Representations of Mental Models and Group Beliefs. In Fuzzy Cognitive Maps for Applied Sciences and Engineering; Springer: Berlin/Heidelberg, Germany, 2014; pp. 29–48. [Google Scholar]
- Park, J.W.; Lee, S.J. A quantitative assessment framework for cyber-attack scenarios on nuclear power plants using relative difficulty and consequence. Ann. Nucl. Energy 2020, 142, 107432. [Google Scholar] [CrossRef]
- Hanafizadeh, P.; Ghamkhari, F. Elicitation of Tacit Knowledge Using Soft Systems Methodology. Syst. Pract. Action Res. 2019, 32, 521–555. [Google Scholar] [CrossRef]
- Papageorgiou, E.I. Learning Algorithms for Fuzzy Cognitive Maps—A Review Study. IEEE Trans. Syst. Man Cybern. Part C Appl. Rev. 2012, 42, 150–163. [Google Scholar] [CrossRef]
- Papageorgiou, E.I.; Subramanian, J.; Karmegam, A.; Papandrianos, N. A risk management model for familial breast cancer: A new application using Fuzzy Cognitive Map method. Comput. Methods Programs Biomed. 2015, 122, 123–135. [Google Scholar] [CrossRef]
- Pogliani, M.; Quarta, D.; Polino, M.; Vittone, M.; Maggi, F.; Zanero, S. Security of controlled manufacturing systems in the connected factory: The case of industrial robots. J. Comput. Virol. Hacking Tech. 2019, 15, 161–175. [Google Scholar] [CrossRef] [Green Version]
- Komporozos-Athanasiou, A. Information Technology Outsourcing in the Service Economy: Client maturity and knowledge/power asymmetries. In Information Technology in the Service Economy: Challenges and Possibilities for the 21st Century; Barrett, M., Davidson, E., Middleton, C., DeGross, J.I., Eds.; IFIP—The International Federation for Information Processing; Springer US: New York, NY, USA, 2008; Volume 267, pp. 301–310. ISBN 978-0-387-09767-1. [Google Scholar]
- Panaousis, E.; Fielder, A.; Malacaria, P.; Hankin, C.; Smeraldi, F. Cybersecurity games and investments: A decision support approach. Lect. Notes Comput. Sci. (Subser. Lect. Notes Artif. Intell. Lect. Notes Bioinform.) 2014, 8840, 266–286. [Google Scholar] [CrossRef] [Green Version]
- Dondossola, G.; Garrone, F.; Szanto, J. Cyber risk assessment of power control systems—A metrics weighed by attack experiments. In Proceedings of the IEEE Power Energy Society General Meeting, Detroit, MI, USA, 24–28 July 2011; pp. 1–9. [Google Scholar] [CrossRef]
- Alshaikh, M. Developing cybersecurity culture to influence employee behavior: A practice perspective. Comput. Secur. 2020, 98, 1–10. [Google Scholar] [CrossRef]
- Adepu, S.; Kandasamy, N.K.; Zhou, J.; Mathur, A. Attacks on smart grid: Power supply interruption and malicious power generation. Int. J. Inf. Secur. 2020, 19, 189–211. [Google Scholar] [CrossRef]
- Hu, G.; Xiao, D.; Xiang, T.; Bai, S.; Zhang, Y. A Compressive Sensing based privacy preserving outsourcing of image storage and identity authentication service in cloud. Inf. Sci. 2017, 387, 132–145. [Google Scholar] [CrossRef]
- Wang, P.; Govindarasu, M. Cyber-Physical Anomaly Detection for Power Grid with Machine Learning. In Industrial Control Systems Security and Resiliency; Springer: Berlin/Heidelberg, Germany, 2019; pp. 31–49. [Google Scholar]
- Lu, N.; Zhang, Y.; Shi, W.; Kumari, S.; Choo, K.-K.R. A secure and scalable data integrity auditing scheme based on hyperledger fabric. Comput. Secur. 2020, 92, 101741. [Google Scholar] [CrossRef]
- Namavar Jahromi, A.; Hashemi, S.; Dehghantanha, A.; Choo, K.-K.R.; Karimipour, H.; Newton, D.E.; Parizi, R.M. An improved two-hidden-layer extreme learning machine for malware hunting. Comput. Secur. 2020, 89, 101655. [Google Scholar] [CrossRef]
- Butpheng, C.; Yeh, K.-H.; Xiong, H. Security and Privacy in IoT-Cloud-Based e-Health Systems—A Comprehensive Review. Symmetry 2020, 12, 1191. [Google Scholar] [CrossRef]
- Xiang, Y.; Wang, L.; Liu, N. Coordinated attacks on electric power systems in a cyber-physical environment. Electr. Power Syst. Res. 2017, 149, 156–168. [Google Scholar] [CrossRef]
- Zachrison, K.S.; Boggs, K.M.; Hayden, E.M.; Espinola, J.A.; Camargo, C.A. Understanding Barriers to Telemedicine Implementation in Rural Emergency Departments. Ann. Emerg. Med. 2020, 75, 392–399. [Google Scholar] [CrossRef]
- Sturm, L.D.; Williams, C.B.; Camelio, J.A.; White, J.; Parker, R. Cyber-physical vulnerabilities in additive manufacturing systems: A case study attack on the STL file with human subjects. J. Manuf. Syst. 2017, 44, 154–164. [Google Scholar] [CrossRef]
- Nepomuceno, T.C.C.; Nepomuceno, K.T.C.; Costa, A.P.C.S. Contractual Misincentives in the Outsourcing of Information Technology: A Principal-Agent Approach. In Global Encyclopedia of Public Administration, Public Policy, and Governance; Springer International Publishing: Cham, Switzerland, 2020; pp. 1–10. [Google Scholar]
- Nepomuceno, T.C.C.; de Moura, J.A.; Costa, A.P.C.S. Modeling sequential bargains and personalities in democratic deliberation systems. Kybernetes 2018, 47, 1906–1923. [Google Scholar] [CrossRef]
- Wang, M.; Xu, B. Observer-based guaranteed cost control of Cyber-Physical Systems under DoS jamming attacks. Eur. J. Control. 2019, 48, 21–29. [Google Scholar] [CrossRef]
- Hong, J.; Liu, C.C.; Govindarasu, M. Integrated anomaly detection for cyber security of the substations. IEEE Trans. Smart Grid 2014, 5, 1643–1653. [Google Scholar] [CrossRef]
- Sivaprakash, A.; Rajan, S.N.E.; Selvaperumal, S. Privacy Protection of Patient Medical Images using Digital Watermarking Technique for E-healthcare System. Curr. Med. Imaging Former. Curr. Med. Imaging Rev. 2019, 15, 802–809. [Google Scholar] [CrossRef]
- Jalali, M.S.; Razak, S.; Gordon, W.; Perakslis, E.; Madnick, S. Health care and cybersecurity: Bibliometric analysis of the literature. J. Med. Internet Res. 2019, 21, e12644. [Google Scholar] [CrossRef] [PubMed]
- Nepomuceno, T.C.C.; Daraio, C.; Costa, A.P.C.S. Combining multi-criteria and directional distances to decompose non-compensatory measures of sustainable banking efficiency. Appl. Econ. Lett. 2020, 27, 329–334. [Google Scholar] [CrossRef]
- Poleto, T.; de Oliveira, R.C.P.; da Silva, A.L.B.; de Carvalho, V.D.H. Using Fuzzy Cognitive Map Approach for Assessing Cybersecurity for Telehealth Scenario. In Trends and Innovations in Information Systems and Technologies, WorldCIST 2020, Proceedings of the Advances in Intelligent Systems and Computing, Budva, Montenegro, 7–10 April 2020; Rocha, A., Adeli, H., Reis, L., Costanzo, S., Orovic, I., Moreira, F., Eds.; Springer: Berlin/Heidelberg, Germany, 2020; Volume 1160, pp. 828–837. [Google Scholar]
- Koohang, A.; Nowak, A.; Paliszkiewicz, J.; Nord, J.H. Information Security Policy Compliance: Leadership, Trust, Role Values, and Awareness. J. Comput. Inf. Syst. 2020, 60, 1–8. [Google Scholar] [CrossRef]
- Alami, H.; Gagnon, M.-P.; Fortin, J.-P.; Kouri, R.P. La télémédecine au Québec: État de la situation des considérations légales, juridiques et déontologiques. Eur. Res. Telemed./La Rech. Eur. Téléméd. 2015, 4, 33–43. [Google Scholar] [CrossRef]
- Gaines, B.R. Knowledge acquisition: Past, present and future. Int. J. Hum. Comput. Stud. 2013, 71, 135–156. [Google Scholar] [CrossRef] [Green Version]
- Handayani, P.W.; Hidayanto, A.N.; Pinem, A.A.; Hapsari, I.C.; Sandhyaduhita, P.I.; Budi, I. Acceptance model of a Hospital Information System. Int. J. Med. Inform. 2017, 99, 11–28. [Google Scholar] [CrossRef] [PubMed]
- Bergström, E.; Lundgren, M.; Ericson, Å. Revisiting information security risk management challenges: A practice perspective. Inf. Comput. Secur. 2019, 27, 358–372. [Google Scholar] [CrossRef]
- Anninou, A.P.; Groumpos, P.P.; Polychronopoulos, P. Modeling health diseases using Competitive Fuzzy Cognitive Maps. In Proceedings of the IFIP Advances in Information and Communication Technology; Springer: Berlin/Heidelberg, Germany, 2013; Volume 412, pp. 88–95. [Google Scholar]
- Mirghafoori, S.H.; Morovati Sharifabadi, A.; Karimi Takalo, S. Development of causal model of sustainable hospital supply chain management using the Intuitionistic Fuzzy Cognitive Map (IFCM) method. J. Ind. Eng. Manag. 2018, 11, 588. [Google Scholar] [CrossRef]
- Pérez-González, D.; Preciado, S.T.; Solana-Gonzalez, P. Organizational practices as antecedents of the information security management performance. Inf. Technol. People 2019, 32, 1262–1275. [Google Scholar] [CrossRef]
- de Carvalho, V.D.H.; Poleto, T.; Nepomuceno, T.C.C.; Costa, A.P.P.C.S. A study on relational factors in information technology outsourcing: Analyzing judgments of small and medium-sized supplying and contracting companies’ managers. J. Bus. Ind. Mark. 2021. ahead of publishing. [Google Scholar] [CrossRef]
- Papageorgiou, E.I.; Hatwágner, M.F.; Buruzs, A.; Kóczy, L.T. A concept reduction approach for fuzzy cognitive map models in decision making and management. Neurocomputing 2017, 232, 16–33. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Main Concepts | Description | Fuzzy Interpretation | References |
|---|---|---|---|
| C1: Insecure network protocols | Due to insecure network protocols, (HTTP), attackers can enter the organization’s network | −1: Low incompatibility network protocol 0: Average incompatibility network protocol 1: High incompatibility network protocol | [34] |
| C2: Sensitive data encryption | Involve custom code development that brings encryption into the individual application data fields | −1: Low Information Security maintenance 0: Average Information Security maintenance 1: High Information Security maintenance | [35] |
| C3: Mobile health apps failure | Operational failures occur in telehealth due to users not being prepared to adopt information security protocols. | −1: Low Operational failures occur in telehealth 0: Average Operational failures occur in telehealth 1: High Operational failures occur in telehealth | [36] |
| C4: Cybersecurity certification | Provides a rationale for why the auditable events are deemed to be adequate to support the after-fact investigations of security incidents into operational telehealth server | −1: Absolute abandonment of auditable events. 0: Average attention to auditable events. 1: Priority attention to auditable events | [37] |
| C5: Outsourcing of IT cloud services | Provides help desks, tech support, and provider to protect the confidentiality of the outsourced information. | −1: No supporting communication security. 0: A few supporting communication security. 1: Priority attention to communication security | [38] |
| C6: IT governance | Provides security strategies aligned with and supporting the business objectives | −1: Absolute abandonment of IT Governance. 0: Average attention to IT Governance. 1: Priority attention to IT Governance | [39] |
| C7: Controls for wireless communication | Establishment of policies and procedures for the effective implementation of selected security and control enhancements into telehealth. | −1: Absolute abandonment of policy access. 0: Average attention to policy access. 1: Priority attention to policy access | [40] |
| C8: Mobile connected medical devices | Lack of updates or lack of patching, a common threat that can have a significant impact on the healthcare organization | −1: Low Information Security maintenance 0: Average Information Security maintenance 1: High Information Security maintenance | [5] |
| C9: Supplier eligibility criteria | Establish security baseline requirements and translate them into eligibility criteria when selecting suppliers | −1: No supporting supplier eligibility 0: A few supporting Supplier eligibility 1: Plenty of supporting supplier eligibility | [41] |
| C10: Medical system configuration error | Medical platforms are software that needs to be installed on a practice or health system’s local server | −1: No supporting medical systems. 0: A few supportive medical systems. 1: Priority attention of medical systems. | [42] |
| C11: Big data privacy in healthcare | Big data has considerable potential to improve patient outcomes and predict outbreaks of epidemics | −1: Low Information Security maintenance 0: Average Information Security maintenance 1: High Information Security maintenance | [43] |
| C12: Augmented reality | Provide remote clinicians, such as surgeons, to guide physicians, paramedics, and other staff to perform emergency procedures in telehealth | −1: No supporting augmented reality 0: A few supporting augmented reality 1: Plenty of supporting augmented reality | [44] |
| C13: IT Investment | Provides IT investments during the pandemic, accelerating the use of telemedicine services | −1: No supporting IT Investment 0: A few supporting IT Investment 1: Plenty of supporting IT Investment | [35] |
| C14: Patient’s errors | Providers should educate patients about cybersecurity and the steps they should take to improve the overall safety of their interactions online | −1: No supporting education. 0: A few supporting education. 1: Plenty of supporting education | [45] |
| C15: Incident response plan | Systems and devices eventually fail due to inaccurate coding, improper handling, or just tear and wear | −1: No supporting incident plan. 0: A few supporting incident plan. 1: Plenty of supporting incident plans | [6] |
| Main Concepts Cybersecurity in Telehealth | Indegree | Outdegree | Centrality | Preferred State |
|---|---|---|---|---|
| C1: Insecure network protocols | 1.01 | 2.69 | 3.71 | Decrease |
| C2: Sensitive data encryption | 0.95 | 1.88 | 2.83 | Increase |
| C3: Mobile health apps failure | 3.26 | 0.00 | 3.25 | Decrease |
| C4: Cybersecurity certification | 0.65 | 1.67 | 2.32 | Increase |
| C5:Outsourcing of IT cloud services | 0.88 | 0.33 | 1.22 | Increase |
| C6: IT governance | 0.27 | 1.34 | 1.61 | Increase |
| C7: Controls for wireless communication | 0.56 | 1.05 | 1.61 | Increase |
| C8: Mobile connected medical devices | 0.91 | 0.97 | 1.88 | Increase |
| C9: Supplier eligibility criteria | 0.41 | 0.35 | 0.77 | Increase |
| C10: Medical system configuration error | 1.68 | 0.00 | 1.68 | Decrease |
| C11: Big Data privacy in healthcare | 3.82 | 0.34 | 4.17 | Decrease |
| C12: Augmented reality | 1.10 | 0.52 | 1.62 | Increase |
| C13: Investments IT | 0.00 | 2.39 | 2.39 | Increase |
| C14: Patient’s error | 0.32 | 0.89 | 1.13 | Decrease |
| C15: Incident response plan | 0.00 | 1.48 | 1.48 | Increase |
| Reference | Objective | Main Similarities | Main Differences |
|---|---|---|---|
| [10] | Develop and validate a telehealth privacy and security self-assessment questionnaire to be applied with providers. | It applies expert assessment that can be used to identify vulnerabilities in telehealth systems. | It does not establish causal relationships among the identified elements. The applied procedure is based in the application of questionnaires and psychometric analysis. |
| [12] | Present a big data risk model using Failure Mode and Effects Analysis (FMEA) and Grey Theory. | It provides a structured approach to assess risk factors, facilitating the assessment and providing a vision of risks relations. | The work uses Different methods (Failure Mode and Effects Analysis and Grey Theory). |
| [13] | Propose a risk model for information security that identify and evaluate the events’ sequence in scenarios related to the abuses of information technology systems. | The model allows ranking the risks based on their criticality, supporting the definitions of preventive or corrective actions. Use of Fuzzy Theory elements. | It does not establish causal relationships among the identified elements. Use of Event Tree Analysis. |
| [14] | Propose an approach to information security risk management based on Failure Mode and Effects Analysis (FMEA) and Fuzzy Theory. | The approach applies identification of risk elements/concepts, prioritizing risk dimensions according to the risk’s criticality, to support defining preventive or corrective actions. Use of Fuzzy Theory elements. | It does not establish causal relationships among the identified elements. Use of Failure Mode and Effects Analysis. |
| [15] | Propose a model to evaluate cybersecurity risk using Fault Tree Analysis, Decision Theory and Fuzzy Theory. | The model analyses risk scenarios also using elements from Fuzzy Theory, supporting the identification of vulnerabilities in cybersecurity linking them with potential consequences. | Use of Fault Tree Analysis, with elements from decision theory. |
| [23] | Propose a framework for cybersecurity risk management in telemedicine. | Identification of causes, consequences, and preventive measures for security threats, using scenario analysis. | Different methods (fault tree analysis and event tree analysis). |
| [29] | Propose a quantitative assessment framework to evaluate nuclear power plant risks related to cyber-attacks. | Assessment of cybersecurity risk elements, using scenarios, and providing risk information to develop preventive or corrective strategies. | Use of difficulty and consequences of cyber-attacks in the assessment, use of Bayesian belief networks and probabilistic safety assessment methods. |
| Objective | Main characteristics | Main characteristics compared to other models/approaches | |
| This work | Propose an analytical approach using Fuzzy Cognitive Maps (FCM) representing experts’ opinions about causal relationships of concepts related to cybersecurity in telehealth systems, providing support for strategic planning and decision-making | Use of expert knowledge creating a graphical representation about expert reasoning about cybersecurity threats, aiding to prioritize them according to scenarios. Support to cybersecurity strategies development by understanding the causal relationships between the concepts. | The approach applied in this study do not consider the probabilistic component involved in risk analysis, in its mathematical formulation to generate de graphs from FCM. Most of the methods or approaches previously presented deal with probabilistic data about the security threats. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Poleto, T.; Carvalho, V.D.H.d.; Silva, A.L.B.d.; Clemente, T.R.N.; Silva, M.M.; Gusmão, A.P.H.d.; Costa, A.P.C.S.; Nepomuceno, T.C.C. Fuzzy Cognitive Scenario Mapping for Causes of Cybersecurity in Telehealth Services. Healthcare 2021, 9, 1504. https://doi.org/10.3390/healthcare9111504
Poleto T, Carvalho VDHd, Silva ALBd, Clemente TRN, Silva MM, Gusmão APHd, Costa APCS, Nepomuceno TCC. Fuzzy Cognitive Scenario Mapping for Causes of Cybersecurity in Telehealth Services. Healthcare. 2021; 9(11):1504. https://doi.org/10.3390/healthcare9111504
Chicago/Turabian StylePoleto, Thiago, Victor Diogho Heuer de Carvalho, Ayara Letícia Bentes da Silva, Thárcylla Rebecca Negreiros Clemente, Maísa Mendonça Silva, Ana Paula Henriques de Gusmão, Ana Paula Cabral Seixas Costa, and Thyago Celso Cavalcante Nepomuceno. 2021. "Fuzzy Cognitive Scenario Mapping for Causes of Cybersecurity in Telehealth Services" Healthcare 9, no. 11: 1504. https://doi.org/10.3390/healthcare9111504