
Adult Granulosa Cell Tumor in Pregnancy: A New Case and a Review of the Literature

 , and
, and
Abstract
:1. Introduction
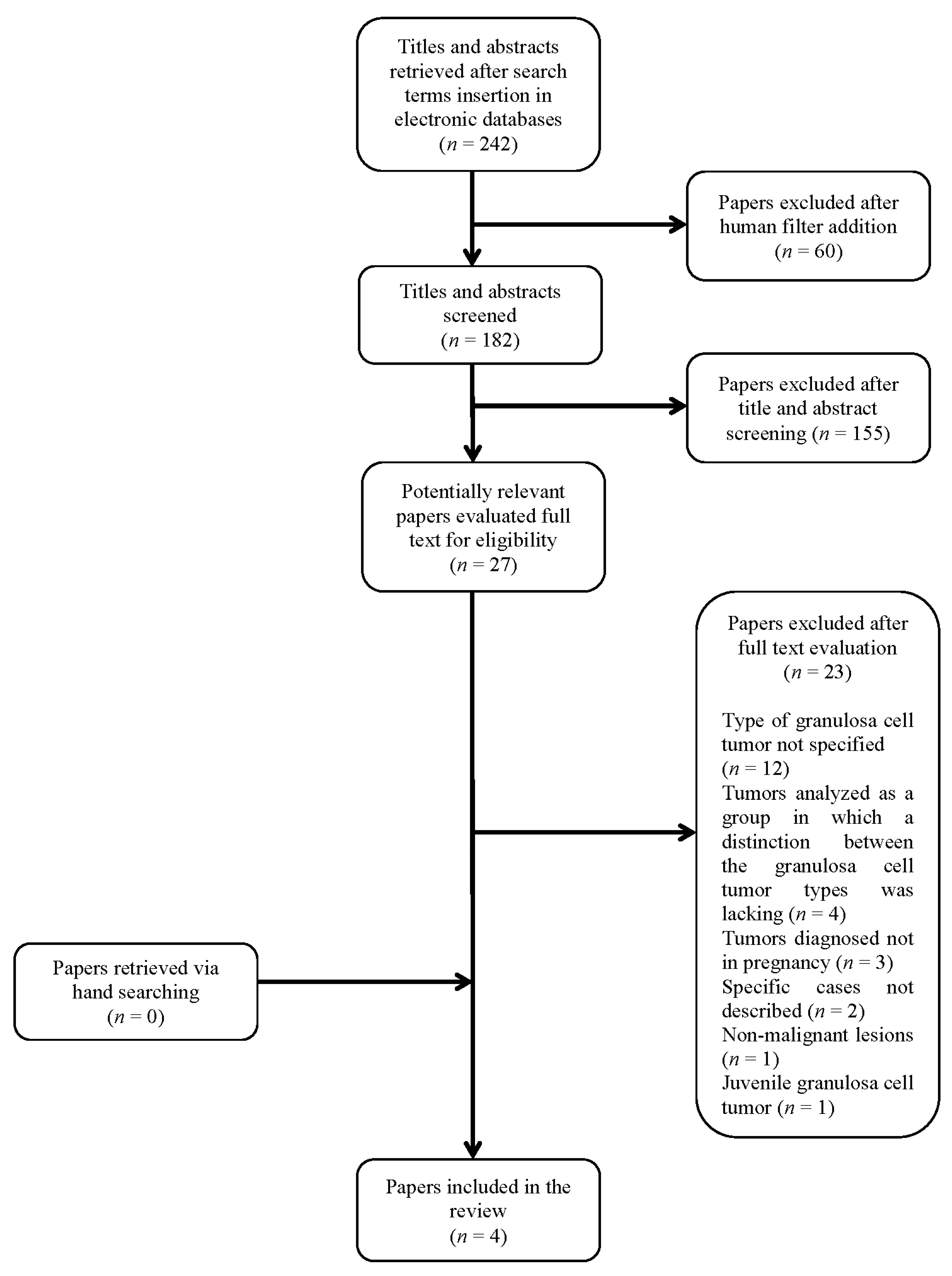
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Levin, G.; Zignon, R.; Haj-Yahya, R.; Matan, L.S.; Rottenstreich, A. Granulosa cell tumor of ovary: A systematic review of recent evidence. Eur. J. Obstet. Gynecol. Reprod. Biol. 2018, 225, 57–61. [Google Scholar] [CrossRef] [PubMed]
- Hasiakos, D.; Papakonstantinou, K.; Goula, K.; Karvouni, E.; Fotiou, S. Juvenile granulosa cell tumor associated with pregnancy: Report of a case and review of the literature. Gynecol. Oncol. 2006, 100, 426–429. [Google Scholar] [CrossRef] [PubMed]
- Mangili, G.; Ottolina, J.; Gadducci, A.; Giorda, G.; Breda, E.; Savarese, A.; Candiani, M.; Frigerio, L.; Scarfone, G.; Pignata, S.; et al. Long-term follow-up is crucial after treatment for granulosa cell tumours of the ovary. Br. J. Cancer 2013, 109, 29–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakr, S.; Abdulfatah, E.; Thomas, S.; Al-Wahab, Z.; Beydoun, R.; Morris, R.; Ali-Fehmi, R.; Bandyopadhyay, S. Granulosa cell tumors: Novel predictors of recurrence in early-stage patients. Int. J. Gynecol. Pathol. 2017, 36, 240. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Cid, M.; Pascual, M.A.; Graupera, B.; Hereter, L.; Cusidó, M.T.; Tresserra, F.; Rotili, A. Adult granulosa cell tumour of the ovary associated with pregnancy. J. Obstet. Gynaecol. 2011, 31, 272. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, R.; Radhakrishnan, G.; Radhika, A.G.; Jain, J.; Sharma, S.; Srivastava, H. Pregnancy concomitant with metastatic adult granulosa cell tumor. Arch. Gynecol. Obstet. 2011, 284, 743. [Google Scholar] [CrossRef] [PubMed]
- Roy, J.; Babu, A.S. Granulosa Cell Tumor of the Ovary—An Incidental Finding during Caesarean Section–A Rare Case Report. Kathmandu Univ. Med. J. 2014, 45, 60. [Google Scholar] [CrossRef] [Green Version]
- Aymen, F.M.; Majed, G.; Hanene, C.; Joumana, L.; Amin, B. Advanced Granulosa Cell Tumor and Pregnancy: A Case Report, How to Treat and How to Preserve Fertility? Endocrinol. Metab. Syndr. 2016, 5. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| First Author | Year | Patient Age | Gravidity and Parity | Primary/Recurrent | Previous Oncological Surgeries before Pregnancy |
|---|---|---|---|---|---|
| Guidi | 2019 | 41 | G5P1122 | Recurrent | Laparoscopic enucleation of an ovarian cyst on the right ovary initially, then right salpingo-oophorectomy, lymph nodes sampling, and omental and peritoneal biopsies |
| Aymen | 2016 | 30 | G1P0 | Primary | NS |
| Roy | 2014 | 23 | G1P0 | Primary | NS |
| Agarwal | 2011 | 26 | G1P0 | Recurrent | Right salpingo-oophorectomy |
| Fernandez-cid | 2011 | 35 | NS | Primary | NS |
| First Author | Symptoms/Signs in the Index Pregnancy Which Prompted Work-Up | Week at Radiologic Work-Up or Intraoperative Diagnosis | Radiologic Work Up | Tumor Localization | Tumor Dimension |
|---|---|---|---|---|---|
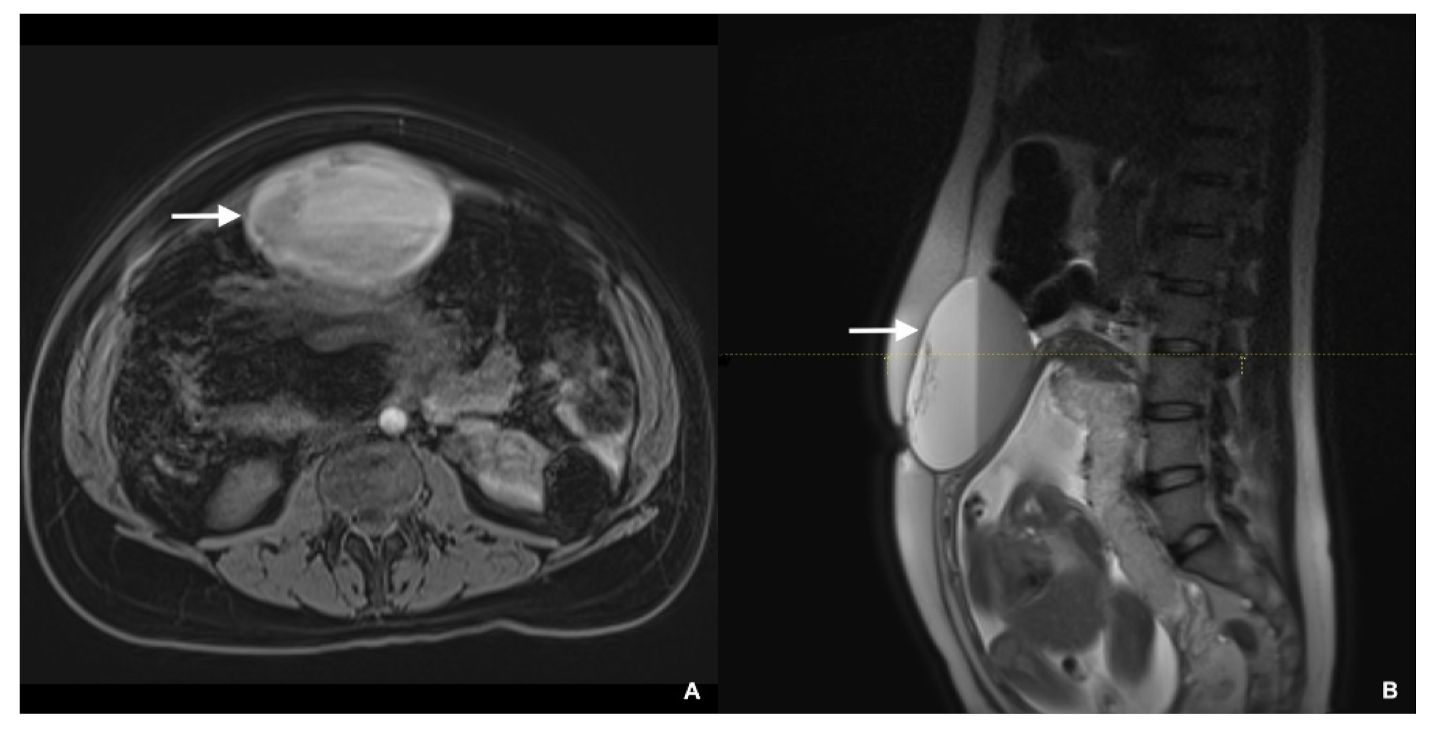
| Guidi | Bulging of a symptomatic abdominal mass, that was palpable and visible | 29 | US and MRI | Uterine fundus | 9.6 × 6.7 × 12 cm3 (MRI) |
| Aymen | Intermittent abdominal unspecific pain | 32 (CD) | NS | Right ovary | 40 × 30 cm (intraoperative) |
| Roy | NS | At term (CD) | NS | Right ovary | 10 × 10 × 5 cm (intraoperative) |
| Agarwal | Acute pain and progressive abdominal distension | 20 | US and MRI | Left ovary | 9.7 × 7.7 cm (US-MRI) |
| Fernandez-cid | Asymptomatic; tumor detected at routine abdominal ultrasound | NS | US | Left ovary | 17 × 14.1 × 11.8 cm (US) |
| First Author | Week at Surgery | Surgery in Pregnancy | Surgery at Delivery | Intraoperative Findings and Sites Positive for AGCT | Chemotherapy during Pregnancy |
|---|---|---|---|---|---|
| Guidi | 36 + 3 | No | Total hysterectomy, left salpingo-oophorectomy, excision of every macroscopically visible nodules in the peritoneum, and infracolic omentectomy | Left ovary, bilaterally in uterosacral ligaments, vesico-uterine fold and douglas pouch. | No |
| Aymen | 32 | No | Right adnexectomy and partial omental removing | Omentum | No |
| Roy | At term | No | Right sided ovariectomy | NS | NS |
| Agarwal | Not applicable | No | No | Significant ascites, peritoneal implants, omental thickening, enlarged paraaortic lymph nodes and bilateral pleural effusion. | Adriamycin–Vincristine (week 21) |
| Fernandez-cid | 15 | Laparoscopic left adnexectomy | No | NS | NS |
| First Author | Gestational Age Delivery (Weeks + Days) | Mode of Delivery | Pregnancy Outcome | Birth Weight (Grams) | Apgars at 1 and 5 min |
|---|---|---|---|---|---|
| Guidi | 36 + 3 | Planned cesarean done early for preterm labor | Live birth, female | 2750 | 9/9 |
| Aymen | 32 | Emergency cesarean for placental abruption | Live birth | 1925 | 2/5 * |
| Roy | At term | Emergency cesarean for labor obstruction | Live birth, male | 2500 | NS |
| Agarwal | 30 | Vaginal after preterm labor | Live birth, male | 1200 | NS |
| Fernandez-cid | 39 | Planned cesarean | Live birth, female | NS | NS |
| First Author | Surgery after Pregnancy | Chemotherapy after Pregnancy | Maternal Oncologic Outcome |
|---|---|---|---|
| Guidi | No | Six cycles of Carboplatin | Follow-up at 26 months negative for recurrence |
| Aymen | Total hysterectomy, left adnexectomy, total omentectomy, appendicectomy, and multiple peritoneal biopsies | Four cycles of BEP protocol (after surgery in pregnancy) | Follow-up at 18-months negative for recurrence |
| Roy | NS | Yes (type not described) | NS |
| Agarwal | Total abdominal hysterectomy and left salpingo-oophorectomy (After the chemotherapy and 8 months postpartum) | Six cycles of cisplatin regimen | Follow-up at 10 months after delivery negative for recurrence |
| Fernandez-cid | No | NS | Asymptomatic and at last US no recurrences |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guidi, S.; Berghella, V.; Scambia, G.; Fagotti, A.; Vidiri, A.; Restaino, S.; Vizzielli, G.; Inzani, F.; Cavaliere, A.F. Adult Granulosa Cell Tumor in Pregnancy: A New Case and a Review of the Literature. Healthcare 2021, 9, 1455. https://doi.org/10.3390/healthcare9111455
Guidi S, Berghella V, Scambia G, Fagotti A, Vidiri A, Restaino S, Vizzielli G, Inzani F, Cavaliere AF. Adult Granulosa Cell Tumor in Pregnancy: A New Case and a Review of the Literature. Healthcare. 2021; 9(11):1455. https://doi.org/10.3390/healthcare9111455
Chicago/Turabian StyleGuidi, Sofia, Vincenzo Berghella, Giovanni Scambia, Anna Fagotti, Annalisa Vidiri, Stefano Restaino, Giuseppe Vizzielli, Frediano Inzani, and Anna Franca Cavaliere. 2021. "Adult Granulosa Cell Tumor in Pregnancy: A New Case and a Review of the Literature" Healthcare 9, no. 11: 1455. https://doi.org/10.3390/healthcare9111455