
How Can Hybrid Simulation Support Organizations in Assessing COVID-19 Containment Measures?


Abstract
:1. Introduction
2. Background
2.1. Epidemiological Studies
2.2. Simulation Advantages for COVID-19 Containment
- Simulation allows the investigation of many different process configurations in one model, regardless of how complex they are. This aspect allows us to model even very complex organizations in which different parallel processes coexist, and several different people flows intersect.
- Simulation supports “what-if” analyses. “What-if” analysis can provide insights into an existing or a hypothetical situation, allowing for safe, replicable, and usually less expensive performance tests [24]. This aspect can allow analyzing in advance the processes considering the evolution of the pandemic and the government decisions, trying to understand how to re-plan organizations as external variables change.
- Simulation can allow the analysis and measurement of the dynamic performance of a given process and the assessment of both the presence and relevance of any grouping or area at risk of contagion.
- Simulation offers interactive and visual assistance for modeling the process and the flow of people, facilitating the comprehension of the model and of its results, enhancing the validation process [25].
2.3. Simulation Approaches for Re-design Organization People Flow during the COVID-19 Pandemic
- Model a variety of possible individual infection phases and individual interactions. ABM responds directly to the necessity of defining individual rules and behavior and describes a decentralized system as agents that can behave independently from one another. ABM has the advanced capability of tracking the movement of disease and the contacts between each individual in a population located in a predefined area. Agents would ideally work in representing various human beings in different infection phases. ABM can be used to study and track the movement of infected individuals and their contacts in a social system. In a DES, where entities (individual) can only have a passive behavior, the interaction between them can be defined a priori and can be represented by interacting with the individual. Based on stocks and continuous flows rather than on discrete entities, SD can describe interactions only at a high level of abstraction.
- Describe inner behavior uncertainties for the individual. The use of stochastic variables in DES allows simulating process-related uncertainties within the process of an organization (e.g., customer arrival rate, duration of activities, reliability of resources) [33], while ABM allows extending the uncertainty to human behaviors. Based on differential equations, SD may not be the best choice [29].
- Model individual actions and organizational processes in time and space. Both DES and ABM can respond to these. In DES, individual modeling is mainly related to their discrete action over time, but it can also capture spatial factors [40], while ABM can be used to model individuals as active agents if the modeler wants to give a higher relevance to their active interaction within the system [37]. The high detail level of SD would not fit the scope. The spread of human epidemics strongly relies on individual social networks and relations within the population. Therefore, modeling the environment where the discrete individuals interact makes it possible to understand spatial characteristics in spreading dynamics.
- Monitor and evaluate the spread of the contagion within different control policies. The ABM approach can be designed to allow epidemiological researchers to do a preliminary “what-if” analysis to assess systems’ behavior under various conditions and to evaluate which alternative control policies to adopt in a predefined time and space to fight epidemics. DES can be used to model and evaluate different control policies applied in organizational processes or individual actions.
3. Methodology
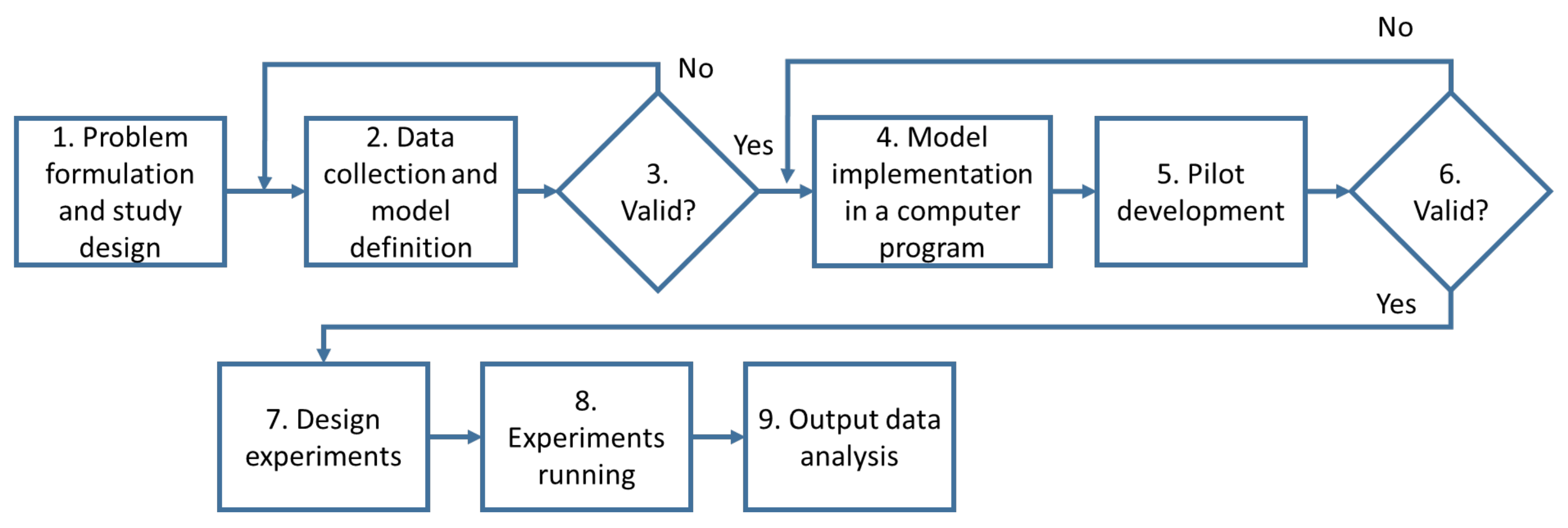
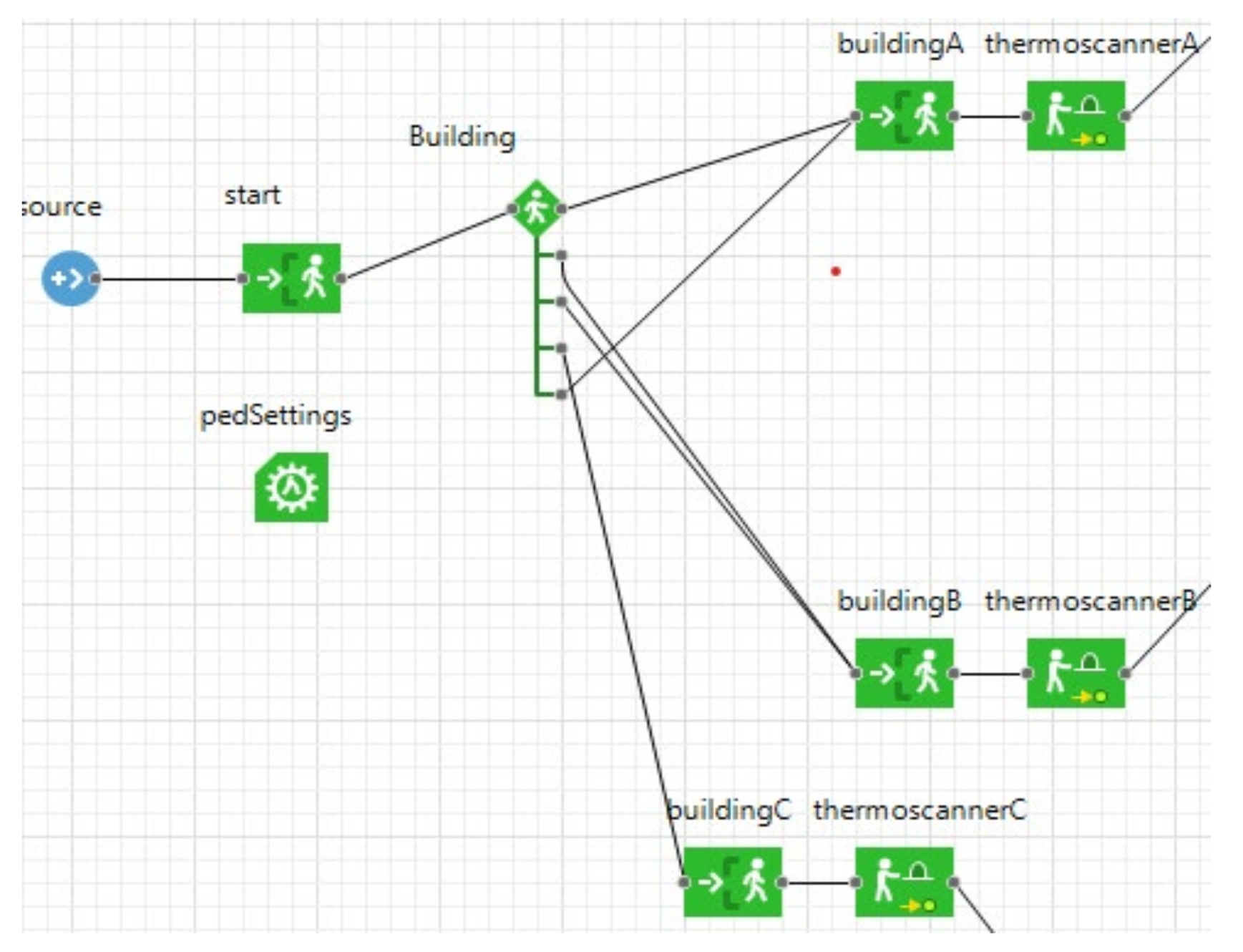
- Problem formulation and study design: the problem under investigation is the assessment of people flows management to contain the spread of COVID-19 in closed environments such as work and study places. In order to face this problem, it was decided to apply a Hybrid Simulation (HS) model. The reasons behind this choice are extensively explained in Section 2.3. The HS integrates an ABM to figure the spread of the virus and a DES to model the interactions of flows of people moving in closed environments interacting with each other (see Section 4 for details).
- Data collection and model definition: in this step, we started to collect the data necessary to define the ABM and the DES models better to include them in the HS model. In particular, in order to define the details of the agent-based model, it was necessary to include all the variables involved in the spread of the virus, which are already present both in the scientific literature and in the recommendations of national and international bodies, such as the infection index, the percentage of symptomatic individuals, the incubation period and the contagion probability (reported in the Section 4.1). Then, to define the discrete event simulation model that models the interactions between flows of people, it is necessary to have people’s paths within the environments, the plans of the buildings included in the study, and the infection rules (reported in the Section 4.2). Once all the variables and parameters included in the models were defined, a first validation was needed.
- Validation: validation should be done throughout the entire simulation study [38], in particular, in the building of the model it is necessary to interact with decision-makers to check the reliability of the parameters’ values set in the model. We check our choices by interacting both with an epidemiologist (for checking the epidemiology values) and with a university campus manager (for checking the policies and retrieving data about course composition and the availability of the spaces).
- Model implementation in a computer program: the models were then implemented in the software used as a tool for integrated simulation, in our case Anylogic 8.7.1.
- Pilot development: as a pilot model, a university campus case study was chosen for which all the data were known (see Section 5.1).
- Validation: the pilot model had been tested with a sensitivity analysis fully described in Section 5.2.
- Design experiments: once the pilot model had been tested, different experiment settings were designed to understand how the model changes when certain elements that strongly influence the spread of the virus were changed.
- Experiment running: the model’s behavior was analyzed when the percentage of classrooms occupied and the efficiency of the protection provided by the masks varied (see Section 5.3 for more details).
- Output data analysis: the results were analyzed, providing valuable indications both for the containment of Covid-19 on the University campus analyzed (and for future research directions as reported in Section 6).
4. The Hybrid Simulation Model
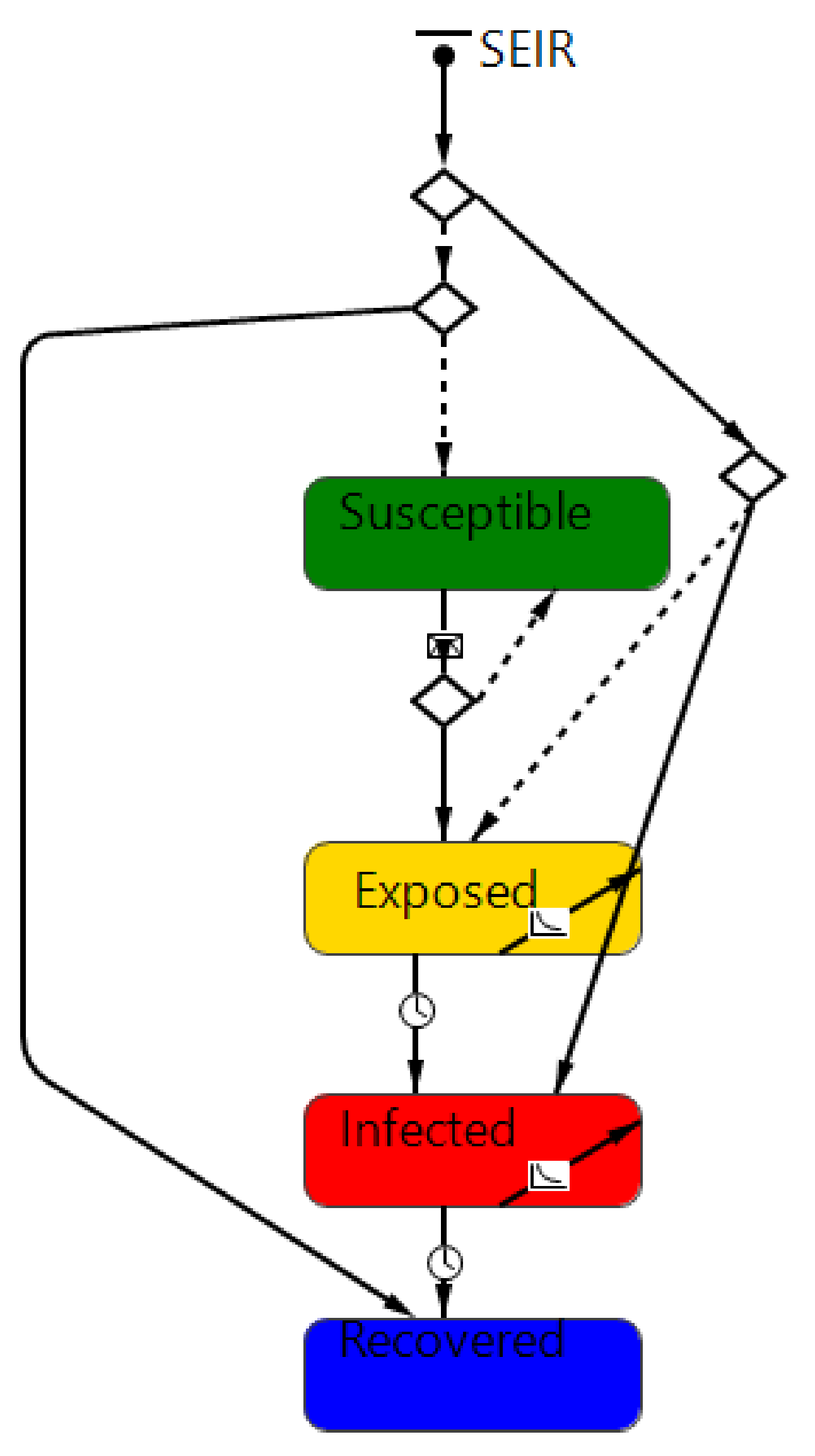
- The first sub-model was designed to describe the generic COVID-19 infection model: in this perspective, a SEIR agent-based model has been developed and adopted;
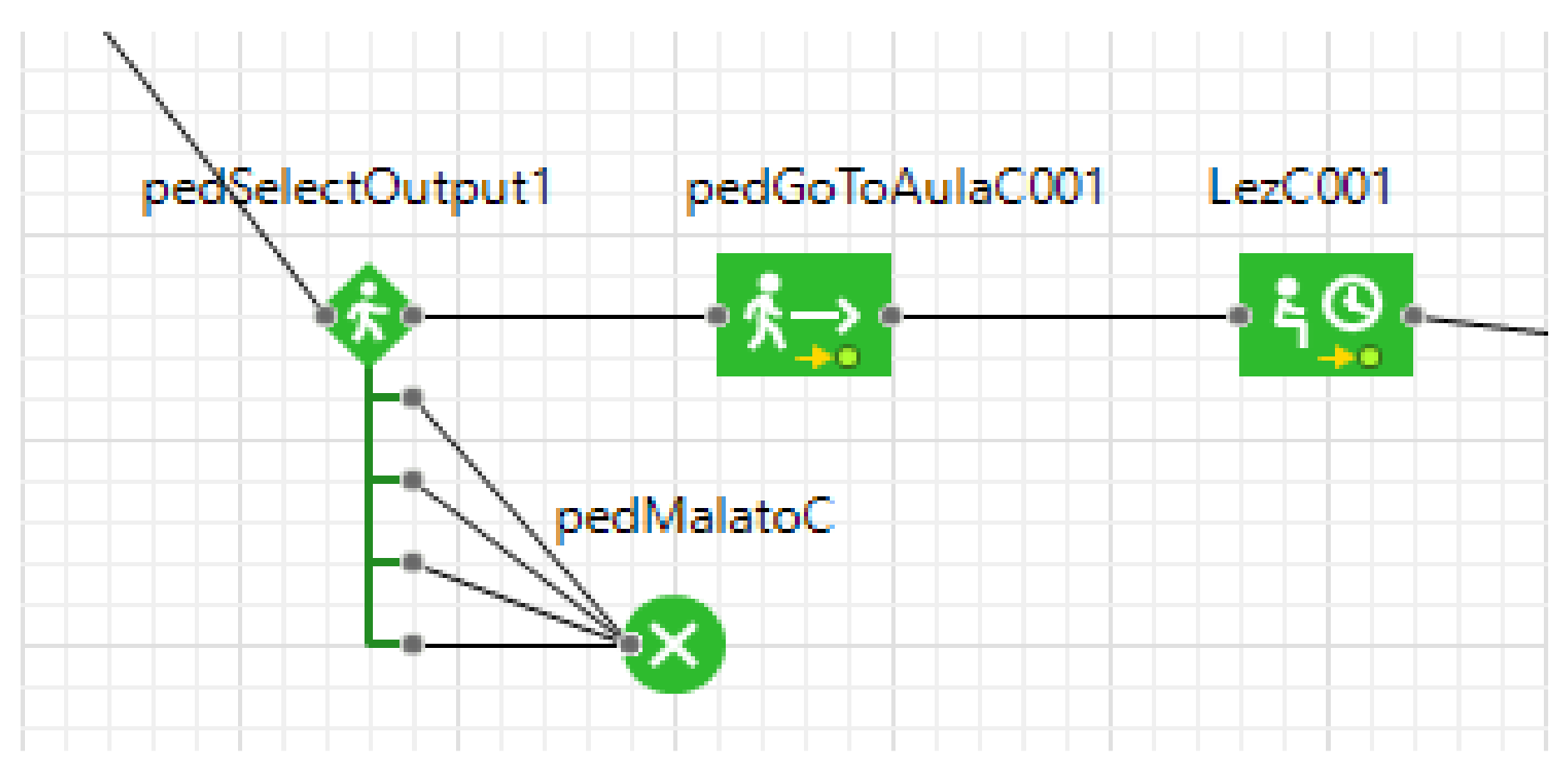
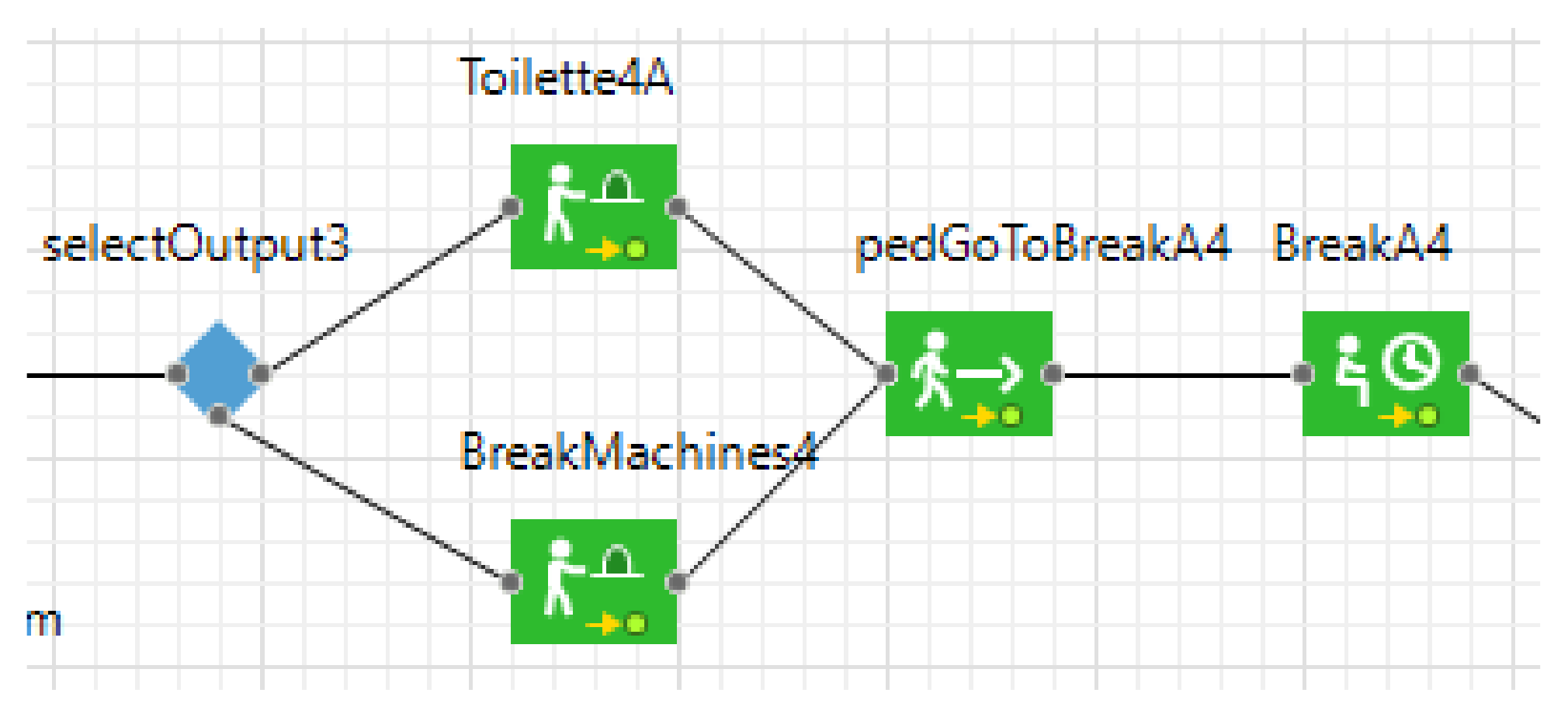
- The second sub-model was conceived to represent the flow and actions of the individual within the organization, leading to a description of the space of individual interactions while performing their activities. For this purpose, a discrete-event simulation has been adopted.
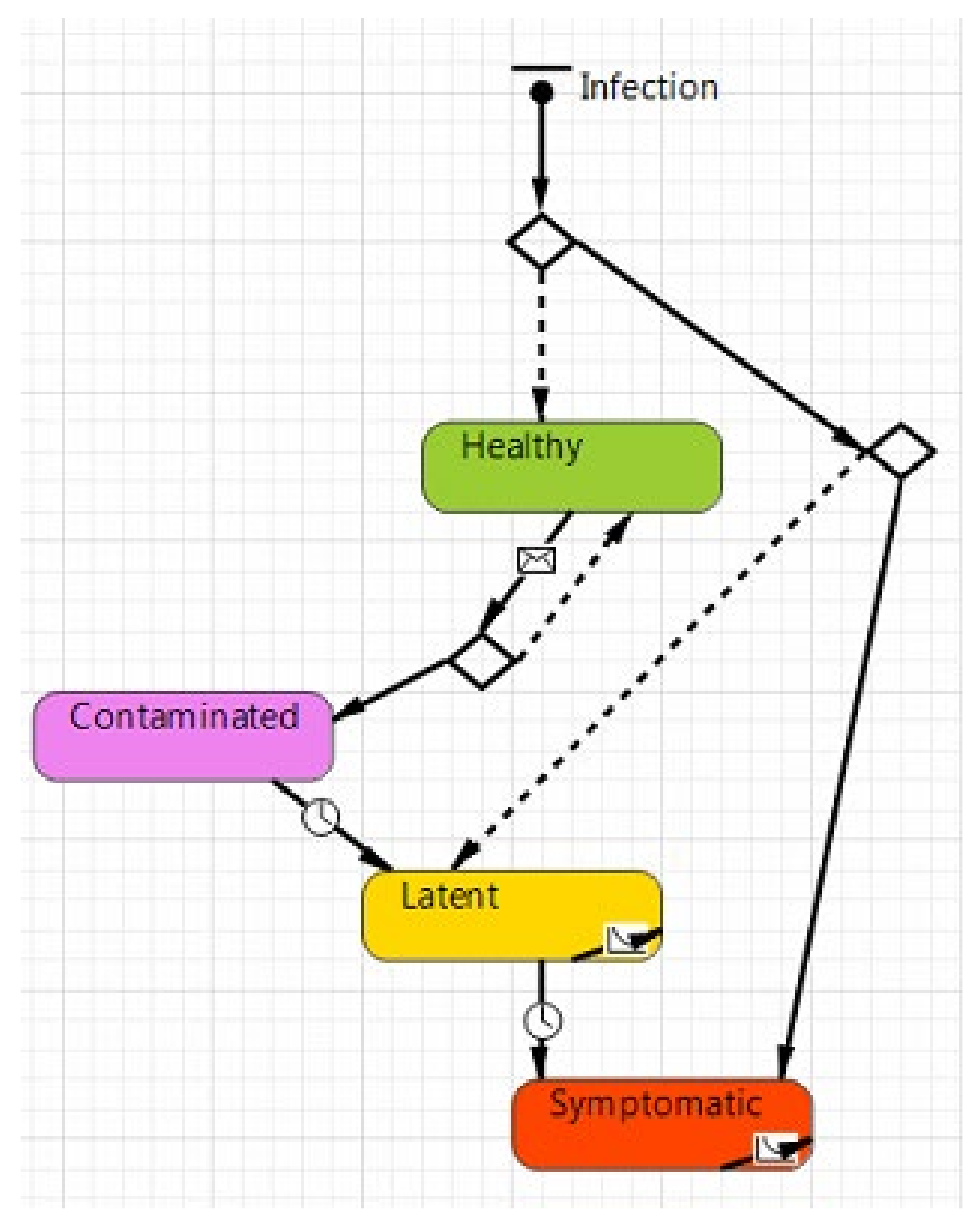
4.1. COVID-19 Infection Model
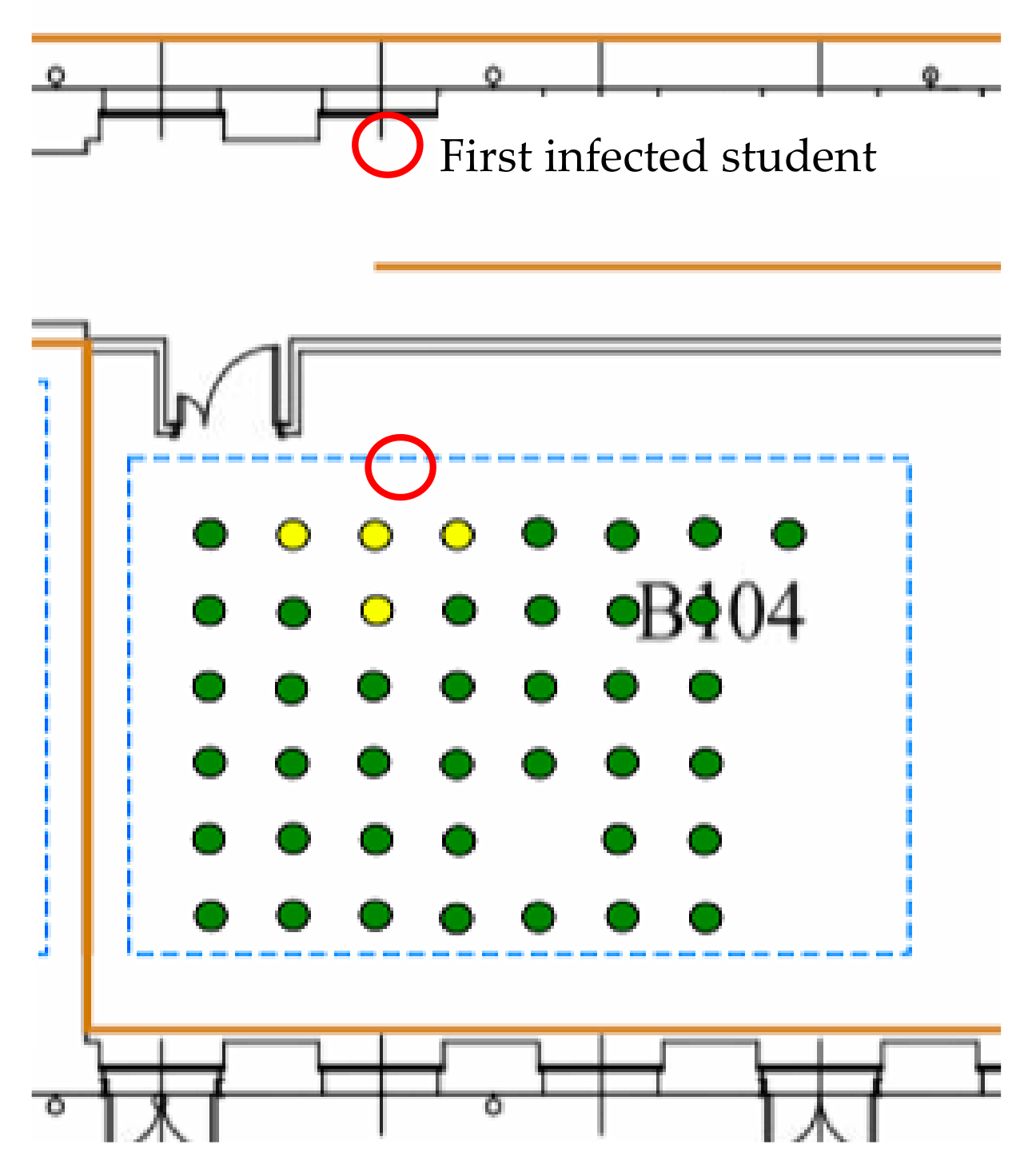
- Healthy (represented by a green color), in this state there are all those individuals who have not contracted the virus and are in good health;
- Contaminated (represented by purple color), which is the state of individuals that are infected during the simulation run but cannot yet contaminate other individuals;
- Latent (represented by yellow color), in this state all those individuals have contracted the SARS-CoV-2, but the disease does not manifest itself with any external signs or symptoms. However, latent individuals are contagious;
- Symptomatic (represented by red color), in this state there are all those individuals that are contaminated and can contaminate other people. They differ from the previous state because these show evident symptoms, such as fever.
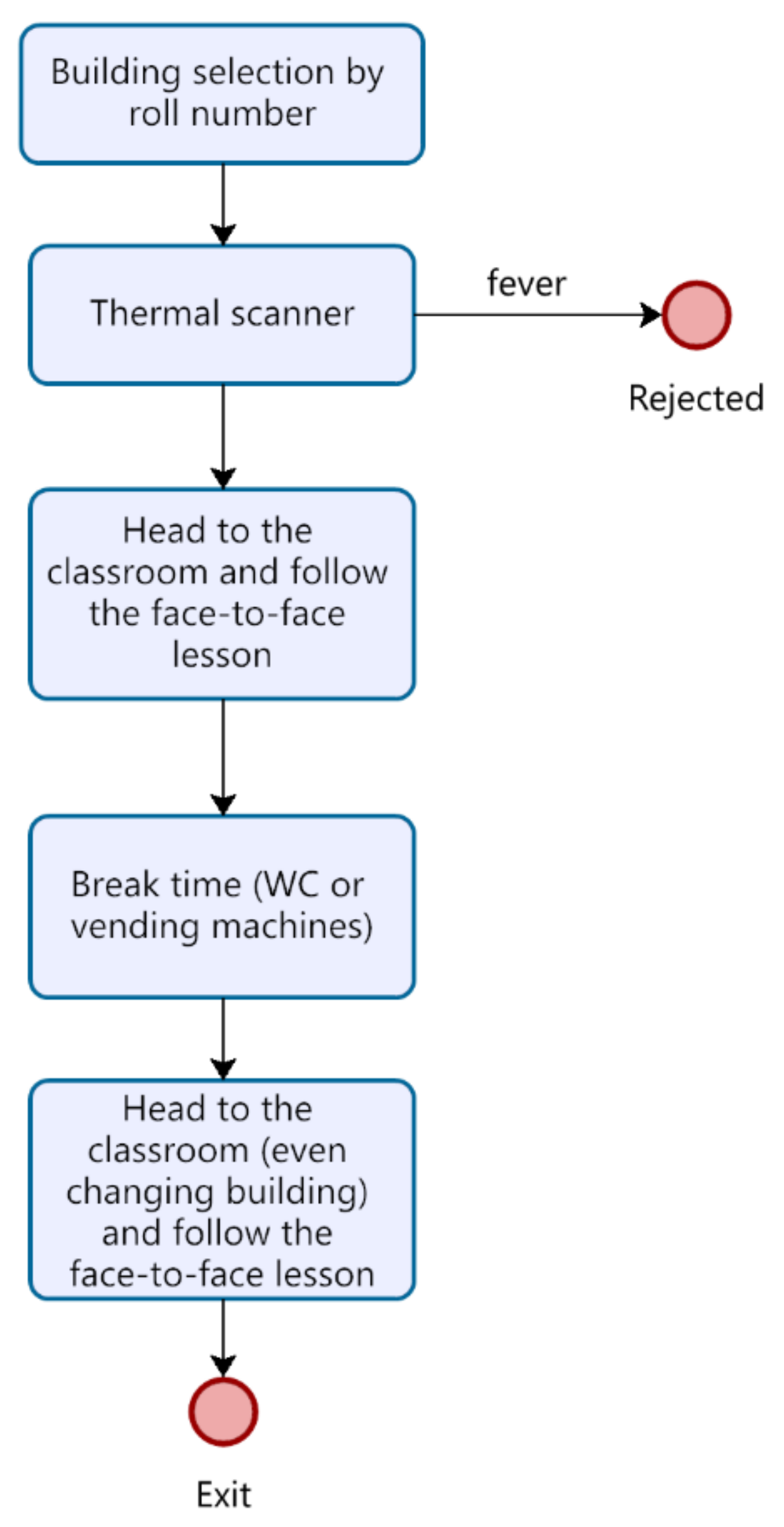
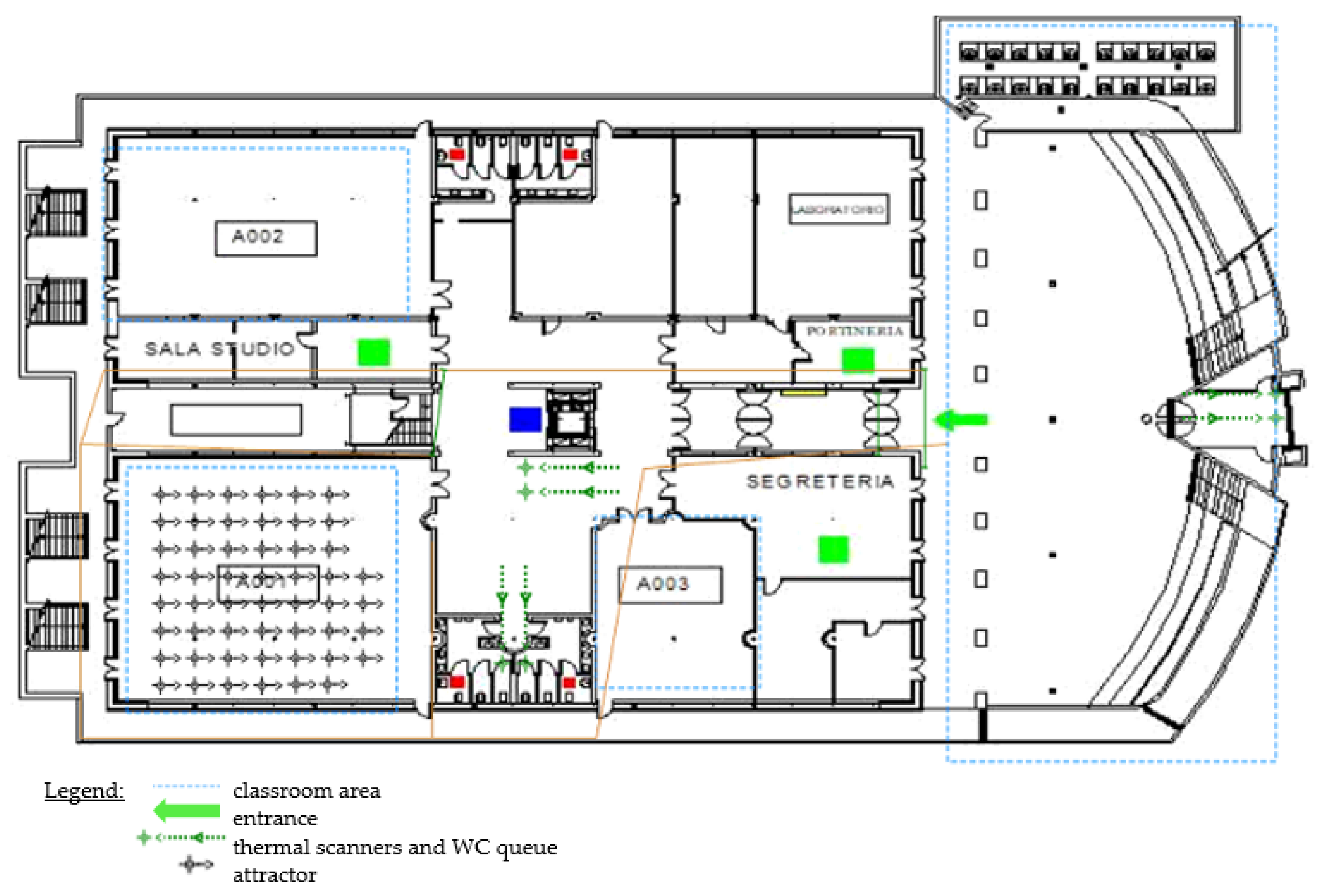
4.2. People Flow
5. The Test Case Analysis: University of Bergamo Case
5.1. Case Description
- Body temperature detectors at each entrance;
- The obligation to wear a mask;
- Defined paths to follow to move inside the buildings (entrances and exits);
- Sanitizing gel dispensers in all the most frequented points and the classrooms;
- Indicators for the distancing of the counters with access to the public.
5.2. Model Validation Scenarios
5.3. Case Results—Testing Alternative Scenarios
- Surgical masks, which do not adhere perfectly to the contours of the face, so the protection of the wearer is limited, but they prevent the escape of respiratory secretions/droplets to the external environment;
- FFP masks (filtering facepiece particles) protect both the wearer and others, filtering the particles in the air down to a size of 0.6 µm. They filter from 80% (FFP1) to 99% (FFP3) of the particles;
- Non-sanitary masks (i.e., fabric masks) are not considered medical or personal protective equipment.
- The fit of the mask is highly influential on its efficiency (if there is a gap, that is, the mask does not adhere well to the face, then the protection decreases), hence the importance of wearing it in the best possible way;
- Masks can reduce the intelligibility of the speech signal [66] and reduce the intensity of sounds passed through them. As a response, people tend to speak louder, and therefore the number of emitted particles theoretically increases.
6. Discussion on the Use of Hybrid Modeling to Design People Flow to Minimize COVID-19 Diffusion
- Models segregation: the flow and the epidemiological models are clearly separated, allowing for a better description of the different aspects via using the appropriate modeling notation (i.e., DES for the people flow and agent-based for the person contagious spread).
- Flexibility: although in general it would be possible to model the agent (i.e., students) flow and the contagious infection spread using only DES through a long and complex sequence of ‘if-then’ blocks, attributes and variables, the segregation of the models and the adoption of ABS allowed higher flexibility, especially when the agent population and the characteristics of epidemiological model change (e.g., the statechart can be easily modified considering the evolution of the knowledge on COVID-19).
- Detection of critical situation in advance: the interactions between agents (i.e., students) in the system (i.e., University) can highlight in advance possible critical situation that may verify in the environment due to the interactions among agents within the population. In summary, the hybrid approach allows for the identification of results and outcomes that would be extremely difficult to detect via a DES or ABS approach alone. The higher the number of students or other variables, the higher the difficulty of the pure DES to identify additional outcomes.
- Simplicity/effectiveness: due to its nature, agent-based modeling allows for better and simplified modeling of the compartmental models typically used to model infection spreading, eliminating the necessity of modeling the virus behaviour via complex DES constructs.
7. Conclusions
7.1. Limitation of the Study
7.2. Future Developments
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Hu, B.; Guo, H.; Zhou, P.; Shi, Z.-L. Characteristics of SARS-CoV-2 and COVID-19. Nat. Rev. Microbiol. 2020, 19, 141–154. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Flessa, S. Modelling Covid-19 under Uncertainty: What Can We Expect? Eur. J. Health Econ. 2020, 21, 665–668. [Google Scholar] [CrossRef] [PubMed]
- Hoertel, N.; Blachier, M.; Blanco, C.; Olfson, M.; Massetti, M.; Rico, M.S.; Limosin, F.; Leleu, H. A Stochastic Agent-Based Model of the SARS-CoV-2 Epidemic in France. Nat. Med. 2020, 26, 1417–1421. [Google Scholar] [CrossRef] [PubMed]
- Groppi, M.; Marca, R.D. Modelli epidemiologici e vaccinazioni: Da Bernoulli a oggi. Mat. Cult. E Soc. Riv. DellUnione Mat. Ital. 2018, 3, 45–59. [Google Scholar]
- Martcheva, M. An Introduction to Mathematical Epidemiology; Texts in Applied Mathematics; Springer: Boston, MA, USA, 2015; Volume 61, ISBN 978-1-4899-7611-6. [Google Scholar]
- Smith, T.; Maire, N.; Ross, A.; Penny, M.; Chitnis, N.; Schapira, A.; Studer, A.; Genton, B.; Lengeler, C.; Tediosi, F.; et al. Towards a Comprehensive Simulation Model of Malaria Epidemiology and Control. Parasitology 2008, 135, 1507–1516. [Google Scholar] [CrossRef] [Green Version]
- Zhou, G.; Chi, C. A Model Simulation Study on Effects of Intervention Measures in Wuhan COVID-19 Epidemic. MedrXiv 2020. [Google Scholar] [CrossRef]
- Sameni, R. Mathematical Modeling of Epidemic Diseases; A Case Study of the COVID-19 Coronavirus. arXiv Prepr. 2020, arXiv:2003.11371. [Google Scholar]
- Zu, J.; Li, M.; Li, Z.; Shen, M.; Xiao, Y.; Ji, F. Epidemic Trend and Transmission Risk of SARS-CoV-2 after Government Intervention in the Mainland of China: A Mathematical Model Study. SSRN Electron. J. 2020. [Google Scholar] [CrossRef]
- Mummert, A.; Otunuga, O.M. Parameter Identification for a Stochastic SEIRS Epidemic Model: Case Study Influenza. J. Math. Biol. 2019, 79, 705–729. [Google Scholar] [CrossRef]
- Zhou, N.; Li, G.; Li, T.; Li, W.; Chen, M.; Zhang, S.; Zhang, H.; Zha, W.; Yuan, L. Using Simulation Technology to Analyze the COVID-19 Epidemic in Changsha, Hunan Province, China, 2020; In Review.
- Mahmood, I.; Jahan, M.; Groen, D.; Javed, A.; Shafait, F. An Agent-Based Simulation of the Spread of Dengue Fever. In Computational Science ICCS 2020; Krzhizhanovskaya, V.V., Závodszky, G., Lees, M.H., Dongarra, J.J., Sloot, P.M.A., Brissos, S., Teixeira, J., Eds.; Lecture Notes in Computer Science; Springer International Publishing: Cham, The Netherlands, 2020; Volume 12139, pp. 103–117. ISBN 978-3-030-50419-9. [Google Scholar]
- Hutton, G.; Molineaux, L.; Killeen, G.F.; Tediosi, F.; Ross, A.; Smith, T.; Tanner, M.; Dietz, K.; Utzinger, J.; Maire, N. Mathematical Modeling of the Impact of Malaria Vaccines on the Clinical Epidemiology and Natural History of Plasmodium Falciparum Malaria: Overview. Am. J. Trop. Med. Hyg. 2006, 75, 1–10. [Google Scholar] [CrossRef]
- Colizza, V.; Barrat, A.; Barthélemy, M.; Vespignani, A. Predictability and Epidemic Pathways in Global Outbreaks of Infectious Diseases: The SARS Case Study. BMC Med. 2007, 5, 34. [Google Scholar] [CrossRef]
- Fraser, C.; Riley, S.; Anderson, R.M.; Ferguson, N.M. Factors That Make an Infectious Disease Outbreak Controllable. Proc. Natl. Acad. Sci. USA 2004, 101, 6146–6151. [Google Scholar] [CrossRef] [Green Version]
- Klinkenberg, D.; Fraser, C.; Heesterbeek, H. The Effectiveness of Contact Tracing in Emerging Epidemics. PLoS ONE 2006, 1, e12. [Google Scholar] [CrossRef]
- Chen, S.-C.; Chang, C.-F.; Liao, C.-M. Predictive Models of Control Strategies Involved in Containing Indoor Airborne Infections. Indoor Air 2006, 16, 469–481. [Google Scholar] [CrossRef]
- Feng, Z.; Yang, Y.; Xu, D.; Zhang, P.; McCauley, M.M.; Glasser, J.W. Timely Identification of Optimal Control Strategies for Emerging Infectious Diseases. J. Theor. Biol. 2009, 259, 165–171. [Google Scholar] [CrossRef]
- Peak, C.M.; Childs, L.M.; Grad, Y.H.; Buckee, C.O. Comparing Nonpharmaceutical Interventions for Containing Emerging Epidemics. Proc. Natl. Acad. Sci. USA 2017, 114, 4023–4028. [Google Scholar] [CrossRef] [Green Version]
- Kwok, K.O.; Tang, A.; Wei, V.W.I.; Park, W.H.; Yeoh, E.K.; Riley, S. Epidemic Models of Contact Tracing: Systematic Review of Transmission Studies of Severe Acute Respiratory Syndrome and Middle East Respiratory Syndrome. Comput. Struct. Biotechnol. J. 2019, 17, 186–194. [Google Scholar] [CrossRef]
- Machado, S.D.; Tavares, J.E.D.R.; Martins, M.G.; Barbosa, J.L.V.; González, G.V.; Leithardt, V.R.Q. Ambient Intelligence Based on IoT for Assisting People with Alzheimer’s Disease Through Context Histories. Electronics 2021, 10, 1260. [Google Scholar] [CrossRef]
- Aranda, J.A.S.; Bavaresco, R.S.; de Carvalho, J.V.; Yamin, A.C.; Tavares, M.C.; Barbosa, J.L.V. A Computational Model for Adaptive Recording of Vital Signs through Context Histories. J. Ambient Intell. Humaniz. Comput. 2021, 1–15. [Google Scholar] [CrossRef]
- Telles, M.J.; Santos, R.; da Silva, J.M.; Righi, R.D.R.; Barbosa, J.L.V. An Intelligent Model to Assist People with Disabilities in Smart Cities. J. Ambient Intell. Smart Environ. 2021, 13, 301–324. [Google Scholar] [CrossRef]
- Hlupic, V.; Robinson, S. Business Process Modelling and Analysis Using Discrete-Event Simulation. In Proceedings of the 1998 Winter Simulation Conference, Proceedings (Cat. No.98CH36274), Washington, DC, USA,, 13–16 December 1998; Volume 2, pp. 1363–1369. [Google Scholar]
- Phumbua, S.; Tjahjono, B. Simulation Modelling of Product-Service Systems: The Missing Link. In Proceedings of the 36th International MATADOR Conference, Manchester, UK, 14–16 July 2010; Hinduja, S., Li, L., Eds.; Springer: London, UK, 2010; pp. 135–138. ISBN 978-1-84996-431-9. [Google Scholar]
- Currie, C.S.M.; Fowler, J.W.; Kotiadis, K.; Monks, T.; Onggo, B.S.; Robertson, D.A.; Tako, A.A. How Simulation Modelling Can Help Reduce the Impact of COVID-19. J. Simul. 2020, 14, 83–97. [Google Scholar] [CrossRef] [Green Version]
- Sterman, J.D. Business Dynamics: Systems Thinking and Modeling for a Complex. World; Irwin/McGraw-Hill: Boston, MA, USA, 2000; ISBN 978-0-07-238915-9. [Google Scholar]
- Leopold, A. Energy Related System Dynamic Models: A Literature Review. Cent. Eur. J. Oper. Res. 2016, 24, 231–261. [Google Scholar] [CrossRef]
- Borshchev, A.; Filippov, A. From System Dynamics and Discrete Event to Practical Agent Based Modeling: Reasons, Techniques, Tools. In Proceedings of the 22nd International Conference of the System Dynamics Society, Oxford, UK, 25–29 July 2004. [Google Scholar]
- Currie, D.J.; Smith, C.; Jagals, P. The Application of System Dynamics Modelling to Environmental Health Decision-Making and Policy—A Scoping Review. BMC Public Health 2018, 18, 402. [Google Scholar] [CrossRef] [Green Version]
- Davahli, M.; Karwowski, W.; Taiar, R. A System Dynamics Simulation Applied to Healthcare: A Systematic Review. Int. J. Environ. Res. Public. Health 2020, 17, 5741. [Google Scholar] [CrossRef]
- Brailsford, S.; Hilton, N. A comparison of discrete event simulation and system dynamics for modelling healthcare systems. In Planning for the Future: Health Service Quality and Emergency Accessibility. Operational Research Applied to Health Services (ORAHS); Glasgow Caledonian University: Glasgow, Scotland, 2001. [Google Scholar]
- Weidmann, D.; Maisenbacher, S.; Kasperek, D.; Maurer, M. Product-Service System Development with Discrete Event Simulation Modeling Dynamic Behavior in Product-Service Systems; IEEE: Manhattan, NY, USA, 2015; pp. 133–138. [Google Scholar]
- Hirth, N.; Maisenbacher, S.; Kasperek, D.; Hollauer, C.; Maurer, M. An Approach to Reveal Starting Points for PSS Design Support with Dynamic Models. Procedia CIRP 2015, 30, 462–467. [Google Scholar] [CrossRef] [Green Version]
- Brailsford, S. Discrete-Event Simulation Is Alive and Kicking! J. Simul. 2014, 8, 1–8. [Google Scholar] [CrossRef]
- Robinson, S. Modelling without Queues: Adapting Discrete-Event Simulation for Service Operations. J. Simul. 2015, 9, 195–205. [Google Scholar] [CrossRef] [Green Version]
- Maisenbacher, S.; Weidmann, D.; Kasperek, D.; Omer, M. Applicability of Agent-Based Modeling for Supporting Product-Service System Development. Procedia CIRP 2014, 16, 356–361. [Google Scholar] [CrossRef] [Green Version]
- Lättilä, L.; Hilletofth, P.; Lin, B. Hybrid Simulation Models—When, Why, How? Expert Syst. Appl. 2010, 37, 7969–7975. [Google Scholar] [CrossRef]
- Wang, B.; Brême, S.; Moon, Y.B. Hybrid Modeling and Simulation for Complementing Lifecycle Assessment. Comput. Ind. Eng. 2014, 69, 77–88. [Google Scholar] [CrossRef]
- Karnon, J.; Stahl, J.; Brennan, A.; Caro, J.J.; Mar, J.; Möller, J. Modeling Using Discrete Event Simulation: A Report of the ISPOR-SMDM Modeling Good Research Practices Task Force–4. Med. Decis. Mak. 2012, 32, 701–711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jalayer, M.; Orsenigo, C.; Vercellis, C. CoV-ABM: A Stochastic Discrete-Event Agent-Based Framework to Simulate Spatiotemporal Dynamics of COVID-19. arXiv Prepr. 2020, arXiv:2007.13231. [Google Scholar]
- Venkateswaran, J.; Damani, O. Effectiveness of Testing, Tracing, Social Distancing and Hygiene in Tackling Covid-19 in India: A System Dynamics Model. arXiv Prepr. 2020, arXiv:2004.08859. [Google Scholar]
- D’Orazio, M.; Bernardini, G.; Quagliarini, E. How to Restart? An Agent-Based Simulation Model towards the Definition of Strategies for COVID-19 “Second Phase” in Public Buildings. Build. Simul. 2021, 14, 1795–1809. [Google Scholar] [CrossRef]
- Sy, C.; Ching, P.M.; San Juan, J.L.; Bernardo, E.; Miguel, A.; Mayol, A.P.; Culaba, A.; Ubando, A.; Mutuc, J.E. Systems Dynamics Modeling of Pandemic Influenza for Strategic Policy Development: A Simulation-Based Analysis of the COVID-19 Case. Process. Integr. Optim. Sustain. 2021, 5, 461–474. [Google Scholar] [CrossRef]
- Bouchnita, A.; Jebrane, A. A Hybrid Multi-Scale Model of COVID-19 Transmission Dynamics to Assess the Potential of Non-Pharmaceutical Interventions. Chaos Solitons Fractals 2020, 138, 109941. [Google Scholar] [CrossRef]
- Garcia-Vicuña, D.; Esparza, L.; Mallor, F. Hospital Preparedness in Epidemics by Using Simulation. The Case of COVID-19. MedrXiv 2020. [Google Scholar] [CrossRef]
- Wood, R.M.; Pratt, A.C.; Kenward, C.; McWilliams, C.J.; Booton, R.D.; Thomas, M.J.; Bourdeaux, C.P.; Vasilakis, C. The Value of Triage during Periods of Intense COVID-19 Demand: Simulation Modeling Study. Med. Decis. Making 2021, 41, 393–407. [Google Scholar] [CrossRef]
- Law, A.; Kelton, W.D. Simulation Modeling and Analysis; McGraw-Hill Education: Boston, MA, USA, 1991; ISBN 978-0-07-116537-2. [Google Scholar]
- Ministero della Salute Nuovo Coronavirus. Available online: https://www.salute.gov.it/portale/nuovocoronavirus/homeNuovoCoronavirus.jsp (accessed on 27 May 2021).
- Kai, D.; Goldstein, G.-P.; Morgunov, A.; Nangalia, V.; Rotkirch, A. Universal Masking Is Urgent in the COVID-19 Pandemic: SEIR and Agent Based Models, Empirical Validation, Policy Recommendations. arXiv Prepr. 2020, arXiv:2004.13553. [Google Scholar]
- Silva, P.C.L.; Batista, P.V.C.; Lima, H.S.; Alves, M.A.; Guimarães, F.G.; Silva, R.C.P. COVID-ABS: An Agent-Based Model of COVID-19 Epidemic to Simulate Health and Economic Effects of Social Distancing Interventions. Chaos Solitons Fractals 2020, 139, 110088. [Google Scholar] [CrossRef]
- Simeone, G. Covid-19 e Immunità Post Infezione. Available online: https://www.ordinemedici.brescia.it/archivio10_notizie-e-comunicati_6_2043.html (accessed on 27 May 2021).
- Centers for Disease Control and Prevention Public Health Guidance for Community-Related Exposure. Available online: https://www.cdc.gov/coronavirus/2019-ncov/php/public-health-recommendations.html (accessed on 27 May 2021).
- Lelieveld, J.; Helleis, F.; Borrmann, S.; Cheng, Y.; Drewnick, F.; Haug, G.; Klimach, T.; Sciare, J.; Su, H.; Pöschl, U. Model Calculations of Aerosol Transmission and Infection Risk of COVID-19 in Indoor Environments. Int. J. Environ. Res. Public Health 2020, 17, 8114. [Google Scholar] [CrossRef]
- Istat Istat Lombardia. Available online: https://www.istat.it/it/uffici-territoriali/lombardia (accessed on 27 May 2021).
- Ministero della Salute Covid-19—Situazione Italia. Available online: https://opendatadpc.maps.arcgis.com/apps/dashboards/b0c68bce2cce478eaac82fe38d4138b1 (accessed on 29 May 2021).
- Epicentro Infografica Web—Dati Della Sorveglianza Integrata COVID-19 in Italia. Available online: https://www.epicentro.iss.it/coronavirus/sars-cov-2-dashboard (accessed on 27 May 2021).
- Elias, C.; Sekri, A.; Leblanc, P.; Cucherat, M.; Vanhems, P. The Incubation Period of COVID-19: A Meta-Analysis. Int. J. Infect. Dis. 2021, 104, 708–710. [Google Scholar] [CrossRef]
- Max Planck Institute Risk Calculator. Available online: https://www.mpic.de/4851094/risk-calculator (accessed on 24 June 2021).
- Law, A.M.; McComas, M.G. Secrets of Successful Simulation Studies. In Proceedings of the 23rd Conference on Winter Simulation, IEEE Computer Society, Washington, DC, USA, 8–11 December 1991; pp. 21–27. [Google Scholar]
- Montevechi, J.A.B.; Filho, R.G.D.A.; Paiva, A.P.; Costa, R.F.S.; Medeiros, A.L. Sensitivity Analysis in Discrete-Event Simulation Using Fractional Factorial Designs. J. Simul. 2010, 4, 128–142. [Google Scholar] [CrossRef]
- Montevechi, J.A.B.; Miranda, R.D.C.; Friend, J.D. Sensitivity Analysis in Discrete Event Simulation Using Design of Experiments; IntechOpen: London, UK, 2012; ISBN 978-953-51-0741-5. [Google Scholar]
- Asadi, S.; Cappa, C.D.; Barreda, S.; Wexler, A.S.; Bouvier, N.M.; Ristenpart, W.D. Efficacy of Masks and Face Coverings in Controlling Outward Aerosol Particle Emission from Expiratory Activities. Sci. Rep. 2020, 10, 15665. [Google Scholar] [CrossRef]
- World Health Organization Coronavirus Disease (COVID-19) Advice for the Public: When and How to Use Masks. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public/when-and-how-to-use-masks (accessed on 15 June 2021).
- Florida Atlantic University Stay 6 Feet Apart. Simulated Cough Reveals That May Not Be Enough. Available online: http://www.fau.edu/newsdesk/articles/mechanical-cough-coronavirus.php (accessed on 15 June 2021).
- Palmiero, A.J.; Symons, D.; Morgan, J.W.; Shaffer, R.E. Speech Intelligibility Assessment of Protective Facemasks and Air-Purifying Respirators. J. Occup. Environ. Hyg. 2016, 13, 960–968. [Google Scholar] [CrossRef]
- Chu, D.K.; Akl, E.A.; Duda, S.; Solo, K.; Yaacoub, S.; Schünemann, H.J.; Chu, D.K.; Akl, E.A.; El-harakeh, A.; Bognanni, A.; et al. Physical Distancing, Face Masks, and Eye Protection to Prevent Person-to-Person Transmission of SARS-CoV-2 and COVID-19: A Systematic Review and Meta-Analysis. Lancet 2020, 395, 1973–1987. [Google Scholar] [CrossRef]
- ISS ISS per COVID-19. Available online: https://www.iss.it/coronavirus (accessed on 15 June 2021).










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Paper ID | Title | Reference | Epidemic | Epidemiological Approach |
|---|---|---|---|---|
| 1 | Towards a comprehensive simulation model of malaria epidemiology and control | [6] | Malaria | EIR |
| 2 | A model simulation study on effects of intervention measures in Wuhan COVID-19 epidemic | [7] | Sars-CoV-2 | Ad hoc infection model |
| 3 | Mathematical Modeling of Epidemic Diseases; A Case Study of the COVID-19 Coronavirus | [8] | Sars-CoV-2 | SIR |
| 4 | Epidemic trend and transmission risk of SARS-CoV-2 after government intervention in the mainland of China: A mathematical model study | [9] | Sars-CoV-2 | SEIPQR |
| 5 | Parameter identification for a stochastic SEIRS epidemic model: case study influenza | [10] | Flu | SEIRS |
| 6 | Using simulation technology to analyze the COVID-19 epidemic in Changsha, Hunan Province, China | [11] | Sars-CoV-2 | SEIAR |
| 7 | An agent-Based Simulation of the Spread of Dengue Fever | [12] | Dengue fever | SEIR |
| 8 | Mathematical Modeling of the impact of Malaria Vaccines on the clinical epidemiology and natural history of Plasmodium falciparum malaria: overview | [13] | Malaria | EIR |
| 9 | Predictability and epidemic pathways in global outbreaks of infectious diseases: the SARS case study | [14] | SARS | SIR |
| 10 | Factors that make an infectious disease outbreak controllable | [15] | SARS | Ad hoc infection model |
| 11 | The effectiveness in Contact tracing in Emerging Epidemics | [16] | SARS | Ad hoc infection model (based on [15]) |
| 12 | Predictive models of control strategies involved in containing indoor airborne infections | [17] | SARS | Ad hoc infection model (partially based on [15]) |
| 13 | Timely identification of optimal control strategies for emerging infectious diseases | [18] | SARS | SEIR |
| 14 | Comparing nonpharmaceutical interventions for containing emerging epidemics | [19] | SARS & MERS | SEIR |
| Paper ID | Reference | Asymptomatic Transmission Ratio | Quarantine Delay | Isolation Delay | Quarantine Efficiency | Isolation Efficiency |
|---|---|---|---|---|---|---|
| 2 | [7] | Not Included | No | No | No | No |
| 3 | [8] | Included | Yes | Yes | Yes | Yes |
| 4 | [9] | Not Included | Yes | Yes | Yes | Yes |
| 6 | [11] | 11, 10% | No | Yes | No | Yes |
| 9 | [14] | Not Included | No | Yes | No | Yes |
| 10 | [15] | 11% | Yes | Yes | Yes | Yes |
| 11 | [16] | Not Included | No | Yes | No | No |
| 12 | [17] | 11% | Yes | No | Yes | No |
| 13 | [18] | Included | Yes | Yes | Yes | Yes |
| 14 | [19] | Included | Yes | Yes | No | Yes |
| Study | Simulation Technique | Objective | Aims | |||
|---|---|---|---|---|---|---|
| Model a Variety of Possible Individual Infection Phases/Interactions | Describe Inner Behavior Uncertainties for the Individual | Model Individual Actions and Organizational Processes in Time and Space | Monitor and Evaluate the Spread of the Contagion within Different Control Policies | |||
| [26] | ABM-DES-SD-HS | Suggesting the right simulation technique to support public health decision-making | N.A | N.A | N.A | N.A |
| [41] | ABM | Illustrating the dynamics of COVID diseases to identify places which have a higher probability to become infection hubs | X | X | ||
| [42] | SD | Simulating the COVID-19 spread in India | X | X | ||
| [43] | ABM | Evaluating the virus containment measures in closed environments | X | X | X | |
| [44] | SD | Evaluating the effectiveness of various policies in mitigating transmission and the resulting economic burden | X | X | ||
| [45] | HS (ABM-SD) | Evaluting the impact of social distancing measures and presymptomatic and surface transmission on the COVID spread. | X | X | X | |
| [46] | DES | Supporting short-term planning decisions about hospital resources utilization | X | |||
| [47] | DES | Understanding the triage efficacy in the intensive care admission and discharge dynamics | X | X | ||
| Variable | Domain/Unit | Definition |
|---|---|---|
| β—Contagion probability | 0–100% | The probability an individual can be infected while exposed |
| α—Initial exposed | 0–100% | The percentage of individuals who could be exposed at the starting of the simulation |
| γ—Initial infectors | 0–100% | The percentage of individuals who could be infectors at the starting of the simulation |
| δ—initial recovered | 0–100% | The percentage of individuals who could be recovered at the starting of the simulation |
| Variable | Value | Definition | Source |
|---|---|---|---|
| Contagiousness Index | 0.0029 | It defines the ratio of infected individuals; it is calculated as the number of positives/Total people in the population, considering the Lombardy Region and people aged 19–50 in February 2021. | [55,56] |
| Symptomatic ratio | 40% | Infected participants are divided into “Symptomatic” and “Latent” based on this parameter. | [57] |
| Incubation period | Normal Min: 2.33 days Max: 17.6 days Median: 5.41 days Mean: 6.38 days | It is the time from exposure to the causative agent until the first symptoms develop (from “Latent” to “Symptomatic” state). | [58] |
| Contagion probability | Triangular Min: 0, 11 Max: 0, 26 Mode: 0, 17 | It is the probability of being contaminated when in contact with an infected individual (transition from “healthy” to “contaminated” states). It has been calculated considering interpersonal distance equal to 2 m and a different Personal Protective Equipment (e.g., FFP1, FFP2, FFP3 masks). | [59] |
| Building | Classrooms | Max. Capacity | Allowed Capacity |
|---|---|---|---|
| Building A | 11 | 1,053 | 183 |
| Building B | 11 | 493 | 44 |
| Building C | 2 | 210 | 45 |
| Building D | 3 | 540 | 66 |
| Base Scenario: Contagiousness Index = 0.0029 | ||
|---|---|---|
| Run | Individuals Infected from Outside | Individuals Contaminated Inside |
| 1 | 0 | 0 |
| 2 | 4 | 0 |
| 3 | 3 | 0 |
| 4 | 3 | 0 |
| 5 | 1 | 1 |
| Mean | 2.2 | 0.2 |
| Validation Scenario: Contagiousness Index = 0.0046 | ||
|---|---|---|
| Run | Individuals Infected from Outside | Individuals Contaminated Inside |
| 1 | 5 | 3 |
| 2 | 1 | 0 |
| 3 | 4 | 0 |
| 4 | 5 | 0 |
| 5 | 4 | 0 |
| Mean | 3.8 | 0.3 |
| Scenario 1: Classroom Occupancy = 50% | ||
|---|---|---|
| Run | Individuals Infected from Outside | Individuals Contaminated Inside |
| 1 | 7 | 6 |
| 2 | 5 | 8 |
| 3 | 11 | 3 |
| 4 | 7 | 12 |
| 5 | 6 | 2 |
| Mean | 7.2 | 6 |
| Scenario 2: FFP2 Masks | ||
|---|---|---|
| Run | Individuals Infected from Outside | Individuals Contaminated Inside |
| 1 | 9 | 0 |
| 2 | 6 | 0 |
| 3 | 4 | 0 |
| 4 | 8 | 1 |
| 5 | 7 | 3 |
| Mean | 6.8 | 0.8 |
| Containment Measures | Example of Measures | Lessons Learned |
|---|---|---|
| Flow management | New path, break areas. Closing/opening community services (e.g., canteen, libraries, laboratories) | The paths and the area defined impact the safety distance among students. Introduction of fixed paths, regulation of access to break areas and closure of community services are resulted to be effective measures. |
| Number and schedule of inputs | Number of classes in presence | The limited number of classes in presence allows better management of flows and common spaces to keep the university safe. |
| Occupancy rate | Occupancy rate of classrooms | The increase in the occupancy rate must be carefully assessed considering the external epidemiological situation because it creates a multiplier effect in the spread of the infection. |
| PPE to be adopted | FFP2 vs. chirurgical mask adoption | The massive adoption of FFP2 is effective in counteracting the spread even when the number of students in presence increases. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cimini, C.; Pezzotta, G.; Lagorio, A.; Pirola, F.; Cavalieri, S. How Can Hybrid Simulation Support Organizations in Assessing COVID-19 Containment Measures? Healthcare 2021, 9, 1412. https://doi.org/10.3390/healthcare9111412
Cimini C, Pezzotta G, Lagorio A, Pirola F, Cavalieri S. How Can Hybrid Simulation Support Organizations in Assessing COVID-19 Containment Measures? Healthcare. 2021; 9(11):1412. https://doi.org/10.3390/healthcare9111412
Chicago/Turabian StyleCimini, Chiara, Giuditta Pezzotta, Alexandra Lagorio, Fabiana Pirola, and Sergio Cavalieri. 2021. "How Can Hybrid Simulation Support Organizations in Assessing COVID-19 Containment Measures?" Healthcare 9, no. 11: 1412. https://doi.org/10.3390/healthcare9111412