
Knowledge Retention of the NIH Stroke Scale among Stroke Unit Health Care Workers Using Video vs. E-Learning: Protocol for a Web-Based, Randomized Controlled Trial

 , , and
, , and
Abstract
:1. Introduction
1.1. Background
1.2. Objectives
2. Materials and Methods
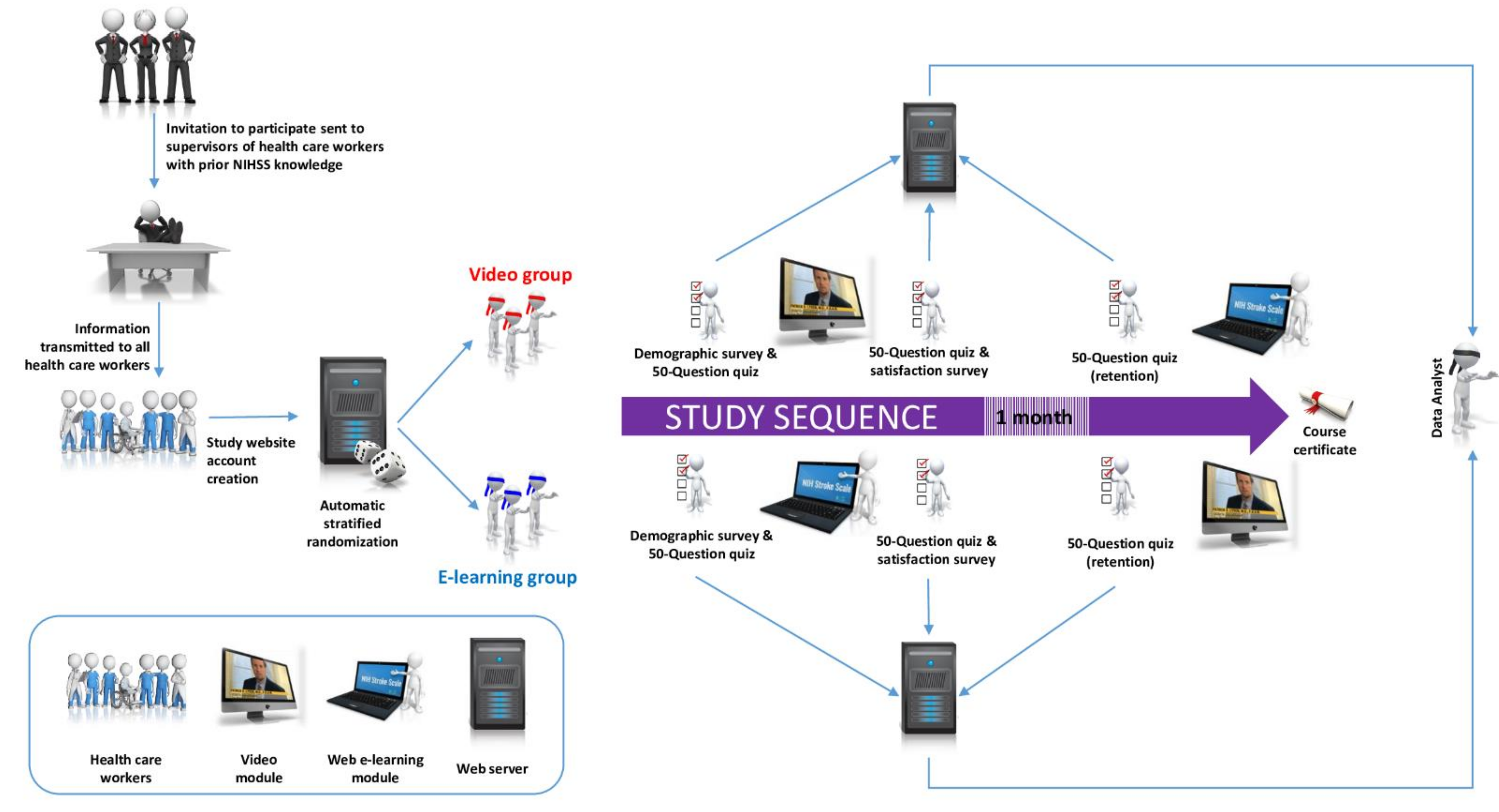
2.1. Study Design and Setting
2.2. Online Platform
2.3. First Questionnaire
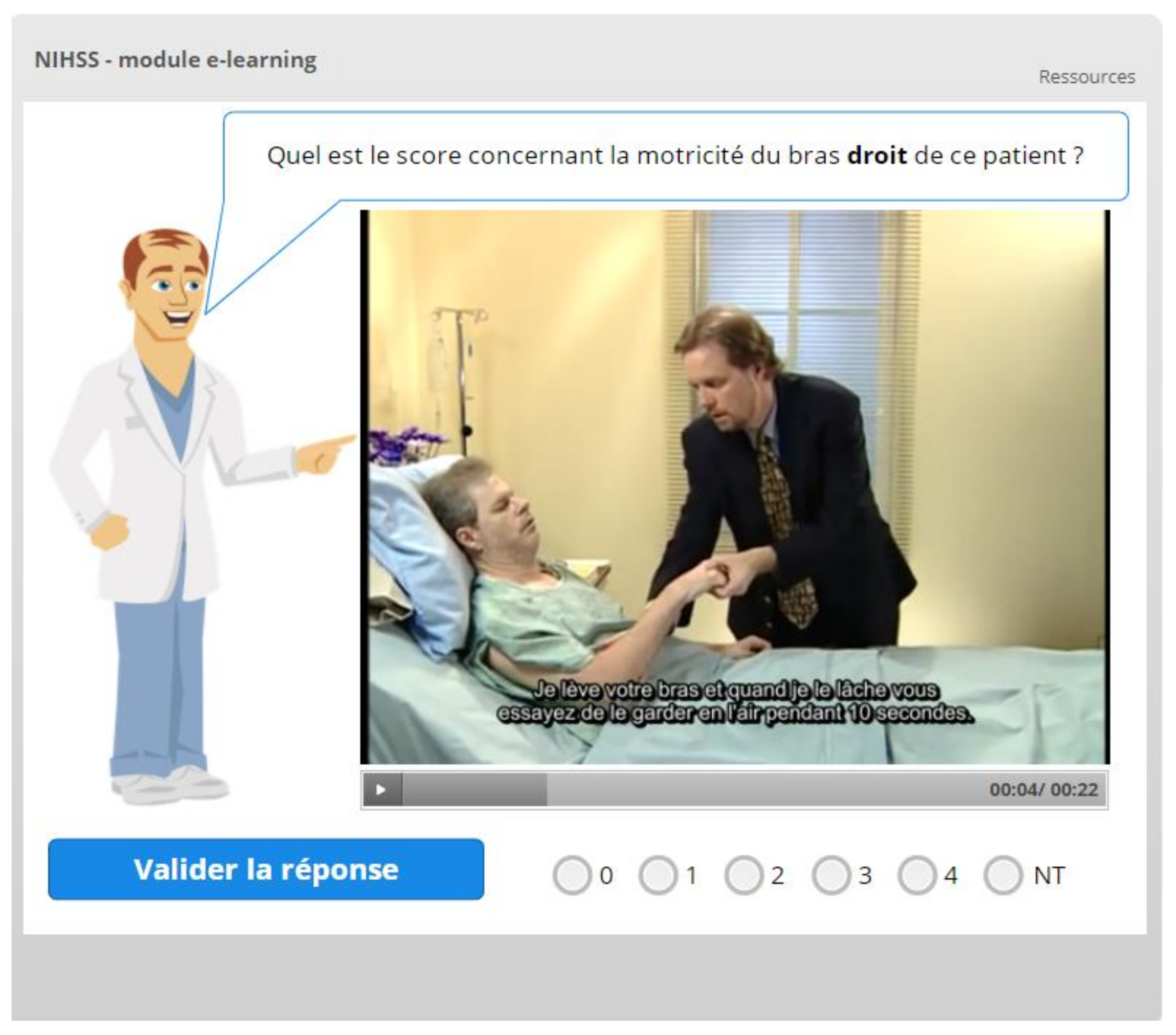
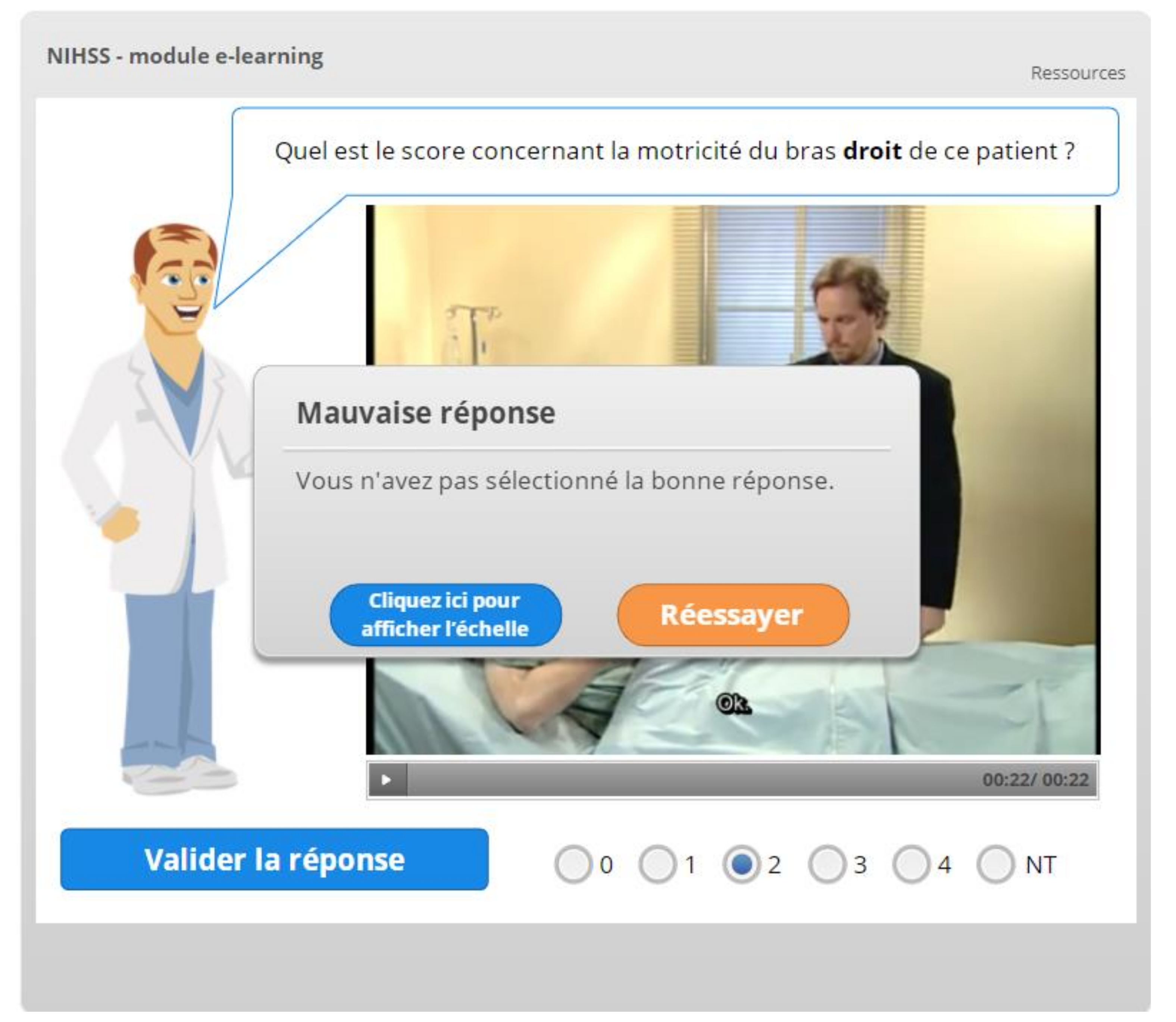
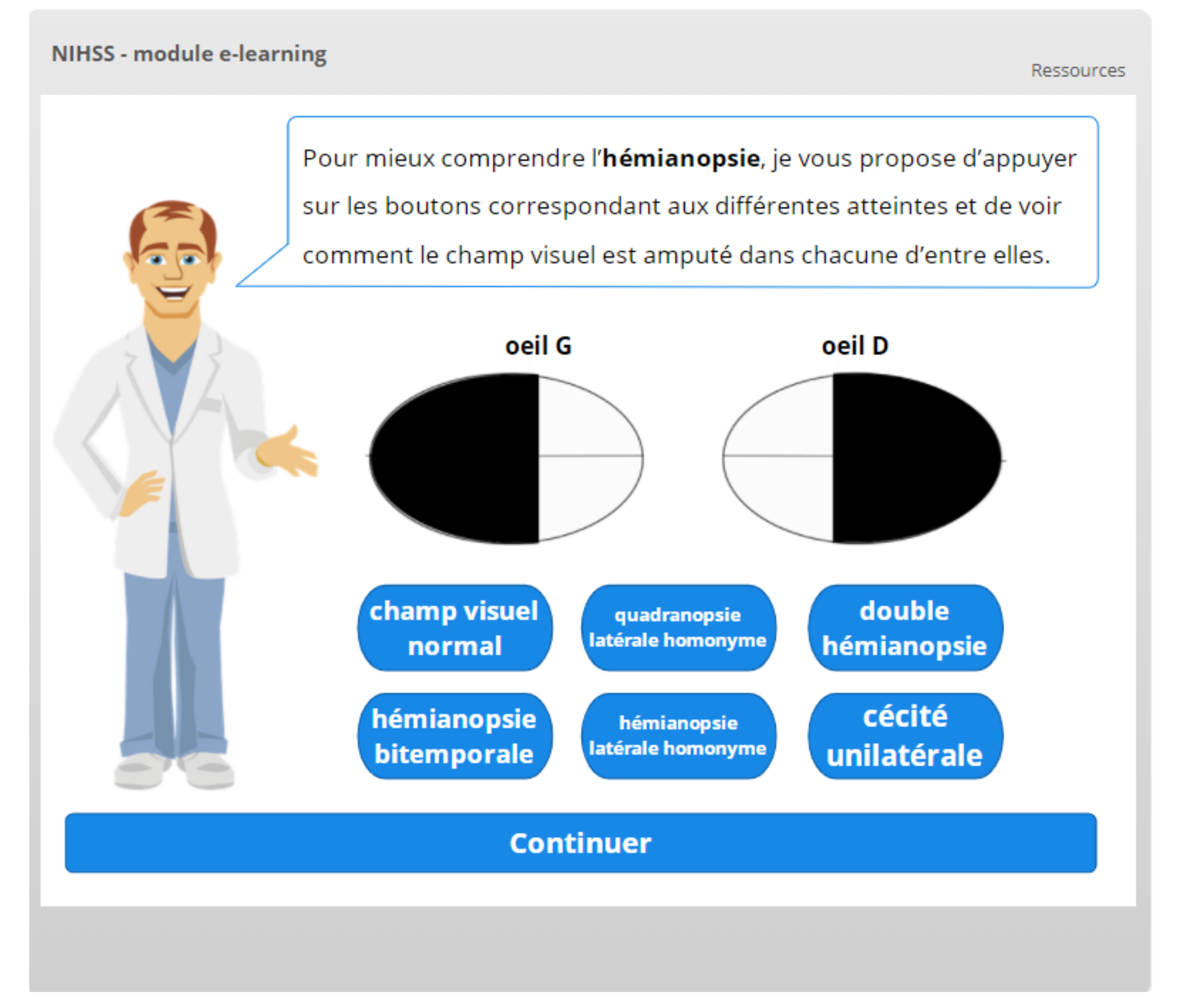
2.4. Learning Material
2.5. Knowledge Retention
2.6. Outcomes
2.7. Participants and Sample Size
2.8. Data Curation and Statistical Analysis
2.9. Ethical Considerations
3. Discussion
3.1. Main Considerations
3.2. Strengths and Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. 2018 Guidelines for the Early Management of Patients With Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2018, 49, e46–e110. [Google Scholar] [CrossRef]
- Katan, M.; Luft, A. Global Burden of Stroke. Semin. Neurol. 2018, 38, 208–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feigin, V.L.; Stark, B.A.; Johnson, C.O.; Roth, G.A.; Bisignano, C.; Abady, G.G.; Abbasifard, M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abedi, V.; et al. Global, regional, and national burden of stroke and its risk factors, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021, 20, 795–820. [Google Scholar] [CrossRef]
- Ntaios, G.; Michel, P.; Georgiopoulos, G.; Guo, Y.; Li, W.; Xiong, J.; Calleja, P.; Ostos, F.; González-Ortega, G.; Fuentes, B.; et al. Characteristics and Outcomes in Patients With COVID-19 and Acute Ischemic Stroke. Stroke 2020, 51, e254–e258. [Google Scholar] [CrossRef]
- Mowla, A.; Doyle, J.; Lail, N.S.; Rajabzadeh-Oghaz, H.; Deline, C.; Shirania, P.; Ching, M.; Crumlish, A.; Steck, D.A.; Janicke, D.; et al. Delays in door-to-needle time for acute ischemic stroke in the emergency department: A comprehensive stroke center experience. J. Neurol. Sci. 2017, 376, 102–105. [Google Scholar] [CrossRef]
- Perotte, R.; Lewin, G.O.; Tambe, U.; Galorenzo, J.B.; Vawdrey, D.K.; Akala, O.O.; Makkar, J.S.; Lin, D.J.; Mainieri, L.; Chang, B.C. Improving Emergency Department Flow: Reducing Turnaround Time for Emergent CT Scans. AMIA Annu. Symp. Proc. 2018, 2018, 897–906. [Google Scholar]
- Wardlaw, J.M.; Seymour, J.; Cairns, J.; Keir, S.; Lewis, S.; Sandercock, P. Immediate Computed Tomography Scanning of Acute Stroke Is Cost-Effective and Improves Quality of Life. Stroke 2004, 35, 2477–2483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lyden, P. Using the National Institutes of Health Stroke Scale. Stroke 2017, 48, 513–519. [Google Scholar] [CrossRef]
- Eskioglou, E.; Huchmandzadeh Millotte, M.; Amiguet, M.; Michel, P. National Institutes of Health Stroke Scale Zero Strokes. Stroke 2018, 49, 3057–3059. [Google Scholar] [CrossRef]
- Bill, O.; Zufferey, P.; Faouzi, M.; Michel, P. Severe stroke: Patient profile and predictors of favorable outcome. J. Thromb. Haemost. 2013, 11, 92–99. [Google Scholar] [CrossRef]
- Delgado, M.G.; Michel, P.; Naves, M.; Maeder, P.; Reichhart, M.; Wintermark, M.; Bogousslavsky, J. Early profiles of clinical evolution after intravenous thrombolysis in an unselected stroke population. J. Neurol. Neurosurg. Psychiatry 2010, 81, 282–285. [Google Scholar] [CrossRef] [PubMed]
- Wee, C.-K.; McAuliffe, W.; Phatouros, C.C.; Phillips, T.J.; Blacker, D.; Singh, T.P.; Baker, E.; Hankey, G.J. Outcomes of Endovascular Thrombectomy with and without Thrombolysis for Acute Large Artery Ischaemic Stroke at a Tertiary Stroke Centre. Cerebrovasc. Dis. Extra 2017, 7, 95–102. [Google Scholar] [CrossRef] [PubMed]
- CHOP 2021 MG. Traitement Neurologique Complexe de l’AVC Aigu en Stroke Unit (SU), Selon la Durée de Traitement en Heures. Available online: https://medcode.ch/ch/fr/chops/CHOP%202021/99.BA.2 (accessed on 14 June 2021).
- Josephson, S.A.; Hills, N.K.; Johnston, S.C. NIH Stroke Scale Reliability in Ratings from a Large Sample of Clinicians. Cerebrovasc. Dis. 2006, 22, 389–395. [Google Scholar] [CrossRef]
- Scott, K.; Morris, A.; Marais, B. Medical student use of digital learning resources. Clin. Teach. 2018, 15, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.-J.; Kim, G. Development of e-learning in medical education: 10 years’ experience of Korean medical schools. Korean J. Med. Educ. 2019, 31, 205–214. [Google Scholar] [CrossRef] [Green Version]
- Rouleau, G.; Gagnon, M.-P.; Côté, J.; Payne-Gagnon, J.; Hudson, E.; Dubois, C.-A.; Bouix-Picasso, J. Effects of E-Learning in a Continuing Education Context on Nursing Care: Systematic Review of Systematic Qualitative, Quantitative, and Mixed-Studies Reviews. J. Med. Internet Res. 2019, 21, e15118. [Google Scholar] [CrossRef] [Green Version]
- Koka, A.; Suppan, L.; Cottet, P.; Carrera, E.; Stuby, L.; Suppan, M. Teaching NIHSS to Paramedics, E-learning vs Video: A Randomized Controlled Trial (Preprint). J. Med. Internet Res. 2020, 22, e18358. [Google Scholar] [CrossRef] [PubMed]
- Suppan, M.; Stuby, L.; Carrera, E.; Cottet, P.; Koka, A.; Assal, F.; Savoldelli, G.L.; Suppan, L. Asynchronous Distance Learning of the National Institutes of Health Stroke Scale During the COVID-19 Pandemic (E-Learning vs Video): Randomized Controlled Trial. J. Med. Internet Res. 2021, 23, e23594. [Google Scholar] [CrossRef]
- Lyden, P.; Brott, T.; Tilley, B.; Welch, K.M.; Mascha, E.J.; Levine, S.; Haley, E.C.; Grotta, J.; Marler, J. Improved reliability of the NIH Stroke Scale using video training. NINDS TPA Stroke Study Group. Stroke 1994, 25, 2220–2226. [Google Scholar] [CrossRef] [Green Version]
- Lyden, P. NIH Stroke Scale Training—Part 2—Basic Instruction. Available online: https://www.youtube.com/watch?v=gzHuNvDhVwE (accessed on 14 June 2021).
- Bochenska, K.; Milad, M.P.; DeLancey, J.O.; Lewicky-Gaupp, C. Instructional Video and Medical Student Surgical Knot-Tying Proficiency: Randomized Controlled Trial. JMIR Med. Educ. 2018, 4, e9. [Google Scholar] [CrossRef] [Green Version]
- Wade, S.W.T.; Moscova, M.; Tedla, N.; Moses, D.A.; Young, N.; Kyaw, M.; Velan, G.M. Adaptive Tutorials Versus Web-Based Resources in Radiology: A Mixed Methods Analysis of Efficacy and Engagement in Senior Medical Students. Acad. Radiol. 2019, 26, 1421–1431. [Google Scholar] [CrossRef]
- Croxton, R.A. The Role of Interactivity in Student Satisfaction and Persistence in Online Learning. J. Online Learn. Teach. 2014, 10, 314–325. [Google Scholar]
- Eysenbach, G. CONSORT-EHEALTH Group CONSORT-EHEALTH: Improving and standardizing evaluation reports of Web-based and mobile health interventions. J. Med. Internet Res. 2011, 13, e126. [Google Scholar] [CrossRef]
- Eysenbach, G. Improving the quality of Web surveys: The Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J. Med. Internet Res. 2004, 6, e34. [Google Scholar] [CrossRef] [PubMed]
- Open Source Matters Joomla Content Management System. Available online: https://www.joomla.org/ (accessed on 30 September 2020).
- Gegabyte Technology. Random Article. Available online: https://www.gegabyte.org/downloads/joomla-extensions/joomla3/modules/291-random-article (accessed on 30 September 2020).
- Joomdonation Membership Pro. Available online: https://joomdonation.com/joomla-extensions/membership-pro-joomla-membership-subscription.html (accessed on 30 September 2020).
- Corejoomla Community Surveys Pro. Available online: https://www.corejoomla.com/products/community-surveys.html (accessed on 30 September 2020).
- Suppan, M.; Stuby, L.; Koka, A.; Suppan, L. NIHSS Video Subtitled in French. Available online: https://nihss-study.ch/video (accessed on 30 September 2021).
- Stuby, L.; Suppan, L.; Koka, A.; Suppan, M. NIHSS—e-Learning Module in French. Available online: https://nihss-study.ch/nihss-e-learning/21c/story_html5.html (accessed on 30 September 2021).
- Kopp, V.; Stark, R.; Fischer, M.R. Fostering diagnostic knowledge through computer-supported, case-based worked examples: Effects of erroneous examples and feedback. Med. Educ. 2008, 42, 823–829. [Google Scholar] [CrossRef] [PubMed]
- Latimier, A.; Riegert, A.; Peyre, H.; Ly, S.T.; Casati, R.; Ramus, F. Does pre-testing promote better retention than post-testing? Npj Sci. Learn. 2019, 4, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Stuby, L.; Currat, L.; Gartner, B.; Mayoraz, M.; Harbarth, S.; Suppan, L.; Suppan, M. Impact of face-to-face teaching in addition to electronic learning on personal protective equipment doffing proficiency in student paramedics: Protocol for a randomized controlled trial. JMIR Res. Protoc. 2021, 10, e26927. [Google Scholar] [CrossRef] [PubMed]
- Kamuche, F.U.; Ledman, R.E. Relationship of Time and Learning Retention. J. Coll. Teach. Learn. 2005, 2, 25. [Google Scholar] [CrossRef] [Green Version]
- Kirchberg, J.; Fritzmann, J.; Weitz, J.; Bork, U. eHealth Literacy of German Physicians in the Pre–COVID-19 Era: Questionnaire Study. JMIR mHealth uHealth 2020, 8, e20099. [Google Scholar] [CrossRef] [PubMed]
- Zou, X.; Liu, S.; Li, J.; Chen, W.; Ye, J.; Yang, Y.; Zhou, F.; Ling, L. Factors Associated With Healthcare Workers’ Insomnia Symptoms and Fatigue in the Fight Against COVID-19, and the Role of Organizational Support. Front. Psychiatry 2021, 12, 652717. [Google Scholar] [CrossRef]
- Eysenbach, G. The law of attrition. J. Med. Internet Res. 2005, 7, e11. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Page | Field | Original Question | English Translation |
|---|---|---|---|
| 1 | Demographics | Age | Age a |
| Genre | Gender b | ||
| Années d’expérience clinique au total | Number of years of total clinical experience a | ||
| Années d’expérience clinique dans un service de neurologie et/ou de neurochirurgie | Number of years of clinical experience in a neurology and/or neurosurgery ward a | ||
| Maîtrise du Français | French proficiency c | ||
| Maîtrise de l’Anglais | English proficiency c | ||
Dans quel service travaillez-vous principalement:
| In which ward do you most frequently work: b
| ||
| 2 | Prior NIHSS knowledge | Avez-vous effectué une formation interne du service pour apprendre à faire une évaluation NIHSS? | Have you completed an in house NIHSS training? b |
| Avez-vous complété une formation certifiante officielle NIHSS? | Have you completed the official NIHSS certification course? b | ||
| Nombre d’années de pratique avec l’échelle NIHSS | Number of years of clinical experience with the NIHSS scale a | ||
Fréquence d’application du NIHSS:
| NIHSS use frequency: b
| ||
| Je me sens à l’aise par rapport à l’application du NIHSS | I feel comfortable using the NIHSS c |
| Page | Field | Original Question | English Translation |
|---|---|---|---|
| 1 | Prior NIHSS learning method exposition | Aviez-vous déjà suivi cette méthode de formation au NIHSS? | Had you already been exposed to this NIHSS learning method in the past? a |
Quand avez-vous suivi cette formation?
| When did you undergo this training?
| ||
| Current training-context | Dans quel cadre avez-vous suivi cette formation?
| In which context did you undergo this training?
| |
| Current training-satisfaction | Comment évaluez-vous le niveau de difficulté global de cette formation? | How would you access the overall difficulty level of this training? b | |
| Que pensez-vous de la durée de cette méthode de formation? | What do you think about the duration of this training? b | ||
| Quel est votre niveau de satisfaction concernant la méthode de formation? | What is your level of satisfaction regarding the learning method? b | ||
| Recommanderiez-vous cette méthode de formation à vos collègues? | Would you recommend this training method to your colleagues? b | ||
| Avez-vous des commentaires supplémentaires? | Do you have any additional comments? |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koka, A.; Suppan, M.; Carrera, E.; Fraga-Freijeiro, P.; Massuk, K.; Imbeault, M.-E.; Missilier Perruzzo, N.; Achab, S.; Salerno, A.; Strambo, D.; et al. Knowledge Retention of the NIH Stroke Scale among Stroke Unit Health Care Workers Using Video vs. E-Learning: Protocol for a Web-Based, Randomized Controlled Trial. Healthcare 2021, 9, 1460. https://doi.org/10.3390/healthcare9111460
Koka A, Suppan M, Carrera E, Fraga-Freijeiro P, Massuk K, Imbeault M-E, Missilier Perruzzo N, Achab S, Salerno A, Strambo D, et al. Knowledge Retention of the NIH Stroke Scale among Stroke Unit Health Care Workers Using Video vs. E-Learning: Protocol for a Web-Based, Randomized Controlled Trial. Healthcare. 2021; 9(11):1460. https://doi.org/10.3390/healthcare9111460
Chicago/Turabian StyleKoka, Avinash, Mélanie Suppan, Emmanuel Carrera, Paula Fraga-Freijeiro, Kiril Massuk, Marie-Eve Imbeault, Nathalie Missilier Perruzzo, Sophia Achab, Alexander Salerno, Davide Strambo, and et al. 2021. "Knowledge Retention of the NIH Stroke Scale among Stroke Unit Health Care Workers Using Video vs. E-Learning: Protocol for a Web-Based, Randomized Controlled Trial" Healthcare 9, no. 11: 1460. https://doi.org/10.3390/healthcare9111460