
Cost and Effectiveness of Long-Term Care Following Integrated Discharge Planning: A Prospective Cohort Study

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
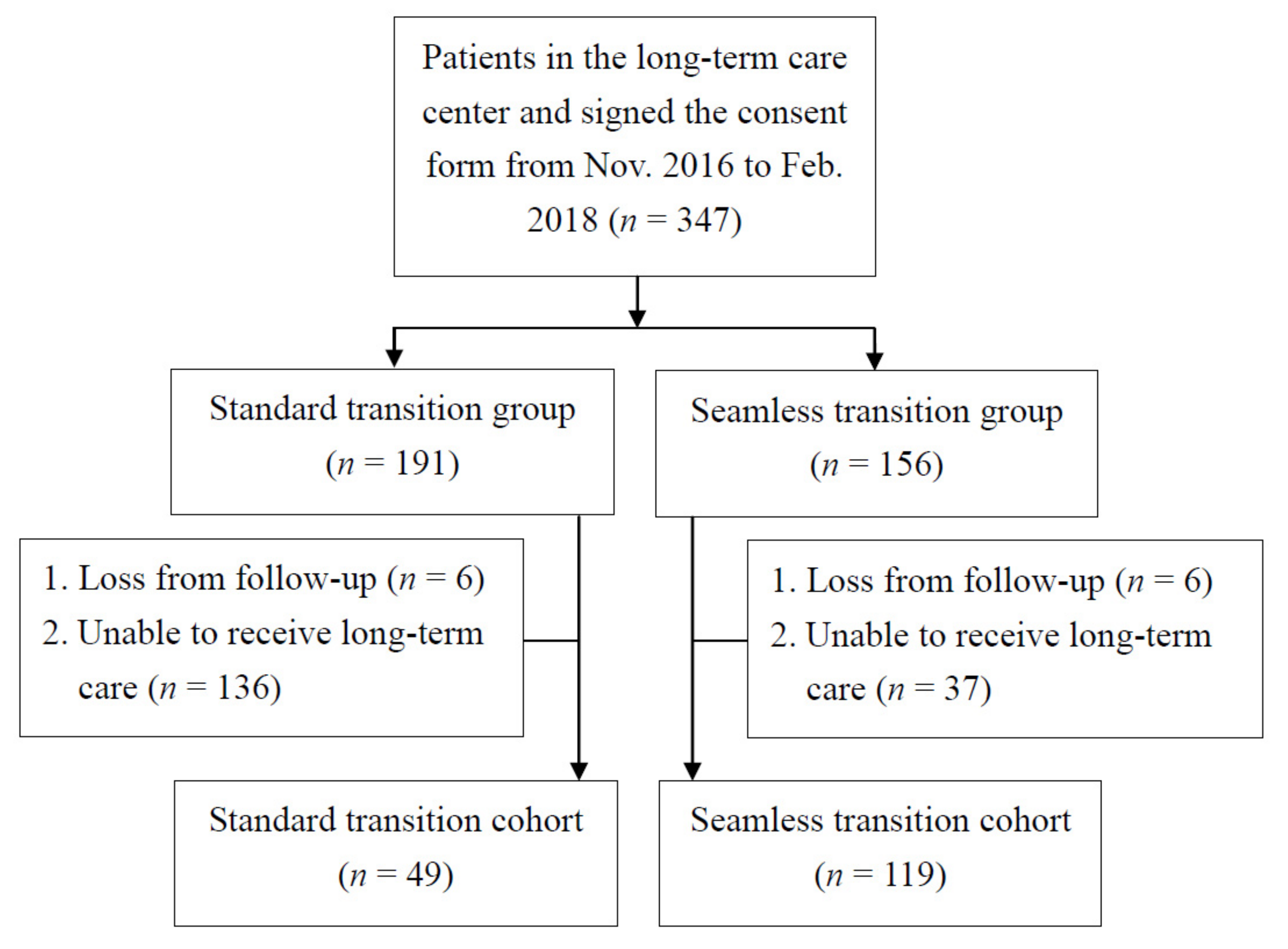
2.1. Study Design and Participants
2.2. Study Measures
2.2.1. Multimorbidity Frailty Index (MFI)
2.2.2. Activities of Daily Living (ADL)
2.2.3. Malnutrition Universal Screening Tool (MUST)
2.2.4. Medical Record Review
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD 2019 Demographics Collaborators. Global age-sex-specific fertility, mortality, healthy life expectancy (HALE), and population estimates in 204 countries and territories, 1950–2019: A comprehensive demographic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1160–1203. [Google Scholar] [CrossRef]
- Bindman, A.B.; Blum, J.D.; Kronick, R. Medicare’s transitional care payment—a step toward the medical home. N. Engl. J. Med. 2013, 368, 692–694. [Google Scholar] [CrossRef] [Green Version]
- Bindman, A.B.; Cox, D.F. Changes in Health Care Costs and Mortality Associated With Transitional Care Management Services after a Discharge among Medicare Beneficiaries. JAMA Intern. Med. 2018, 178, 1165–1171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naylor, M.; Brooten, D.; Campbell, R.; Jacobsen, B.S.; Mezey, M.D.; Pauly, M.V.; Schwartz, J.S. Comprehensive discharge planning and home follow-up of hospitalized elders—A randomized clinical trial. JAMA 1999, 281, 613–662. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forster, A.J.; Clark, H.D.; Menard, A.; Dupuis, N.; Chernish, R.; Chandok, N.; Khan, A.; Letourneau, M.; van Walraven, C. Effect of a nurse team coordinator on outcomes for hospitalized medicine patients. Am. J. Med. 2005, 118, 1148–1153. [Google Scholar] [CrossRef]
- Jack, B.W.; Chetty, V.K.; Anthony, D.; Greenwald, J.L.; Sanchez, G.M.; Johnson, A.E.; Forsythe, S.R.; O’Donnell, J.K.; Paasche-Orlow, M.K.; Manasseh, C.; et al. A reengineered hospital discharge program to decrease rehospitalization: A randomized trial. Ann. Intern. Med. 2009, 150, 178–187. [Google Scholar] [CrossRef]
- Shepperd, S.; McClaran, J.; Phillips, C.O.; Lannin, N.A.; Clemson, L.M.; McCluskey, A.; Cameron, I.D.; Barras, S.L. Discharge planning from hospital to home. Cochrane Database Syst. Rev. 2010, CD000313. [Google Scholar] [CrossRef]
- Preyde, M.; Macaulay, C.; Dingwall, T. Discharge planning from hospital to home for elderly patients: A meta-analysis. J. Evid. Based Soc. Work 2009, 6, 198–216. [Google Scholar] [CrossRef]
- Coleman, E.A.; Boult, C. Improving the quality of transitional care for persons with complex care needs. J. Am. Geriatr. Soc. 2003, 1, 556–557. [Google Scholar] [CrossRef]
- Hoyer, E.H.; Young, D.L.; Friedman, L.A.; Brotman, D.J.; Klein, L.M.; Friedman, M.; Needham, D.M. Routine Inpatient Mobility Assessment and Hospital Discharge Planning. JAMA Intern. Med. 2019, 179, 118–120. [Google Scholar] [CrossRef]
- Department of Long-Term Care, Ministry of Health and Welfare: Promotion of Long-Term Care for Ten Years Plan 2.0. Available online: https://1966.gov.tw/LTC/cp-4001-42414-201.html (accessed on 9 July 2019).
- Groenendaal, M.; Loor, A.; Trouw, M.; Achterberg, W.P.; Caljouw, M.A.A. Perspectives of Healthcare Professionals on Meaningful Activities for Persons with Dementia in Transition from Home to a Nursing Home: An Explorative Study. Healthcare 2019, 7, 98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Godin, J.; Theou, O.; Black, K.; McNeil, S.A.; Andrew, M.K. Long-Term Care Admissions Following Hospitalization: The Role of Social Vulnerability. Healthcare 2019, 7, 91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.C.; Lu, Y.P.; Wang, J.H.; Liang, C.K.; Chou, M.Y.; Lin, Y.T.; Chen, F.T.; Lin, M.L.; Lee, S.H.; Huang, J.J. The Effectiveness of a Timely Discharge Plan in Older Adults: A Prospective HospitalBased Cohort Study in Southern Taiwan. Aging Med. Healthc. 2019, 10, 104–108. [Google Scholar] [CrossRef]
- Wen, Y.C.; Chen, L.K.; Hsiao, F. Predicting mortality and hospitalization of older adults by the multimorbidity frailty indexY. PLoS ONE 2017, 12, e0187825. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoogendijk, E.O.; Afilalo, J.; Ensrud, K.E.; Kowal, P.; Onder, G.; Fried, L.P. Frailty: Implications for clinical practice and public health. Lancet 2019, 394, 1365–1375. [Google Scholar] [CrossRef]
- Katz, S.; Ford, A.B.; Moskowitz, R.W.; Jackson, B.A.; Jaffe, M.W. Studies of illness in the aged. The index of ADL: A standardized measure of biological and psychosocial function. JAMA 1963, 185, 914–919. [Google Scholar] [CrossRef]
- Katz, S. Assessing self-maintenance: Activities of daily living, mobility and instrumental activities of daily living. J. Am. Geriatr. Soc. 1983, 31, 721–727. [Google Scholar] [CrossRef]
- Axmon, A.; Ekstam, L.; Slaug, B.; Schmidt, S.M.; Fange, A.M. Detecting longitudinal changes in activities of daily living (ADL) dependence: Optimizing ADL staircase response choices. Br. J. Occup. Ther. 2019, 82, 646–652. [Google Scholar] [CrossRef]
- Fänge, A.M.; Carlsson, G.; Axmon, A.; Thordardottir, B.; Chiatti, C.; Nilsson, M.H.; Ekstam, L. Effects of applying a standardized assessment and evaluation protocol in housing adaptation implementation—Results from a quasi-experimental study. BMC Public Health 2019, 19, 1446. [Google Scholar]
- Cawood, A.L.; Elia, M.; Sharp, S.K.; Stratton, R.J. Malnutrition self-screening by using MUST in hospital outpatients: Validity, reliability, and ease of use. Am. J. Clin. Nutr. 2012, 96, 1000–1007. [Google Scholar] [CrossRef] [Green Version]
- Rasheed, S.; Woods, R.T. Predictive validity of ‘Malnutrition Universal Screening Tool’ (‘MUST’) and Short Form Mini Nutritional Assessment (MNA-SF) in terms of survival and length of hospital stay. e-SPEN J. 2013, 8, e44–e50. [Google Scholar] [CrossRef]
- Elia, M. The ‘MUST’ Report: Nutritional Screening of Adults a Multidisciplinary Responsibility: Development and Use of the ‘Malnutrition Universal Screening Tool’ (‘MUST’) for Adults; BAPEN: Redditch, UK, 2003. [Google Scholar]
- Ahmed, T.; Haboubi, N. Assessment and management of nutrition in older people and its importance to health. Clin. Interv. Aging 2010, 5, 207–216. [Google Scholar]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Lou, S.J.; Hou, M.F.; Chang, H.T.; Chiu, C.C.; Lee, H.H.; Yeh, S.J.; Shi, H.Y. Machine Learning Algorithms to Predict Recurrence within 10 Years after Breast Cancer Surgery: A Prospective Cohort Study. Cancers 2020, 12, 3817. [Google Scholar] [CrossRef] [PubMed]
- Kuo, Y.H.; Chiu, C.C.; Tseng, L.Y.; Wu, C.H.; Chen, M.H.; Fang, Y.C.; Tseng, W.C.; Chen, C.H.; Yeh, S.J.; Shi, H.Y. Long-Term Trends and Predictors of Medical Resource Utilization and Medical Outcomes in Inguinal Hernia Repair: A Nationwide Cohort Study. World J. Surg. 2021, 45, 1771–1778. [Google Scholar] [CrossRef] [PubMed]
- Borm, G.F.; Fransen, J.; Lemmens, W.A. A simple sample size formula for analysis of covariance in randomized clinical trials. J. Clin. Epidemiol. 2007, 60, 1234–1238. [Google Scholar] [CrossRef]
- Naylor, M.D.; Aiken, L.H.; Kurtzman, E.T.; Olds, D.M.; Hirschman, K.B. The care span: The importance of transitional care in achieving health reform. Health Aff. 2011, 30, 746–754. [Google Scholar] [CrossRef]
- Verhaegh, K.J.; MacNeil-Vroomen, J.L.; Eslami, S.; Geerlings, S.E.; de Rooij, S.E.; Buurman, B.M. Transitional care interventions prevent hospital readmissions for adults with chronic illnesses. Health Aff. 2014, 33, 1531–1539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Low, L.L.; Vasanwala, F.F.; Ng, L.B.; Chen, C.; Lee, K.H.; Tan, S.Y. Effectiveness of a transitional home care program in reducing acute hospital utilization: A quasi-experimental study. BMC Health Serv. Res. 2015, 15, 100. [Google Scholar] [CrossRef] [Green Version]
- Auerbach, A.D.; Kripalani, S.; Vasilevskis, E.E.; Sehgal, N.; Lindenauer, P.K.; Metlay, J.P.; Fletcher, G.; Ruhnke, G.W.; Flanders, S.A.; Kim, C.; et al. Preventability and causes of readmissions in a national cohort of general medicine patients. JAMA Intern. Med. 2016, 176, 484–493. [Google Scholar] [CrossRef]
- Braet, A.; Weltens, C.; Sermeus, W. Effectiveness of discharge interventions from hospital to home on hospital readmissions: A systematic review. JBI Database Syst. Rev. Implement Rep. 2016, 14, 106–173. [Google Scholar] [CrossRef] [PubMed]
- Mabire, C.; Dwyer, A.; Garnier, A.; Pellet, J. Meta-analysis of the effectiveness of nursing discharge planning interventions for older inpatients discharged home. J. Adv. Nurs. 2018, 74, 788–799. [Google Scholar] [CrossRef]
- Zurlo, A.; Zuliani, G. Management of care transition and hospital discharge. Aging Clin. Exp. Res. 2018, 30, 263–270. [Google Scholar] [CrossRef]
- Yuan, B.; Li, J.; Wu, L.; Wang, Z. Multi-Level Social Health Insurance System in the Age of Frequent Employment Change: The Urban Unemployment-Induced Insurance Transition and Healthcare Utilization in China. Healthcare 2019, 7, 77. [Google Scholar] [CrossRef] [Green Version]
- Ridwan, E.S.; Hadi, H.; Wu, Y.L.; Tsai, P.S. Effects of Transitional Care on Hospital Readmission and Mortality Rate in Subjects With COPD: A Systematic Review and Meta-Analysis. Respir. Care 2019, 64, 1146–1156. [Google Scholar] [CrossRef]
- Damy, T.; Chouihed, T.; Delarche, N.; Berrut, G.; Cacoub, P.; Henry, P.; Lamblin, N.; Andrès, E.; Hanon, O. Diagnosis and Management of Heart Failure in Elderly Patients from Hospital Admission to Discharge: Position Paper. J. Clin. Med. 2021, 10, 3519. [Google Scholar] [CrossRef]
- Condon, C.; Lycan, S.; Duncan, P.; Bushnell, C. Reducing readmissions after stroke with a structured nurse practitioner/registered nurse transitional stroke program. Stroke 2016, 47, 1599–1604. [Google Scholar] [CrossRef] [Green Version]
- Buurman, B.M.; Hoogerduijn, J.G.; de Haan, R.J.; Abu-Hanna, A.; Lagaay, A.M.; Verhaar, H.J.; Schuurmans, M.J.; Levi, M.; de Rooij, S.E. Geriatric conditions in acutely hospitalized older patients: Prevalence and one-year survival and functional decline. PLoS ONE 2011, 6, e26951. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Standard Transition Cohort (n = 49) | Seamless Transition Cohort (n = 119) | p Value | |
|---|---|---|---|---|
| Demographic characteristics | ||||
| Age, years | 80.88 ± 9.96 | 77.77 ± 11.32 | 0.097 | |
| Gender | Male | 33(67.3%) | 70(58.8%) | 0.392 |
| Female | 16(32.7%) | 49(41.2%) | ||
| Body mass index, km/m2 | 22.31 ± 4.24 | 22.79 ± 3.97 | 0.486 | |
| Education, years | 7.88 ± 5.37 | 6.50 ± 4.9 | 0.110 | |
| Marital status | Single | 5(10.2%) | 4(3.4%) | 0.208 |
| Married | 32(65.3%) | 79(66.4%) | ||
| Widowed | 12(24.5%) | 36(30.3%) | ||
| Family support * | 1.08 ± 0.53 | 1.08 ± 0.51 | 0.979 | |
| Smoking | Yes | 3(6.1%) | 17(14.3%) | 0.221 |
| Drinking | Yes | 5(10.2%) | 7(5.9%) | 0.338 |
| Clinical characteristics | ||||
| Charlson Comorbidity Index, score | 4.25 ± 2.64 | 4.60 ± 3.28 | 0.506 | |
| Multimorbidity Frailty Index | 0.15 ± 0.87 | 0.14 ± 0.11 | 0.849 | |
| Activities of Daily Living * | 0 | 3(6.1%) | 15(12.6%) | 0.059 |
| 1 | 8(16.3%) | 24(20.2%) | ||
| 2 | 20(40.8%) | 25(21.0%) | ||
| 3 | 18(36.7%) | 55(46.2%) | ||
| Malnutrition Universal Screening Tool * | 0 | 33(67.3%) | 78(65.5%) | 0.265 |
| 1 | 4(8.2%) | 20(16.8%) | ||
| 2 | 12(24.5%) | 21(17.6%) | ||
| Discharged with urinary catheter | Yes | 10(20.4%) | 34(28.6%) | 0.368 |
| Medical resource utilization | ||||
| Length of stay before discharge, days | 25.71 ± 23.40 | 22.61 ± 15.90 | 0.399 | |
| Total direct medical costs during hospitalization, USD | 148,231.78 ± 105,067.45 | 135,976.91 ± 127,758.22 | 0.554 | |
| Total outpatient costs at 6 months after discharge, USD | 21,237.92 ± 13,778.73 | 15,316.95 ± 14,330.01 | 0.015 | |
| Total inpatient costs at 6 months after discharge, USD | 76,329.61 ± 209,050.34 | 33,066.32 ± 60,084.40 | 0.040 | |
| Total emergency room costs at 6 months after discharge, USD | 9215.75 ± 12,423.25 | 4515.60 ± 6687.79 | 0.002 | |
| Total medical direct costs before and 6 months after discharge, USD | 255,015.05 ± 267,362.66 | 188,875.78 ± 152,821.57 | 0.045 | |
| Medical outcomes | ||||
| Readmission within 14 days after discharge | Yes | 2(4.1%) | 13(10.9%) | 0.235 |
| Readmission within 30 days after discharge | Yes | 8(16.3%) | 23(19.3%) | 0.813 |
| Readmission within 90 days after discharge | Yes | 11(22.4%) | 37(31.1%) | 0.348 |
| Readmission within 180 days after discharge | Yes | 21(42.9%) | 46(38.7%) | 0.740 |
| Mortality | Yes | 5(10.2%) | 18(15.1%) | 0.551 |
| Unplanned Readmission within 14 Days | Unplanned Readmission within 30 Days | Unplanned Readmission within 90 Days | Unplanned Readmission within 180 Days | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variable | OR | 95% C.I. | p Value | OR | 95% C.I. | p Value | OR | 95% C.I. | p Value | OR | 95% C.I. | p Value |
| Transition cohort, seamless vs. standard | 3.53 | 0.69–18.00 | 0.130 | 1.19 | 0.40–3.57 | 0.759 | 2.03 | 0.82–5.01 | 0.125 | 0.96 | 0.46–1.98 | 0.906 |
| Age | 1.01 | 0.96–1.07 | 0.639 | 1.03 | 0.99–1.07 | 0.217 | 1.02 | 0.99–1.06 | 0.168 | 1.03 | 1.01–1.06 | 0.032 |
| Gender, male vs. female | 0.08 | 0.01–0.54 | 0.010 | 0.39 | 0.13–1.18 | 0.094 | 0.96 | 0.42–2.19 | 0.929 | 1.01 | 0.52–1.94 | 0.986 |
| Body mass index, km/m2 | 1.01 | 0.85–1.18 | 0.991 | 1.02 | 0.92–1.14 | 0.664 | 0.96 | 0.89–1.03 | 0.250 | 0.94 | 0.87–1.01 | 0.055 |
| Education, years | 1.02 | 0.90–1.16 | 0.729 | 1.03 | 0.94–1.14 | 0.501 | 1.02 | 0.95–1.10 | 0.624 | |||
| Marital status | ||||||||||||
| Married vs. single | 0.12 | 0.02–0.91 | 0.040 | 0.12 | 0.02–0.78 | 0.026 | 0.27 | 0.05–1.48 | 0.130 | |||
| Widowed vs. single | 0.07 | 0.01–0.62 | 0.017 | 0.10 | 0.01–0.66 | 0.017 | 0.19 | 0.03–1.12 | 0.066 | |||
| Family support * | 0.40 | 0.12–1.36 | 0.143 | 0.29 | 0.12–0.72 | 0.008 | 0.50 | 0.24–1.04 | 0.064 | 0.71 | 0.37–1.35 | 0.294 |
| Smoking, yes vs. no | 0.31 | 0.03–2.89 | 0.302 | 0.27 | 0.05–1.55 | 0.142 | 0.29 | 0.07–1.20 | 0.088 | |||
| Drinking, yes vs. no | 0.48 | 0.04–5.46 | 0.553 | 0.82 | 0.13–5.12 | 0.834 | 0.62 | 0.11–3.51 | 0.592 | |||
| Charlson Comorbidity Index, score | 1.14 | 0.95–1.36 | 0.168 | 1.16 | 1.01–1.35 | 0.046 | 1.12 | 0.99–1.27 | 0.079 | |||
| Multimorbidity Frailty Index | 0.13 | 0.01–87.00 | 0.541 | 0.58 | 0.01–11.20 | 0.840 | 10.60 | 0.16–70.94 | 0.270 | |||
| Activities of Daily Living * | ||||||||||||
| 1 vs. 0 | 0.37 | 0.05–2.99 | 0.350 | 0.27 | 0.05–1.63 | 0.153 | 0.75 | 0.19–2.96 | 0.681 | 2.20 | 6.31–7.64 | 0.217 |
| 2 vs. 0 | 0.48 | 0.07–3.47 | 0.466 | 0.24 | 0.04–1.31 | 0.098 | 0.69 | 0.18–2.65 | 0.585 | 1.20 | 0.35–4.12 | 0.772 |
| 3 vs. 0 | 0.22 | 0.03–1.41 | 0.109 | 0.69 | 0.16–2.94 | 0.615 | 0.99 | 0.30–3.25 | 0.992 | 2.14 | 0.70–6.59 | 0.183 |
| Malnutrition Universal Screening Tool * | ||||||||||||
| 1 vs. 0 | 0.91 | 0.14–6.21 | 0.926 | 2.24 | 0.55–9.13 | 0.259 | ||||||
| 2 vs. 0 | 0.22 | 0.02–2.83 | 0.247 | 0.60 | 0.13–2.74 | 0.509 | ||||||
| Discharged with urinary catheter | ||||||||||||
| Yes vs. no | 2.39 | 0.68–8.39 | 0.175 | 3.18 | 1.20–8.43 | 0.020 | ||||||
| Unplanned Readmission within 14 Days | Unplanned Readmission within 30 Days | Unplanned Readmission within 90 Days | Unplanned Readmission within 180 Days | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variable | OR | 95% C.I. | p Value | OR | 95% C.I. | p Value | OR | 95% C.I. | p Value | OR | 95% C.I. | p Value |
| Transition cohort, seamless vs. standard | 3.53 | 0.69–18.00 | 0.130 | 1.19 | 0.40–3.57 | 0.759 | 2.03 | 0.82–5.01 | 0.125 | 0.96 | 0.46–1.98 | 0.906 |
| Age | 1.01 | 0.96–1.07 | 0.639 | 1.03 | 0.99–1.07 | 0.217 | 1.02 | 0.99–1.06 | 0.168 | 1.03 | 1.01–1.06 | 0.032 |
| Gender, male vs. female | 0.08 | 0.01–0.54 | 0.010 | 0.39 | 0.13–1.18 | 0.094 | 0.96 | 0.42–2.19 | 0.929 | 1.01 | 0.52–1.94 | 0.986 |
| Body mass index, km/m2 | 1.01 | 0.85–1.18 | 0.991 | 1.02 | 0.92–1.14 | 0.664 | 0.96 | 0.89–1.03 | 0.250 | 0.94 | 0.87–1.01 | 0.055 |
| Education, years | 1.02 | 0.90–1.16 | 0.729 | 1.03 | 0.94–1.14 | 0.501 | 1.02 | 0.95–1.10 | 0.624 | |||
| Marital status | ||||||||||||
| Married vs. single | 0.12 | 0.02–0.91 | 0.040 | 0.12 | 0.02–0.78 | 0.026 | 0.27 | 0.05–1.48 | 0.130 | |||
| Widowed vs. single | 0.07 | 0.01–0.62 | 0.017 | 0.10 | 0.01–0.66 | 0.017 | 0.19 | 0.03–1.12 | 0.066 | |||
| Family support * | 0.40 | 0.12–1.36 | 0.143 | 0.29 | 0.12–0.72 | 0.008 | 0.50 | 0.24–1.04 | 0.064 | 0.71 | 0.37–1.35 | 0.294 |
| Smoking, yes vs. no | 0.31 | 0.03–2.89 | 0.302 | 0.27 | 0.05–1.55 | 0.142 | 0.29 | 0.07–1.20 | 0.088 | |||
| Drinking, yes vs. no | 0.48 | 0.04–5.46 | 0.553 | 0.82 | 0.13–5.12 | 0.834 | 0.62 | 0.11–3.51 | 0.592 | |||
| Charlson Comorbidity Index, score | 1.14 | 0.95–1.36 | 0.168 | 1.16 | 1.01–1.35 | 0.046 | 1.12 | 0.99–1.27 | 0.079 | |||
| Multimorbidity Frailty Index | 0.13 | 0.01–87.00 | 0.541 | 0.58 | 0.01–11.20 | 0.840 | 10.60 | 0.16–70.94 | 0.270 | |||
| Activities of Daily Living * | ||||||||||||
| 1 vs. 0 | 0.37 | 0.05–2.99 | 0.350 | 0.27 | 0.05–1.63 | 0.153 | 0.75 | 0.19–2.96 | 0.681 | 2.20 | 6.31–7.64 | 0.217 |
| 2 vs. 0 | 0.48 | 0.07–3.47 | 0.466 | 0.24 | 0.04–1.31 | 0.098 | 0.69 | 0.18–2.65 | 0.585 | 1.20 | 0.35–4.12 | 0.772 |
| 3 vs. 0 | 0.22 | 0.03–1.41 | 0.109 | 0.69 | 0.16–2.94 | 0.615 | 0.99 | 0.30–3.25 | 0.992 | 2.14 | 0.70–6.59 | 0.183 |
| Malnutrition Universal Screening Tool * | ||||||||||||
| 1 vs. 0 | 0.91 | 0.14–6.21 | 0.926 | 2.24 | 0.55–9.13 | 0.259 | ||||||
| 2 vs. 0 | 0.22 | 0.02–2.83 | 0.247 | 0.60 | 0.13–2.74 | 0.509 | ||||||
| Discharged with urinary catheter | ||||||||||||
| Yes vs. no | 2.39 | 0.68–8.39 | 0.175 | 3.18 | 1.20–8.43 | 0.020 | ||||||
| Mean Value | Seamless Transition Cohort (n = 119) | Standard Transition Cohort (n = 49) | Difference * (Seamless–Standard) |
|---|---|---|---|
| Total direct medical costs during hospitalization | 4458.26 | 4860.06 | −401.80 |
| Total outpatient costs at 6 months after discharge | 502.20 | 696.32 | −194.12 |
| Total inpatient costs at 6 months after discharge | 1084.14 | 2502.61 | −1418.47 |
| Total emergency costs at 6 months after discharge | 148.05 | 302.15 | −154.10 |
| Total direct medical costs at 6 months after discharge | 6192.65 | 8361.15 | −2168.50 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.-C.; Lee, W.-Y.; Chou, M.-Y.; Liang, C.-K.; Chen, H.-F.; Yeh, S.-C.J.; Yaung, C.-L.; Tsai, K.-T.; Huang, J.-J.; Wang, C.; et al. Cost and Effectiveness of Long-Term Care Following Integrated Discharge Planning: A Prospective Cohort Study. Healthcare 2021, 9, 1413. https://doi.org/10.3390/healthcare9111413
Wang Y-C, Lee W-Y, Chou M-Y, Liang C-K, Chen H-F, Yeh S-CJ, Yaung C-L, Tsai K-T, Huang J-J, Wang C, et al. Cost and Effectiveness of Long-Term Care Following Integrated Discharge Planning: A Prospective Cohort Study. Healthcare. 2021; 9(11):1413. https://doi.org/10.3390/healthcare9111413
Chicago/Turabian StyleWang, Yu-Chun, Wen-Ying Lee, Ming-Yueh Chou, Chih-Kuang Liang, Hsueh-Fen Chen, Shu-Chuan Jennifer Yeh, Chih-Liang Yaung, Kang-Ting Tsai, Joh-Jong Huang, Chi Wang, and et al. 2021. "Cost and Effectiveness of Long-Term Care Following Integrated Discharge Planning: A Prospective Cohort Study" Healthcare 9, no. 11: 1413. https://doi.org/10.3390/healthcare9111413