
Determining Factors for Independent Walking in Patients Undergoing Cardiovascular Surgery: Differences between Coronary Artery Bypass Grafting, Heart Valve Surgery, and Aortic Surgery

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Subjects
2.3. Data Collection
2.4. Early Post-Operative CR Program
2.5. Statistical Analyses
3. Results
3.1. Demographics of Patients
3.2. Post-Operative Progresssion of CR
3.3. Factors Related to Post-Operative Independent Walking
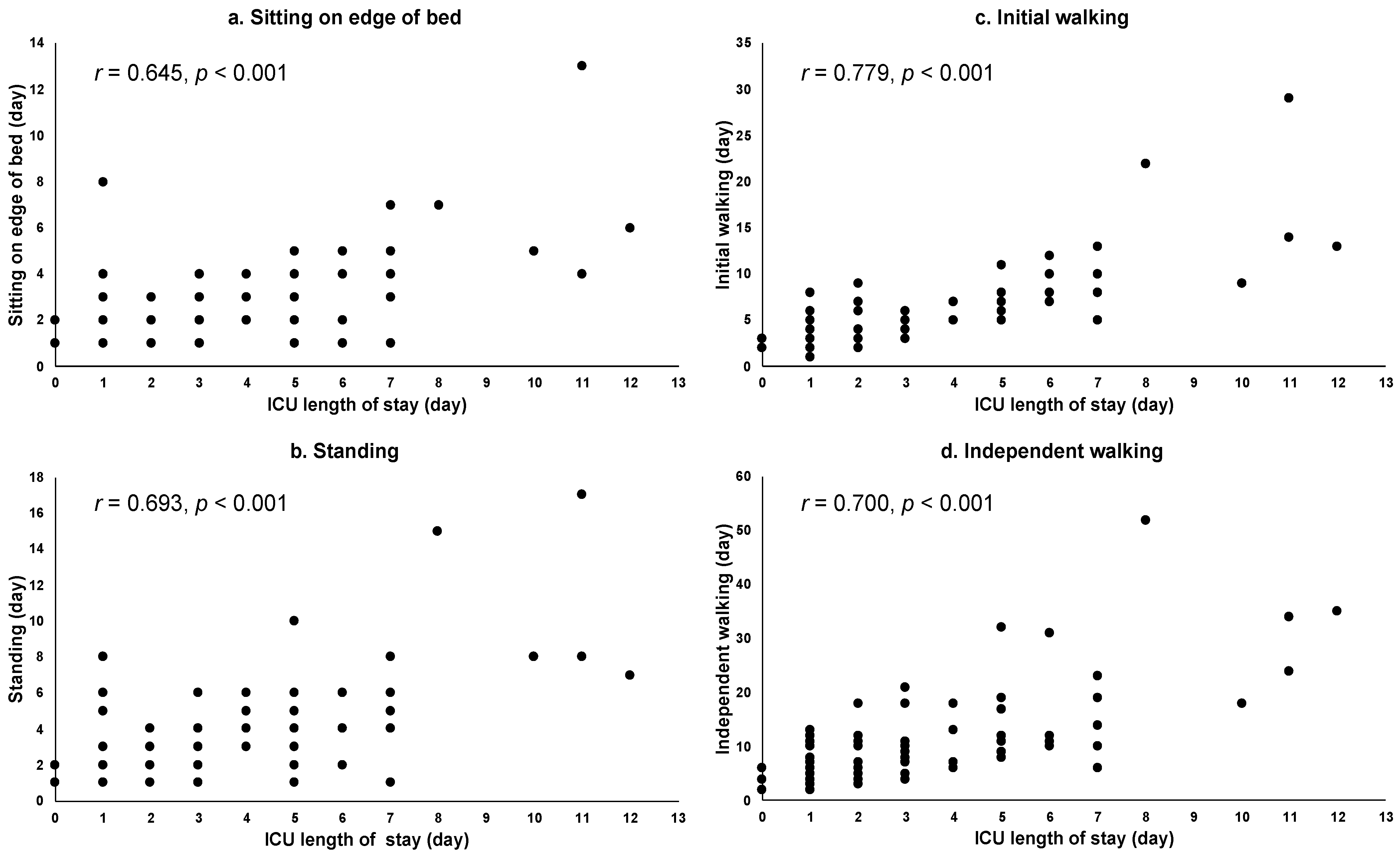
3.4. Relationships between ICU Length of Stay and Progression of CR in the Aortic Surgery Group
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- JCS Joint Working Group Guidelines for Rehabilitation in Patients With Cardiovascular Disease (JCS 2012). Circ. J. 2014, 78, 2022–2093. [CrossRef] [Green Version]
- Cui, Z.; Li, N.; Gao, C.; Fan, Y.; Zhuang, X.; Liu, J.; Zhang, J.; Tan, Q. Precision implementation of early ambulation in elderly patients undergoing off-pump coronary artery bypass graft surgery: A randomized-controlled clinical trial. BMC Geriatr. 2020, 1, 1–10. [Google Scholar] [CrossRef]
- Ohbe, H.; Nakamura, K.; Uda, K.; Matsui, H.; Yasunaga, H. Effect of Early Rehabilitation on Physical Function in Patients Undergoing Coronary Artery Bypass Grafting: A Nationwide Inpatient Database Study. J. Clin. Med. 2021, 10, 618. [Google Scholar] [CrossRef]
- Dong, Z.; Yu, B.; Zhang, Q.; Pei, H.; Xing, J.; Fang, W.; Sun, Y.; Song, Z. Early Rehabilitation Therapy Is Beneficial for Patients With Prolonged Mechanical Ventilation After Coronary Artery Bypass Surgery. Int. Heart J. 2016, 57, 241–246. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, K.; McCarthy, C.P.; McCarthy, K.J.; Brown, C.H.; Needham, D.M.; Januzzi Jr, J.L.; McEvoy, J.W. Delirium in the Cardiac Intensive Care Unit. J. Am. Heart Assoc. 2018, 7, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Shirvani, F.; Naji, S.A.; Davari, E.; Sedighi, M. Early mobilization reduces delirium after coronary artery bypass graft surgery. Asian Cardiovasc. Thorac. Ann. 2020, 28, 566–571. [Google Scholar] [CrossRef]
- Balady, G.J.; Ades, P.A.; Bittner, V.A.; Franklin, B.A.; Gordon, N.F.; Thomas, R.J.; Tomaselli, G.F.; Yancy, C.W. Referral, enrollment, and delivery of cardiac rehabilitation/secondary prevention programs at clinical centers and beyond: A presidential advisory from the American Heart Association. Circulation 2011, 124, 2951–2960. [Google Scholar] [CrossRef] [Green Version]
- Chaddha, A.; Eagle, K.A.; Braverman, A.C.; Kline-Rogers, E.; Hirsch, A.T.; Brook, R.; Jackson, E.A.; Woznicki, E.M.; Housholder-Hughes, S.; Pitler, L.; et al. Exercise and Physical Activity for the Post-Aortic Dissection Patient: The Clinician’s Conundrum. Clin. Cardiol. 2015, 38, 647–651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dylewicz, P.; Bienkowska, S.; Szczesniak, L.; Rychlewski, T.; Przywarska, I.; Wilk, M.; Jastrzebski, A. Beneficial effect of short-term endurance training on glucose metabolism during rehabilitation after coronary bypass surgery. Chest 2000, 117, 47–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hedbäck, B.E.; Perk, J.; Engvall, J.; Areskog, N.H. Cardiac rehabilitation after coronary artery bypass grafting: Effects on exercise performance and risk factors. Arch. Phys. Med. Rehabil. 1990, 71, 1069–1073. [Google Scholar]
- Engblom, E.; Korpilahti, K.; Hämäläinen, H.; Rönnemaa, T.; Puukka, P. Quality of life and return to work 5 years after coronary artery bypass surgery. Long-term results of cardiac rehabilitation. J. Cardiopulm. Rehabil. 1997, 17, 29–36. [Google Scholar] [CrossRef] [PubMed]
- JCS/JSCVS/JATS/JSVS 2020 Guideline on Diagnosis and Treatment of Aortic Aneurysm and Aortic Dissection. Circ. J. 2020. Available online: https://www.j-circ.or.jp/cms/wp-content/uploads/2020/07/JCS2020_Ogino.pdf (accessed on 20 October 2021). (In Japanese).
- Chaddha, A.; Kline-Rogers, E.; Woznicki, E.M.; Brook, R.; Housholder-Hughes, S.; Braverman, A.C.; Pitler, L.; Hirsch, A.T.; Eagle, K.A. Activity recommendations for postaortic dissection patients. Circulation 2014, 130, e140–e142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franklin, B.A.; Brinks, J.; Sacks, R.; Trivax, J.; Friedman, H. Reduced walking speed and distance as harbingers of the approaching grim reaper. Am. J. Cardiol. 2015, 116, 313–317. [Google Scholar] [CrossRef] [PubMed]
- Lo, A.X.; Donnelly, J.P.; McGwin, G., Jr.; Bittner, V.; Ahmed, A.; Brown, C.J. Impact of gait speed and instrumental activities of daily living on all-cause mortality in adults ≥65 years with heart failure. Am. J. Cardiol. 2015, 115, 797–801. [Google Scholar] [CrossRef] [Green Version]
- Saitoh, M.; Takahashi, T.; Sakurada, K.; Kumamaru, M.; Hanafusa, Y.; Iwatsu, K.; Tahara, M.; Oura, K.; Yuguchi, S.; Morisawa, T. Factors determining achievement of early postoperative cardiac rehabilitation goal in patients with or without preoperative kidney dysfunction undergoing isolated cardiac surgery. J. Cardiol. 2013, 61, 299–303. [Google Scholar] [CrossRef] [Green Version]
- Kato, M.; Saitoh, M.; Kawamura, T.; Iwata, K.; Sakurada, K.; Okamura, D.; Tahara, M.; Yuguchi, S.; Kamisaka, K.; Oura, K.; et al. Postoperative atrial fibrillation is associated with delayed early rehabilitation after heart valve surgery: A multicenter study. Phys. Ther. Res. 2019, 22, 1–8. [Google Scholar] [CrossRef]
- Iida, Y.; Yamazaki, T.; Kawabe, T.; Usui, A.; Yamada, S. Postoperative muscle proteolysis affects systemic muscle weakness in patients undergoing cardiac surgery. Int. J. Cardiol. 2014, 172, 595–597. [Google Scholar] [CrossRef]
- Hirsch, C.H.; Sommers, L.; Olsen, A.; Mullen, L.; Winograd, C.H. The natural history of functional morbidity in hospitalized older patients. J. Am. Geriatr. Soc. 1990, 38, 1296–1303. [Google Scholar] [CrossRef]
- Monteleone, S.; Dalla Toffola, E.; Emiliani, V.; Ricotti, S.; Bruggi, M.; Conte, T.; D’Armini, A.M.; Orlandoni, G.; Petrucci, L. Recovery of deambulation after cardiothoracic surgery: A single center experience. Eur. J. Phys. Rehabil. Med. 2015, 51, 763–771. [Google Scholar]
- Shimizu, H.; Okada, M.; Tangoku, A.; Doki, Y.; Endo, S.; Fukuda, H.; Hirata, Y.; Iwata, H.; Kobayashi, J.; Kumamaru, H.; et al. Thoracic and cardiovascular surgeries in Japan during 2017: Annual report by the Japanese Association for Thoracic Surgery. Gen. Thorac. Cardiovasc. Surg. 2020, 68, 414–449. [Google Scholar] [CrossRef] [Green Version]
- Khan, F.M.; Naik, A.; Hameed, I.; Robinson, N.B.; Spadaccio, C.; Rahouma, M.; Yongle, R.; Demetres, M.; Chen, H.; Chang, M.; et al. Open Repair of Descending Thoracic and Thoracoabdominal Aortic Aneurysms: A Meta-Analysis. Ann. Thorac. Surg. 2020, 110, 1941–1949. [Google Scholar] [CrossRef]
- Xu, S.; Liu, J.; Li, L.; Wu, Z.; Li, J.; Liu, Y.; Zhu, J.; Sun, L.; Guan, X.; Gong, M.; et al. Cardiopulmonary bypass time is an independent risk factor for acute kidney injury in emergent thoracic aortic surgery: A retrospective cohort study. J. Cardiothorac. Surg. 2019, 14, 90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buth, J.; Harris, P.L.; Hobo, R.; van Eps, R.; Cuypers, P.; Duijm, L.; Tielbeek, X. Neurologic complications associated with endovascular repair of thoracic aortic pathology: Incidence and risk factors. a study from the European Collaborators on Stent/Graft Techniques for Aortic Aneurysm Repair (EUROSTAR) registry. J. Vasc. Surg. 2007, 46, 1103–1110; discussion 1110–1111. [Google Scholar] [CrossRef] [Green Version]
- Chiesa, R.; Tshomba, Y.; Civilini, E.; Marone, E.M.; Bertoglio, L.; Baccellieri, D.; Coppi, G.; Logaldo, D.; Melissano, G. Open repair of descending thoracic aneurysms. HSR Proc. Intensive Care Cardiovasc. Anesth. 2010, 2, 177–190. [Google Scholar] [PubMed]
- Takashima, N.; Ohkubo, T.; Miura, K.; Okamura, T.; Murakami, Y.; Fujiyoshi, A.; Nagasawa, S.Y.; Kadota, A.; Kita, Y.; Miyagawa, N.; et al. Long-term risk of BP values above normal for cardiovascular mortality: A 24-year observation of Japanese aged 30 to 92 years. J. Hypertens. 2012, 30, 2299–2306. [Google Scholar] [CrossRef] [PubMed]
- Seino, Y.; Nanjo, K.; Tajima, N.; Kadowaki, T.; Kashiwagi, A.; Araki, E.; Ito, C.; Inagaki, N.; Iwamoto, Y.; Kasuga, M.; et al. Report of the committee on the classification and diagnostic criteria of diabetes mellitus. J. Diabetes Investig. 2010, 1, 212–228. [Google Scholar] [CrossRef] [Green Version]
- Fliser, D.; Laville, M.; Covic, A.; Fouque, D.; Vanholder, R.; Juillard, L.; Van Biesen, W. A European Renal Best Practice (ERBP) position statement on the Kidney Disease Improving Global Outcomes (KDIGO) clinical practice guidelines on acute kidney injury: Part 1: Definitions, conservative management and contrast-induced nephropathy. Nephrol. Dial. Transplant. 2012, 27, 4263–4272. [Google Scholar] [CrossRef] [Green Version]
- Edition, F. Diagnostic and statistical manual of mental disorders. Am. Psychiatric. Assoc. 2013, 21, 591–643. [Google Scholar]
- Canet, J.; Gallart, L.; Gomar, C.; Paluzie, G.; Valles, J.; Castillo, J.; Sabate, S.; Mazo, V.; Briones, Z.; Sanchis, J. Prediction of postoperative pulmonary complications in a population-based surgical cohort. Anesthesiology 2010, 113, 1338–1350. [Google Scholar] [CrossRef]
- Bailey, M.L.; Richter, S.M.; Mullany, D.V.; Tesar, P.J.; Fraser, J.F. Risk factors and survival in patients with respiratory failure after cardiac operations. Ann. Thorac. Surg. 2011, 92, 1573–1579. [Google Scholar] [CrossRef]
- Leditschke, I.A.; Green, M.; Irvine, J.; Bissett, B.; Mitchell, I.A. What are the barriers to mobilizing intensive care patients? Cardiopulm. Phys. Ther. J. 2012, 23, 26–29. [Google Scholar] [CrossRef] [PubMed]
- Tabuchi, Y.; Morimoto, Y.; Yano, Y.; Tawara, Y.; Sato, S.; Tanigawa, K.; Eishi, K.; Kozu, R. Risk Factors for Post-operative Respiratory Failure and Respiratory Tract Infections Following Cardiovascular Surgery. Kyobu Geka 2017, 70, 1051–1062. (In Japanese) [Google Scholar] [PubMed]
- Waite, I.; Deshpande, R.; Baghai, M.; Massey, T.; Wendler, O.; Greenwood, S. Home-based preoperative rehabilitation (prehab) to improve physical function and reduce hospital length of stay for frail patients undergoing coronary artery bypass graft and valve surgery. J. Cardiothorac. Surg. 2017, 12, 91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steinmetz, C.; Bjarnason-Wehrens, B.; Baumgarten, H.; Walther, T.; Mengden, T.; Walther, C. Prehabilitation in patients awaiting elective coronary artery bypass graft surgery - effects on functional capacity and quality of life: A randomized controlled trial. Clin. Rehabil. 2020, 34, 1256–1267. [Google Scholar] [CrossRef]
- Golaghaie, F.; Esmaeili-Kalantari, S.; Sarzaeem, M.; Rafiei, F. Adherence to lifestyle changes after coronary artery bypass graft: Outcome of preoperative peer education. Patient Educ. Couns. 2019, 102, 2231–2237. [Google Scholar] [CrossRef]
- Erbel, R.; Aboyans, V.; Boileau, C.; Bossone, E.; Bartolomeo, R.D.; Eggebrecht, H.; Evangelista, A.; Falk, V.; Frank, H.; Gaemperli, O.; et al. 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: Document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC). Eur. Heart J. 2014, 35, 2873–2926. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Variables | CABG Group (n = 153) | Heart Valve Surgery Group (n = 312) | Aortic Surgery Group (n = 102) | p Value a | |||
|---|---|---|---|---|---|---|---|
| Age, year | 69.0 [63.0–77.5] | 70.0 [60.0–77.0] | 69.0 [58.0–78.0] | 0.205 | |||
| Male, n (%) | 115 (75.2) | 155 (49.7) | ††† | 67 (65.7) | ‡ | <0.001 | |
| BMI, kg/m2 | 23.8 [21.6–26.5] | * | 22.4 [20.2–24.7] | ††† | 23.2 [20.7–24.8] | <0.001 | |
| NYHA functional classification, n (%) | |||||||
| I/II/III/IV/Unknown | 43 (28.1)/45 (29.4)/39 (25.5)/24 (15.7)/2 (1.3) | 72 (23.1)/109 (34.9)/93 (29.8)/36 (11.5)/2 (0.6) | 53 (52.0)/20 (19.6)/10 (9.8)/4 (3.9)/15 (14.7) | ‡‡‡ | <0.001 | ||
| LVEF, % | 65.5 [54.8–72.3] | 66.0 [58.0–72.0] | 66.0 [59.0–70.0] | 0.700 | |||
| E/e’, cm/s | 10.6 [8.0–13.7] | 14.3 [10.6–20.4] | ††† | 9.0 [7.6–12.5] | ‡‡‡ | <0.001 | |
| Comorbidities, n (%) | |||||||
| Hypertension | 90 (58.8) | 133 (42.6) | †† | 64 (62.7) | ‡‡ | <0.001 | |
| Diabetes | 62 (40.5) | *** | 55 (17.6) | ††† | 7 (6.9) | ‡ | <0.001 |
| Renal disease | 28 (18.3) | 66 (21.2) | 11 (10.8) | 0.058 | |||
| Respiratory disease | 25 (16.3) | 59 (18.9) | 14 (13.7) | 0.471 | |||
| Central nervous system disease | 28 (18.3) | 32 (10.3) | † | 10 (9.8) | 0.040 | ||
| Operative time, min | 304.0 [248.5–340.5] | *** | 257.5 [221.5–294.8] | ††† | 381.0 [321.8–457.0] | ‡‡‡ | <0.001 |
| Amount of bleeding, mL | 1010.0 [500.0–1649.5] | *** | 1230.0 [545.5–1800.0] | 2290.0 [980.0–3495.0] | ‡‡‡ | <0.001 | |
| Aortic cross clumping time, min | 0.0 [0–74.5] | *** | 80.0 [68.0–108.0] | ††† | 135.0 [102.3–169.5] | ‡‡‡ | <0.001 |
| Cardiopulmonary bypass time, min | 72.0 [0–119] | *** | 135.0 [111.0–166.0] | ††† | 207.0 [161.8–246.5] | ‡‡‡ | <0.001 |
| Emergency surgery, n (%) | 22 (14.4) | *** | 5 (1.6) | ††† | 50 (49.0) | ‡‡‡ | <0.001 |
| Length of intensive care unit stay, day | 1.0 [1.0–2.0] | *** | 1.0 [0–2.0] | 2.0 [1.0–5.0] | ‡‡‡ | <0.001 | |
| Duration of mechanical ventilatory support, hour | 11.8 [8.6–17.9] | *** | 9.6 [7.4–14.9] | ††† | 18.8 [11.8–25.1] | ‡‡‡ | <0.001 |
| Post-operative complications, n (%) | 62 (40.52) | *** | 116 (37.2) | 71 (69.6) | ‡‡‡ | <0.001 | |
| Cardiovascular | 13 (8.6) | 40 (12.8) | 10 (9.8) | 0.372 | |||
| Acute kidney injury | 2 (1.3) | 9 (2.9) | 7 (6.9) | 0.052 | |||
| Delirium | 11 (7.2) | 20 (6.4) | 13 (12.7) | 0.135 | |||
| Respiratory | 50 (32.7) | *** | 79 (25.3) | 67 (65.7) | ‡‡‡ | <0.001 | |
| Cardiac rehabilitation progress | |||||||
| Sitting on the edge of a bed, day | 1.0 [1.0–2.0] | *** | 1.0 [1.0–1.0] | 2.0 [1.0–3.0] | ‡‡‡ | <0.001 | |
| Standing, day | 1.0 [1.0–2.0] | *** | 1.0 [1.0–2.0] | 2.0 [1.0–4.0] | ‡‡‡ | <0.001 | |
| Initial walking, day | 3.0 [2.0–4.0] | *** | 2.0 [2.0–4.0] | †† | 4.0 [3.0–6.3] | ‡‡‡ | <0.001 |
| Independent walking, day | 5.0 [4.0–7.0] | *** | 5.0 [3.0–6.0] | † | 8.0 [5.0–12.0] | ‡‡‡ | <0.001 |
| Length of stay in hospital, day | 18.0 [15.0–21.0] | *** | 18.0 [15.0–24.0] | 23.5 [19.0–30.0] | ‡‡‡ | <0.001 | |
| CABG Group (n = 153) | Heart Valve Surgery Group (n = 312) | Aortic Surgery Group (n = 102) | ||||
|---|---|---|---|---|---|---|
| β [95%CI] | p Value | β [95%CI] | p Value | β [95%CI] | p Value | |
| Age, year | 0.109 [0.046–0.173] | <0.001 | 0.074 [0.019–0.128] | 0.009 | 0.023 [−0.101–0.147] | 0.714 |
| Male (presence) | −0.138 [−0.941–0.665] | 0.735 | −0.453 [−1.202–0.296] | 0.235 | −0.021 [−1.751–1.709] | 0.981 |
| BMI, kg/m2 | −0.217 [−0.414–0.020] | 0.031 | −0.209 [−0.431–0.012] | 0.064 | −0.314 [−0.170–0.797] | 0.201 |
| NYHA functional classification, class | 0.501 [−0.158–1.160] | 0.135 | 1.467 [0.692–2.243] | <0.001 | −0.184 [−1.933–1.565] | 0.835 |
| LVEF, % | −0.021 [−0.079–0.038] | 0.486 | −0.075 [−0.131–0.019] | 0.008 | 0.098 [−0.082–0.278] | 0.098 |
| E/e’, cm/s | 0.205 [0.039–0.370] | 0.016 | 0.063 [−0.019–0.144] | 0.130 | 0.301 [−0.149–0.752] | 0.187 |
| Comorbidity (presence) | ||||||
| Hypertension | −0.260 [−0.964–0.444] | 0.466 | −0.465 [−1.222–0.291] | 0.227 | 0.791 [−0.889–2.471] | 0.352 |
| Diabetes | 0.201 [−0.506–0.907] | 0.576 | 0.044 [−0.941–1.028] | 0.930 | −1.215 [−4.425–1.995] | 0.454 |
| Renal disease | 1.615 [0.756–2.475] | <0.001 | 2.279 [1.396–3.161] | <0.001 | 2.433 [−0.146–5.012] | 0.064 |
| Respiratory disease | 1.014 [0.089–1.939] | 0.032 | 1.365 [0.419–2.310] | 0.001 | 1.035 [−1.397–3.468] | 0.400 |
| Central nervous system disease | 0.719 [0.171–1.610] | 0.113 | 0.086 [−1.151–1.322] | 0.892 | 1.321 [−1.403–4.046] | 0.334 |
| Operative time, min | 0.006 [−0.004–0.016] | 0.215 | 0.012 [0.001–0.022] | 0.025 | 0.031 [0.020–0.041] | <0.001 |
| Amount of bleeding, mL | 0.001 [8.377–0.002] | 0.048 | 0.001 [−0.001–0.001] | 0.584 | 0.001 [0.001–0.001] | <0.001 |
| Aortic cross clumping time, min | 0.008 [−0.009–0.024] | 0.364 | 0.020 [−0.002–0.042] | 0.074 | 0.036 [0.007–0.065] | 0.017 |
| Cardiopulmonary bypass time, min | 0.001 [−0.003–0.019] | 0.158 | 0.005 [−0.008–0.018] | 0.436 | 0.024 [0.005–0.043] | 0.014 |
| Emergency surgery (presence) | 2.069 [1.137–3.000] | <0.001 | 0.739 [−2.247–3.725] | 0.627 | 1.490 [−0.118–3.098] | 0.069 |
| Length of intensive care unit stay, day | 1.428 [1.136–1.713] | <0.001 | 2.137 [1.958–2.316] | <0.001 | 2.261 [1.801–2.721] | <0.001 |
| Duration of mechanical ventilatory support, hour | 0.047 [0.018–0.076] | 0.002 | 0.152 [0.135–0.168] | <0.001 | 0.182 [0.071–0.293] | 0.001 |
| Post-operative complications (presence) | ||||||
| Cardiovascular | 1.318 [0.087–2.548] | 0.036 | 2.698 [1.617–3.779] | <0.001 | 3.375 [0.722–6.028] | 0.013 |
| Acute kidney injury | 1.265 [−1.784–4.314] | 0.414 | 2.282 [0.055–4.508] | 0.045 | 7.534 [4.688–10.381] | <0.001 |
| Delirium | 1.394 [0.069–2.719] | 0.039 | 2.834 [1.335–4.332] | <0.001 | 3.154 [0.796–5.513] | 0.009 |
| Respiratory | 2.107 [1.449–2.765] | <0.001 | 2.785 [1.981–3.590] | <0.001 | 2.671 [1.037–4.304] | 0.002 |
| Types of surgery (presence) | ||||||
| Off-pump CABG | −0.507 [−1.198–0.183] | 0.148 | ||||
| MICS | −1.338 [−2.094–−0.581] | <0.001 |
| CABG Group (n = 153) | Heart Valve Surgery Group (n = 312) | Aortic Surgery Group (n = 102) | ||||
|---|---|---|---|---|---|---|
| R2 = 0.499, p < 0.001 | R2 = 0.698, p < 0.001 | R2 = 0.606, p < 0.001 | ||||
| β [95%CI] | p Value | β [95%CI] | p Value | β [95%CI] | p Value | |
| Age, year | 0.057 [0.002–0.111] | 0.041 | −0.005 [−0.039–0.029] | 0.776 | ||
| BMI, kg/m2 | −0.064 [−0.221–0.093] | 0.421 | ||||
| NYHA functional classification, class | 0.803 [0.355–1.251] | <0.001 | ||||
| E/e’, cm/s | 0.119 [−0.015–0.252] | 0.082 | ||||
| Comorbidity (presence) | ||||||
| Renal disease | 0.898 [0.177–1.619] | 0.015 | 0.688 [0.139–1.238] | 0.014 | ||
| Respiratory disease | 0.327 [−0.367–1.021] | 0.354 | 0.547 [0.013–1.080] | 0.045 | ||
| Operative time, min | −0.001 [−0.007–0.006] | 0.913 | 0.016 [−0.001–0.032] | 0.061 | ||
| Amount of bleeding, mL | 0.001 [−0.001–0.001] | 0.234 | 0.022 [−0.037–0.081] | 0.458 | ||
| Aortic cross clumping time, min | −0.008 [−0.050–0.034] | 0.712 | ||||
| Cardiopulmonary bypass time, min | −0.006 [−0.034–0.023] | 0.681 | ||||
| Emergency surgery (presence) | 0.942 [−0.160–2.043] | 0.093 | ||||
| Length of intensive care unit stay, day | 0.863 [0.499–1.226] | <0.001 | 1.326 [1.003–1.649] | <0.001 | 1.503 [0.947–2.058] | <0.001 |
| Duration of mechanical ventilatory support, hour | 0.010 [−0.014–0.033] | 0.426 | 0.054 [0.031–0.078] | <0.001 | −0.010 [−0.122–0.101] | 0.858 |
| Post-operative complications (presence) | ||||||
| Cardiovascular complications | 0.663 [−0.385–1.711] | 0.213 | 0.835 [−0.192–1.479] | 0.011 | 1.682 [−0.226–3.589] | 0.083 |
| Acute kidney injury | −0.453 [−1.761–0.855] | 0.496 | 3.062 [0.451–5.673] | 0.022 | ||
| Delirium | 0.155 [−0.903–1.214] | 0.772 | 0.588 [−0.317–1.494] | 0.202 | 1.052 [−0.770–2.874] | 0.254 |
| Respiratory complications | 0.911 [0.269–1.555] | 0.006 | 0.841 [0.303–1.378] | 0.002 | 0.187 [−1.060–1.434] | 0.767 |
| Types of surgery (presence) | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sakamoto, Y.; Morimoto, Y.; Hanada, M.; Yano, Y.; Sawai, T.; Miura, T.; Eishi, K.; Kozu, R. Determining Factors for Independent Walking in Patients Undergoing Cardiovascular Surgery: Differences between Coronary Artery Bypass Grafting, Heart Valve Surgery, and Aortic Surgery. Healthcare 2021, 9, 1475. https://doi.org/10.3390/healthcare9111475
Sakamoto Y, Morimoto Y, Hanada M, Yano Y, Sawai T, Miura T, Eishi K, Kozu R. Determining Factors for Independent Walking in Patients Undergoing Cardiovascular Surgery: Differences between Coronary Artery Bypass Grafting, Heart Valve Surgery, and Aortic Surgery. Healthcare. 2021; 9(11):1475. https://doi.org/10.3390/healthcare9111475
Chicago/Turabian StyleSakamoto, Yui, Yosuke Morimoto, Masatoshi Hanada, Yudai Yano, Terumitsu Sawai, Takashi Miura, Kiyoyuki Eishi, and Ryo Kozu. 2021. "Determining Factors for Independent Walking in Patients Undergoing Cardiovascular Surgery: Differences between Coronary Artery Bypass Grafting, Heart Valve Surgery, and Aortic Surgery" Healthcare 9, no. 11: 1475. https://doi.org/10.3390/healthcare9111475