
Study on the Types of Elderly Intelligent Health Management Technology and the Influencing Factors of Its Adoption


Abstract
:1. Introduction
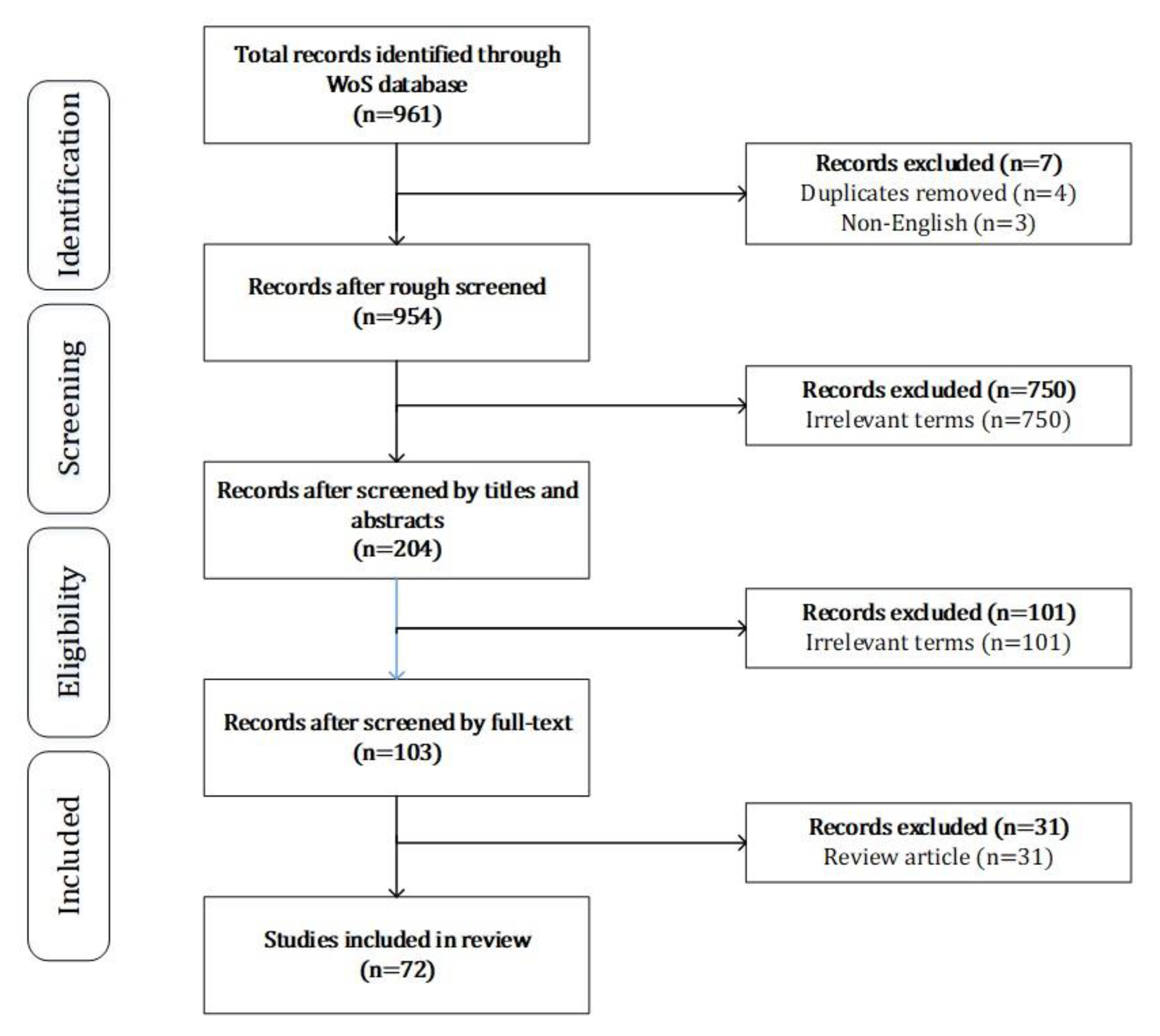
2. Materials and Methods
3. Results
3.1. Types of IHMT
3.1.1. Self-Monitoring
3.1.2. Medical Care
3.1.3. Remote Monitoring
3.1.4. Health Education
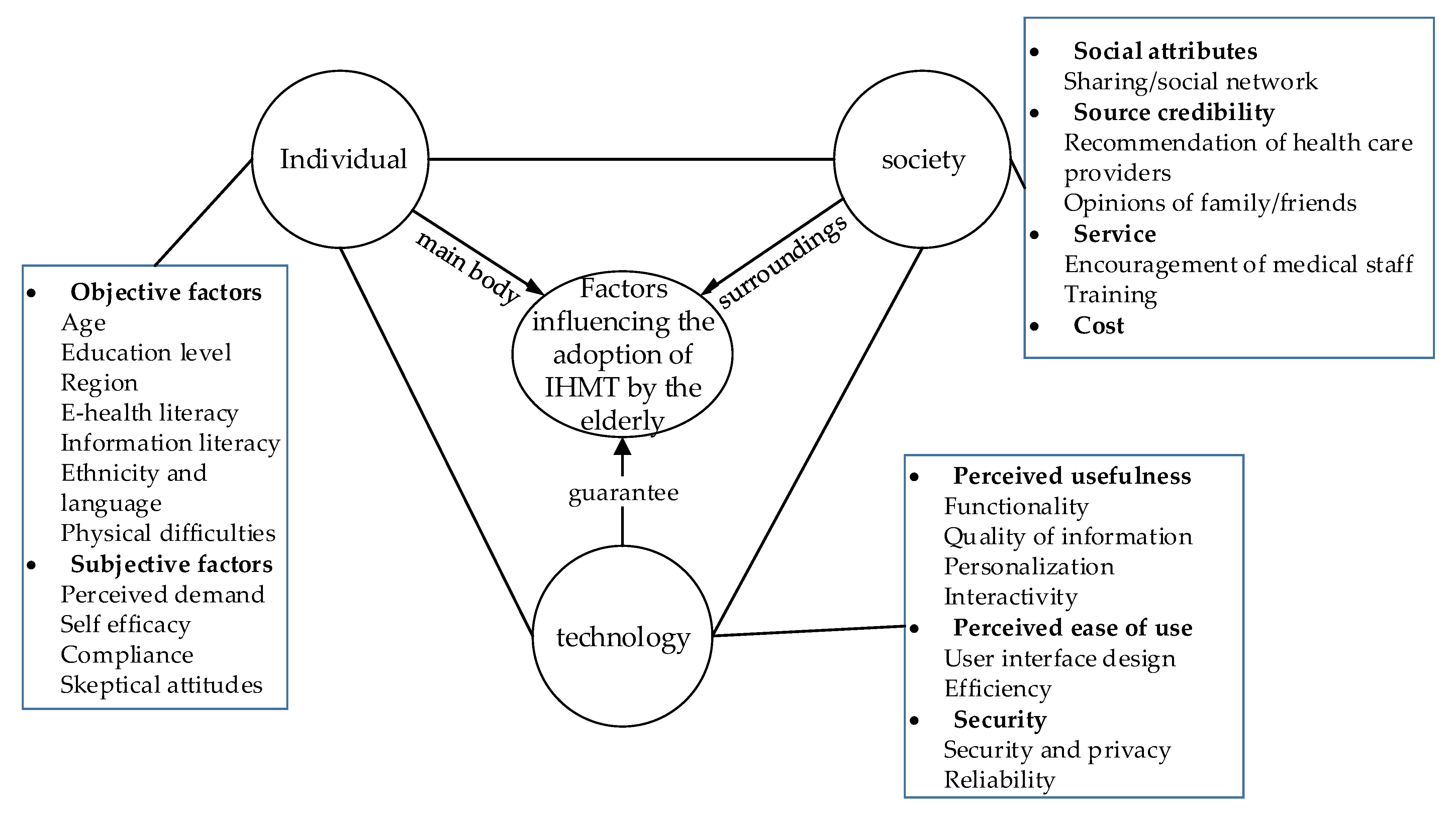
3.2. Influencing Factors of the Elderly Adopting IHMT
3.2.1. Individual Level
- Objective factors
- 2.
- Subjective factors
3.2.2. Social Level
- Social attributes
- 2.
- Source credibility
- 3.
- Service
- 4.
- Cost
3.2.3. Technical Level
- Perceived usefulness
- 2.
- Perceived ease of use
- 3.
- Security
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| IHMT | intelligent health management technology |
| IoT | Internet of things |
| QOL | quality of life |
| MCI | mild cognitive impairment |
| app | application |
References
- The State Council the People’s Republic of China. Available online: http://www.gov.cn/shuju/2017-03/23/content_5180093.htm (accessed on 17 September 2021).
- Zou, P.; Stinson, J.; Parry, M.; Dennis, C.L.; Yang, Y.Q.; Lu, Z.Q. A smartphone app (mDASHNa-CC) to support healthy diet and hypertension control for Chinese Canadian seniors: Protocol for design, usability and feasibility testing. JMIR Res. Protoc. 2020, 9, 11.e15545. [Google Scholar] [CrossRef]
- Kato, S.; Ando, M.; Kondo, T.; Yoshida, Y.; Honda, H.; Maruyama, S. Lifestyle intervention using Internet of Things (IoT) for the elderly: A study protocol for a randomized control trial (the BEST-LIFE study). Nagoya J. Med. Sci. 2018, 80, 175–182. [Google Scholar] [CrossRef]
- Chau, J.P.C.; Lee, D.T.F.; Yu, D.S.F.; Chow, A.Y.M.; Yu, W.C.; Chair, S.Y.; Lai, A.S.F.; Chick, Y.L. A feasibility study to investigate the acceptability and potential effectiveness of a telecare service for older people with chronic obstructive pulmonary disease. J. Healthc. Inform. Res. 2012, 81, 674–682. [Google Scholar] [CrossRef] [PubMed]
- Irizarry, T.; Shoemake, J.; Nilsen, M.L.; Czaja, S.; Beach, S.; Dabbs, A.D. Patient portals as a tool for health care engagement: A mixed-method study of older adults with varying levels of health literacy and prior patient portal use. J. Med. Internet Res. 2017, 19, 22.e99. [Google Scholar] [CrossRef] [PubMed]
- Chung, J.; Demiris, G.; Thompson, H.J. Ethical considerations regarding the use of smart home technologies for older adults: An integrative review. Annu. Rev. Nurs. Res. 2019, 34, 155–181. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reeder, B.; Demiris, G.; Marek, K.D. Older adults’ satisfaction with a medication dispensing device in home care. Inform. Health Soc. Care 2013, 38, 211–222. [Google Scholar] [CrossRef] [PubMed]
- McManus, D.D.; Chong, J.W.; Soni, A.; Saczynski, J.S.; Esa, N.; Napolitano, C.; Darling, C.E.; Boyer, E.; Rosen, R.K.; Floyd, K.C.; et al. PULSE-SMART: Pulse-based arrhythmia discrimination using a Novel smartphone application. J. Cardiovasc. Electrophysiol. 2016, 27, 51–57. [Google Scholar] [CrossRef]
- Portz, J.D.; Vehovec, A.; Dolansky, M.A.; Levin, J.B.; Bull, S.; Boxer, R. The development and acceptability of a mobile application for tracking symptoms of heart failure among older adults. Telemed. J. E-Health 2018, 24, 161–165. [Google Scholar] [CrossRef] [PubMed]
- Quinn, C.C.; Khokhar, B.; Weed, K.; Barr, E.; Gruber-Baldini, A.L. Older adult self-efficacy study of mobile phone diabetes management. Diabetes Technol. Ther. 2015, 17, 455–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rasche, P.; Wille, M.; Brohl, C.; Theis, S.; Schafer, K.; Knobe, M.; Mertens, A. Prevalence of Health app use among older adults in Germany: National survey. JMIR Mhealth Uhealth 2018, 6, 11.e26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Still, C.H.; Jones, L.M.; Moss, K.O.; Variath, M.; Wright, K.D. African American older adults’ perceived use of technology for hypertension self-management. Res. Gerontol. Nurs. 2018, 11, 249–256. [Google Scholar] [CrossRef]
- Gould, C.E.; Loup, J.; Kuhn, E.; Beaudreau, S.A.; Ma, F.; Goldstein, M.K.; Wetherell, J.L.; Zapata, A.M.L.; Choe, P.; O’Hara, R. Technology use and preferences for mental health self-management interventions among older veterans. Int. J. Geriatr. Psychiatry 2020, 35, 321–330. [Google Scholar] [CrossRef] [PubMed]
- Willard, S.; Cremers, G.; Man, Y.P.; van Rossum, E.; Spreeuwenberg, M.; de Witte, L. Development and testing of an online community care platform for frail older adults in the Netherlands: A user-centred design. BMC Geriatr. 2018, 18, 87. [Google Scholar] [CrossRef] [PubMed]
- Hermanns, M.; Haas, B.K.; Lisk, J. Engaging older adults with Parkinson’s disease in physical activity using technology: A feasibility study. Gerontol. Geriatr. Med. 2019, 5, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Batsis, J.A.; Zagaria, A.B.; Halter, R.J.; Boateng, G.G.; Proctor, P.; Bartels, S.J.; Kotz, D. Use of Amulet in behavioral change for geriatric obesity management. Digit. Health 2019, 5, 7. [Google Scholar] [CrossRef] [PubMed]
- Zaslavsky, O.; Thompson, H.J.; McCurry, S.M.; Landis, C.A.; Kitsiou, S.; Ward, T.M.; Heitkemper, M.M.; Demiris, G. Use of a wearable technology and motivational interviews to improve sleep in older adults with osteoarthritis and sleep disturbance: A pilot study. Res. Gerontol. Nurs. 2019, 12, 167–173. [Google Scholar] [CrossRef]
- Zhang, Y.T.; Fang, Y.; Xu, Y.; Xiong, P.; Zhang, J.Y.; Yang, J.R.; Ran, L.; Tan, X.D. Adherence with blood pressure monitoring wearable device among the elderly with hypertension: The case of rural China. Brain Behav. 2020, 10, 9.e01599. [Google Scholar] [CrossRef]
- Fanning, J.; Brooks, A.K.; Ip, E.; Nicklas, B.J.; Rejeski, W.J. A Mobile health intervention to reduce pain and improve health (MORPH) in older adults with obesity: Protocol for the MORPH trial. JMIR Res. Protoc. 2018, 7, 11.e128. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.H.; Lin, Y.H.; Hung, C.S.; Huang, C.C.; Yeih, D.F.; Chuang, P.Y.; Ho, Y.L.; Chen, M.F. Clinical outcome and cost-effectiveness of a synchronous telehealth service for seniors and nonseniors with cardiovascular diseases: Quasi-experimental study. J. Med. Internet Res. 2013, 15, 11.e87. [Google Scholar] [CrossRef]
- Zhou, M.; Zhao, L.D.; Kong, N.; Campy, K.S.; Qu, S.J.; Wang, S. Factors influencing behavior intentions to telehealth by Chinese elderly: An extended TAM model. Int. J. Med. Inform. 2019, 126, 118–127. [Google Scholar] [CrossRef]
- Parker, S.J.; Jessel, S.; Richardson, J.E.; Reid, M.C. Older adults are mobile too! Identifying the barriers and facilitators to older adults’ use of mHealth for pain management. BMC Geriatr. 2013, 13, 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, K.; Kim, S.; Lee, E.; Park, J.Y. Mobile app use for insomnia self-management in urban community-dwelling older Korean adults: Retrospective intervention study. JMIR Mhealth Uhealth 2020, 8, 17.e17755. [Google Scholar] [CrossRef] [PubMed]
- Goransson, C.; Wengstrom, Y.; Halleberg-Nyman, M.; Langius-Eklof, A.; Ziegert, K.; Blomberg, K. An app for supporting older people receiving home care—Usage, aspects of health and health literacy: A quasi-experimental study. BMC Med. Inform. Decis. Mak. 2020, 20, 226. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.A.; Nguyen, A.L.; Berg, J.; Amin, A.; Bachman, M.; Guo, Y.Q.; Evangelista, L. Attitudes and preferences on the use of mobile health technology and health games for self-management: Interviews with older adults on anticoagulation therapy. JMIR Mhealth Uhealth 2014, 2, 12.e32. [Google Scholar] [CrossRef]
- Goransson, C.; Eriksson, I.; Ziegert, K.; Wengstrom, Y.; Langius-Eklof, A.; Brovall, M.; Kihlgren, A.; Blomberg, K. Testing an app for reporting health concerns-Experiences from older people and home care nurses. Int. J. Older People Nurs. 2018, 13, 10.e12181. [Google Scholar] [CrossRef] [PubMed]
- Taha, J.; Czaja, S.J.; Sharit, J.; Morrow, D.G. Factors affecting usage of a personal health record (PHR) to manage health. Psychol. Aging 2013, 28, 1124–1139. [Google Scholar] [CrossRef] [PubMed]
- Belli, H.M.; Chokshi, S.K.; Hegde, R.; Troxel, A.B.; Blecker, S.; Testa, P.A.; Anderman, J.; Wong, C.; Mann, D.M. Implementation of a behavioral economics electronic health record (BE-EHR) module to reduce overtreatment of diabetes in older adults. J. Gen. Intern. Med. 2020, 35, 3254–3261. [Google Scholar] [CrossRef]
- Choi, M. Association of eHealth use, literacy, informational social support, and health-promoting behaviors: Mediation of health self-efficacy. Int. J. Environ. Res. Public Health 2020, 17, 12. [Google Scholar] [CrossRef] [PubMed]
- Kullgren, J.T.; Harkins, K.A.; Bellamy, S.L.; Gonzales, A.; Tao, Y.Y.; Zhu, J.S.; Volpp, K.G.; Asch, D.A.; Heisler, M.; Karlawish, J. A mixed-methods randomized controlled trial of financial incentives and peer networks to promote walking among older adults. Health Educ. Behav. 2014, 41, 43S–50S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McMahon, S.K.; Lewis, B.; Oakes, M.; Guan, W.H.; Wyman, J.F.; Rothman, A.J. Older Adults’ experiences using a commercially available monitor to self-track their physical activity. JMIR Mhealth Uhealth 2016, 4, 594–603. [Google Scholar] [CrossRef]
- Portz, J.D.; Bayliss, E.A.; Bull, S.; Boxer, R.S.; Bekelman, D.B.; Gleason, K.; Czaja, S. Using the technology acceptance model to explore user experience, intent to use, and use behavior of a patient portal among older adults with multiple chronic conditions: Descriptive qualitative study. J. Med. Internet Res. 2019, 21, 12.e11604. [Google Scholar] [CrossRef] [PubMed]
- Brath, H.; Morak, J.; Kastenbauer, T.; Modre-Osprian, R.; Strohner-Kastenbauer, H.; Schwarz, M.; Kort, W.; Schreier, G. Mobile health (mHealth) based medication adherence measurement—A pilot trial using electronic blisters in diabetes patients. Br. J. Clin. Pharmacol. 2013, 76, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Turchioe, M.R.; Grossman, L.V.; Baik, D.; Lee, C.T.S.; Maurer, M.S.; Goyal, P.; Safford, M.M.; Creber, R.M.M. Older Adults can successfully monitor symptoms using an inclusively designed mobile application. J. Am. Geriatr. Soc. 2020, 68, 1313–1318. [Google Scholar] [CrossRef] [PubMed]
- Sheeran, T.; Rabinowitz, T.; Lotterman, J.; Reilly, C.F.; Brown, S.; Donehower, P.; Ellsworth, E.; Amour, J.L.; Bruce, M.L. Feasibility and impact of telemonitor-based depression care management for geriatric homecare patients. Telemed. J. E-Health 2011, 17, 620–626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gellis, Z.D.; Kenaley, B.; McGinty, J.; Bardelli, E.; Davitt, J.; Ten Have, T. Outcomes of a telehealth intervention for homebound older adults with heart or chronic respiratory failure: A randomized controlled trial. Gerontologist 2012, 52, 541–552. [Google Scholar] [CrossRef] [Green Version]
- Taha, J.; Sharit, J.; Czaja, S.J. The Impact of numeracy ability and technology skills on older adults’ performance of health management tasks using a patient portal. J. Appl. Gerontol. 2014, 33, 416–436. [Google Scholar] [CrossRef]
- Creber, R.M.M.; Hickey, K.T.; Maurer, M.S. Gerontechnologies for older patients with heart failure: What is the role of smartphones, tablets, and remote monitoring devices in improving symptom monitoring and self-care management? Curr. Cardiovasc. Risk Rep. 2016, 10, 8. [Google Scholar] [CrossRef] [Green Version]
- Bakas, T.; Sampsel, D.; Israel, J.; Chamnikar, A.; Ellard, A.; Clark, J.G.; Ulrich, M.G.; Vanderelst, D. Satisfaction and technology evaluation of a telehealth robotic program to optimize healthy independent living for older adults. J. Nurs. Scholarsh. 2018, 50, 666–675. [Google Scholar] [CrossRef]
- Richard, E.; Jongstra, S.; Soininen, H.; Brayne, C.; van Charante, E.P.M.; Meiller, Y.; van der Groep, B.; Beishuizen, C.R.L.; Mangialasche, F.; Barbera, M.; et al. Healthy ageing through internet counselling in the elderly: The HATICE randomised controlled trial for the prevention of cardiovascular disease and cognitive impairment. BMJ Open 2016, 6, 10.e010806. [Google Scholar] [CrossRef]
- Vanoh, D.; Ishak, I.H.; Shahar, S.; Manaf, Z.A.; Ali, N.M.; Noah, H.A.M. Development and assessment of a web-based intervention for educating older people on strategies promoting healthy cognition. Clin. Interv. Aging 2018, 13, 1787–1798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kakulla, B. Older Adults Keep Pace on Tech Usage. AARP Research. Available online: https://www.aarp.org/research/topics/technology/info-2019/2020-technology-trends-older-americans.html (accessed on 17 September 2021).
- Gordon, N.P.; Hornbrook, M.C. Older adults’ readiness to engage with eHealth patient education and self-care resources: A cross-sectional survey. BMC Health Serv. Res. 2018, 18, 13. [Google Scholar] [CrossRef] [PubMed]
- Nymberg, V.M.; Bolmsjo, B.B.; Wolff, M.; Calling, S.; Gerward, S.; Sandberg, M. ‘Having to learn this so late in our lives...’ Swedish elderly patients’ beliefs, experiences, attitudes and expectations of e-health in primary health care. Scand. J. Prim. Health Care 2019, 37, 41–52. [Google Scholar] [CrossRef] [Green Version]
- Quintana, Y.; Fahy, D.; Abdelfattah, A.M.; Henao, J.; Safran, C. The design and methodology of a usability protocol for the management of medications by families for aging older adults. BMC Med. Inform. Decis. Mak. 2019, 19, 5. [Google Scholar] [CrossRef] [Green Version]
- Jonker, L.T.; Plas, M.; de Bock, G.H.; Buskens, E.; van Leeuwen, B.L.; Lahr, M.M.H. Remote Home monitoring of older surgical cancer patients: Perspective on study implementation and feasibility. Ann. Surg. Oncol. 2021, 28, 67–78. [Google Scholar] [CrossRef] [PubMed]
- Batsis, J.A.; Dokko, R.; Naslund, J.A.; Zagaria, A.B.; Kotz, D.; Bartels, S.J.; Carpenter-Song, E. Opportunities to Improve a mobile obesity wellness intervention for rural older adults with obesity. J. Community Health 2020, 45, 94–200. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, L.; Keshavjee, K.; Archer, N.; Patterson, C.; Gwadry-Sridhar, F.; Demers, C. Barriers to technology use among older heart failure individuals in managing their symptoms after hospital discharge. Int. J. Med. Inform. 2017, 105, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Middlemass, J.B.; Vos, J.; Siriwardena, A.N. Perceptions on use of home telemonitoring in patients with long term conditions—Concordance with the Health Information Technology Acceptance Model: A qualitative collective case study. BMC Med. Inform. Decis. Mak. 2017, 17, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Askari, M.; Klaver, N.S.; van Gestel, T.J.; van de Klundert, J. Intention to use medical apps among older adults in The Netherlands: Cross-sectional study. J. Med. Internet Res. 2020, 22, 12.e18080. [Google Scholar] [CrossRef] [PubMed]
- Mira, J.J.; Navarro, I.; Botella, F.; Borras, F.; Nuno-Solinis, R.; Orozco, D.; Iglesias-Alonso, F.; Perez-Perez, P.; Lorenzo, S.; Toro, N. A Spanish pillbox app for elderly patients taking multiple medications: Randomized controlled trial. J. Med. Internet Res. 2014, 16, 117–130.e99. [Google Scholar] [CrossRef] [Green Version]
- Meguerditchian, A.; Tamblyn, R.; Meterissian, S.; Law, S.; Prchal, J.; Winslade, N.; Stern, D. Adjuvant Endocrine therapy in breast cancer: A Novel e-Health approach in optimizing treatment for seniors (OPTIMUM): A two-group controlled comparison pilot study. JMIR Res. Protoc. 2016, 5, 14.e199. [Google Scholar] [CrossRef]
- Guo, Y.T.; Chen, Y.D.; Lane, D.A.; Liu, L.H.; Wang, Y.T.; Lip, G.Y.H. Mobile health technology for atrial fibrillation management integrating decision support, education, and patient involvement: mAF app trial. Am. J. Med. 2017, 130, 1388–1396.e6. [Google Scholar] [CrossRef] [Green Version]
- Mansson, L.; Lundin-Olsson, L.; Skelton, D.A.; Janols, R.; Lindgren, H.; Rosendahl, E.; Sandlund, M. Older adults’ preferences for, adherence to and experiences of two self-management falls prevention home exercise programmes: A comparison between a digital programme and a paper booklet. BMC Geriatr. 2020, 20, 15. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.L.; Zhao, Y.; Yu, L.S.; Liu, J.X.; Zwetsloot, I.M.; Cabrera, J.; Tsui, K.L. A personalized health monitoring system for community-dwelling elderly people in Hong Kong: Design, implementation, and evaluation study. J. Med. Internet Res. 2020, 22, e19223. [Google Scholar] [CrossRef] [PubMed]
- Huh, J.; Le, T.; Reeder, B.; Thompson, H.J.; Demiris, G. Perspectives on wellness self-monitoring tools for older adults. Int. J. Med. Inform. 2013, 82, 1092–1103. [Google Scholar] [CrossRef] [Green Version]
- Kutz, D.; Shankar, K.; Connelly, K. Making sense of mobile- and web-based wellness information technology: Cross-generational study. J. Med. Internet Res. 2013, 15, e83. [Google Scholar] [CrossRef] [PubMed]
- Disler, R.T.; Inglis, S.C.; Newton, P.; Currow, D.C.; Macdonald, P.S.; Glanville, A.R.; Donesky, D.; Carrieri-Kohlman, V.; Davidson, P.M. Older patients’ perspectives of online health approaches in chronic obstructive pulmonary disease. Telemed. J. E-Health 2019, 25, 840–846. [Google Scholar] [CrossRef] [PubMed]
- Contreras-Somoza, L.M.; Irazoki, E.; Castilla, D.; Botella, C.; Toribio-Guzman, J.M.; Parra-Vidales, E.; Suso-Ribera, C.; Suarez-Lopez, P.; Perea-Bartolome, M.V.; Franco-Martin, M.A. Study on the acceptability of an ICT Platform for older adults with mild cognitive impairment. J. Med. Syst. 2020, 44, 12. [Google Scholar] [CrossRef] [PubMed]
- Cajita, M.I.; Hodgson, N.A.; Lam, K.W.; Yoo, S.; Han, H.R. Facilitators of and Barriers to mHealth adoption in older adults with heart failure. Comput. Inform. Nurs. 2018, 36, 376–382. [Google Scholar] [CrossRef]
- Sun, C.L.; Sun, L.; Xi, S.G.; Zhang, H.; Wang, H.; Feng, Y.K.; Deng, Y.F.; Wang, H.M.; Xiao, X.C.; Wang, G.; et al. Mobile phone-based telemedicine practice in older Chinese patients with Type 2 diabetes mellitus: Randomized controlled trial. JMIR Mhealth Uhealth 2019, 7, e10664. [Google Scholar] [CrossRef]
- Kastner, M.; Makarski, J.; Hayden, L.; Hamid, J.S.; Holroyd-Leduc, J.; Twohig, M.; Macfarlane, C.; Hynes, M.T.; Prasaud, L.; Sklar, B.; et al. Effectiveness of an eHealth self-management tool for older adults with multimorbidity (KeepWell): Protocol for a hybrid effectiveness-implementation randomised controlled trial. BMJ Open 2021, 11, 10.e048350. [Google Scholar] [CrossRef]
- Holden, R.J.; Campbell, N.L.; Abebe, E.; Clark, D.O.; Ferguson, D.; Bodke, K.; Boustani, M.A.; Callahan, C.M.; The Brain Health Patient Safety Laboratory. Usability and feasibility of consumer-facing technology to reduce unsafe medication use by older adults. Res. Soc. Adm. Pharm. 2020, 16, 54–61. [Google Scholar] [CrossRef]
- Kuo, M.C.; Chen, C.M.; Wu, F.G.; Chen, C.H.; Yin, Z.X.; Wang, C.Y. Use of photo diary and focus group to explore needs for digital disease management program among community older adults with chronic disease. Health Soc. Care Community 2020, 1–11. [Google Scholar] [CrossRef]
- Rose, K.M.; Gordon, K.C.; Schlegel, E.C.; McCall, M.; Gao, Y.; Ma, M.Y.; Lenger, K.A.; Ko, E.; Wright, K.D.; Wang, H.N.; et al. Smarthealth technology study protocol to improve relationships between older adults with dementia and family caregivers. J. Adv. Nurs. 2021, 77, 2519–2529. [Google Scholar] [CrossRef]
- Puig, J.; Echeverria, P.; Lluch, T.; Herms, J.; Estany, C.; Bonjoch, A.; Ornelas, A.; Paris, D.; Loste, C.; Sarquella, M.; et al. A specific mobile health application for older HIV-infected patients: Usability and patient’s satisfaction. Telemed. J. E-Health 2021, 27, 432–440. [Google Scholar] [CrossRef] [PubMed]
- Cook, D.J.; Moradkhani, A.; Douglas, K.S.V.; Prinsen, S.K.; Fischer, E.N.; Schroeder, D.R. Patient education self-management during surgical recovery: Combining mobile (iPad) and a content management system. Telemed. J. e-Health 2014, 20, 312–317. [Google Scholar] [CrossRef] [Green Version]
- Halcomb, E.; Purcell, R.; Hickman, L.; Smyth, E. Telemonitoring is acceptable amongst community dwelling older Australians with chronic conditions. Collegian 2016, 23, 383–390. [Google Scholar] [CrossRef]
- Kim, H.; Park, E.; Lee, S.; Kim, M.; Park, E.J.; Hong, S. Self-management of chronic diseases among older Korean adults: An mHealth training, protocol, and feasibility study. JMIR Mhealth Uhealth 2018, 6, e147. [Google Scholar] [CrossRef] [Green Version]
- Richardson, J.E.; Lee, J.I.; Nirenberg, A.; Reid, M.C. The potential role for smartphones among older adults with chronic noncancer pain: A qualitative study. Pain Med. 2018, 19, 1132–1139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogonowski, C.; Aal, K.; Vaziri, D.; von Rekowski, T.; Randall, D.; Schreiber, D.; Wieching, R.; Wulf, V. ICT-based fall prevention system for older adults: Qualitative results from a long-term field study. ACM Trans. Comput. Hum. Interact. 2016, 23, 23–33. [Google Scholar] [CrossRef]
- Alkawaldeh, M.Y.; Jacelon, C.S.; Choi, J. Older adults’ experiences with a tablet-based self-management intervention for diabetes mellitus type II: A qualitative study. Geriatr. Nurs. 2020, 41, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Pettersson, B.; Wiklund, M.; Janols, R.; Lindgren, H.; Lundin-Olsson, L.; Skelton, D.A.; Sandlund, M. Managing pieces of a personal puzzle’ Older people’s experiences of self-management falls prevention exercise guided by a digital program or a booklet. BMC Geriatr. 2019, 19, 12. [Google Scholar] [CrossRef]
- Liu, Y.C.; Chen, C.H.; Lin, Y.S.; Chen, H.Y.; Irianti, D.; Jen, T.N.; Yeh, J.Y.; Chiu, S.Y.H. Design and usability evaluation of mobile voice-added food reporting for elderly people: Randomized controlled trial. JMIR Mhealth Uhealth 2020, 8, e20317. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Types (Number of Related Papers) | Specific Techniques | Representative Literature |
|---|---|---|
| Self-monitoring (34) | Medication dispensing device | [8] |
| Embedded sensor | [9,10] | |
| Self-management application | [11,12,13,14] | |
| Online community care platform | [15] | |
| Physical activity tracker | [16] | |
| Wearable systems | [3,17,18,19] | |
| Mobile app | [20] | |
| Medical care (21) | Telemedicine | [21,22] |
| Mobile app | [23,24,25,26,27] | |
| Electronic health record systems | [28,29,30] | |
| Wearable systems | [31] | |
| Physical activity monitors | [32] | |
| Patient Portal | [5,33] | |
| Web-based system | [34] | |
| Remote monitoring (12) | Telemonitoring app | [35] |
| Web-based system | [4] | |
| In-home monitor | [36,37] | |
| Patient Portal | [38] | |
| Embedded sensor | [39] | |
| Robotics | [40] | |
| Health education (5) | Mobile app | [2] |
| Web-based system | [41,42] |
| Influencing Factor | Related Variable | Main Conclusion | Representative Literature |
|---|---|---|---|
| Objective factors | Age | The older the elderly, the worse their performance | [12,28,44,45,46] |
| Education level | Populations with a high education level tend to use new technology | [28,47] | |
| Region | Compared to urban residents, rural ones are not likely to use new technology | [48] | |
| E-health literacy | E-health literacy is considered as a prerequisite of using mobile health app | [5,15,30,47,49] | |
| Information literacy | People skilled in computer and Internet use tend to adopt IHMT | [13,14,38,46] | |
| Ethnicity and language | Ethnic and linguistic differences affect users’ acceptance and use behavior | [13,44] | |
| Physical difficulties | Physical difficulties are an obstacle for the elderly to accept new technologies | [9] | |
| Self-efficacy | People with high efficacy are more willing to accept new technology | [11,13,16,30,39,45,49,50,51] | |
| Compliance | Procedures/equipment that can improve compliance are easy to be continuously used | [19,24,29,52,53,54,55] | |
| Skeptical attitudes | Skepticism is a barrier to the elderly using new technology | [12] | |
| Perceived demand | Perceived demand is an essential factor in promoting the use of intelligent health management devices | [8,21,56] |
| Influencing Factor | Related Variable | Main Conclusion | Representative Literature |
|---|---|---|---|
| Social attributes | Sharing/social network | Social networking increases interest and a sense of achievement and promotes user’s compliance | [57,58,59,60] |
| Source credibility | Recommendation of health care providers | The support of health care providers helps to improve the credibility of the system/equipment | [50,61] |
| Opinions of family/friends | The opinions of family/friends affect users’ acceptance of health information technology | [56] | |
| Service | Encouragement of medical staff | The encouragement of medical staff has played an important role in the use of health information technology by the elderly | [25] |
| Training | The elderly look forward to technical support through training | [2,5,13,14,39,48,60,62] | |
| Cost | Cost | Whether to save operating costs is a central consideration for health care organizations | [10,21,37,63] |
| Influencing Factor | Related Variable | Main Conclusion | Representative Literature |
|---|---|---|---|
| Perceived usefulness | Functionality | Users are interested in core functions such as speed of running, reminders, notifications, encouragement, follow-up, goal setting, and online video presentation, and in the way they are provided | [31,34,64,65,66] |
| Quality of information | Information quality has a significant impact on older people’s acceptance of intelligent health management technologies | [22,67] | |
| Personalization | Personalization is a key characteristic that enhances the attractiveness and acceptability of IHMT | [35,41,68,69,70,71] | |
| Interactivity | Interactive games and healthcare worker or peer interactions can increase interest in older adults | [5,17,26,27,45,58,62,70,71,72] | |
| Perceived ease of use | User interface design | Devices with simple operation, large font, and touch screen interface are more popular | [23,26,42,46,48,68,73,74] |
| Efficiency | Voice input design can improve time efficiency | [75] | |
| Security | Security and privacy | Users’ concern about the security and privacy of health data is one of the reasons they do not use or do not continuously use. | [14,51] |
| Reliability | Fear of misdiagnosis due to unreliability of programs/equipment is one of the main obstacles | [12,50] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Z.; Qi, H.; Wang, L. Study on the Types of Elderly Intelligent Health Management Technology and the Influencing Factors of Its Adoption. Healthcare 2021, 9, 1494. https://doi.org/10.3390/healthcare9111494
Chen Z, Qi H, Wang L. Study on the Types of Elderly Intelligent Health Management Technology and the Influencing Factors of Its Adoption. Healthcare. 2021; 9(11):1494. https://doi.org/10.3390/healthcare9111494
Chicago/Turabian StyleChen, Zhu, Huiying Qi, and Luman Wang. 2021. "Study on the Types of Elderly Intelligent Health Management Technology and the Influencing Factors of Its Adoption" Healthcare 9, no. 11: 1494. https://doi.org/10.3390/healthcare9111494