
Development and Effect of Virtual Reality Practice Program for Improving Practical Competency of Caregivers Specializing in Dementia

Abstract
:1. Introduction
1.1. Background
1.2. Study Purpose
- -
- Analyze the current curriculum of caregivers and analyze the actual educational needs through interviews.
- -
- Develop cases for improving the practical competency of caregivers in caring for dementia patients.
- -
- Implement virtual reality (VR) cases for improving the practical competency of caregivers in caring for dementia patients.
- -
- Conduct a pilot test to evaluate the effectiveness of a virtual reality (VR) practice program developed to enhance the practical competency of caregivers in caring for dementia patients.
2. Study Method
2.1. Study Design
2.2. Study Process
2.3. Virtual Reality Practice Program Development and Evaluation
2.3.1. Analysis
Analysis of the Current Situation: Analysis of Domestic Caregivers’ Training Courses
Target Needs Analysis: Investigation of Educational Needs for Caregivers
- Study subjects
- 2.
- Measurement
- 3.
- Result analysis
2.3.2. Design
Learning Goals and Topic Selection
2.3.3. Development
- Practice program case development: based on the topic selected by the analysis process, a case study program was developed.
- Expert validity: contents developed as a case study program were evaluated for content validity by experts, such as nursing professors and actual clinical practitioners, and the final virtual reality practice program case was developed based on this process.
- Virtual reality implementation of practice program example: the finally developed practical program was implemented through virtual reality.
2.3.4. Evaluation
3. Data Collection and Ethical Considerations
4. Result
4.1. Virtual Reality Practice Program Development
4.1.1. Analysis of Domestic Caregiver Training Courses
4.1.2. Analysis of Educational Needs for Caregivers
General Characteristics of Subjects
Content Analysis
Design
Development
- a.
- Case development of virtual reality practice program
- b.
- Expert validity: For the content validity of the virtual reality practice program developed in this study, content validity was performed with the following subjects: one medicine professor with dementia research experience, one occupational therapy professor, two nursing professors, and one long-term care facility head with experience in nursing dementia patients. As a result, feedback on program time and gender of virtual reality characters was reflected and completed.
- c.
- Case virtual reality implementation
- d.
- Evaluation of the effectiveness of Korean-style virtual reality practice program
5. Discussion
6. Conclusions and Implication
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
- Topic setting and situation introduction.
- (1)
- Target: caregivers caring for dementia patients.
- (2)
- Subject: mental behavioral symptoms of dementia patients (aggressive behavior due to delusions).
- (3)
- Place of practice: researcher’s lab (Room 506, K University).
- (4)
- Learning Goals
- -
- Explain the definition of psycho-behavioral symptoms in dementia patients.
- -
- It is possible to understand aggressive behavior among the psycho-behavioral symptoms of dementia patients.
- -
- Among the psycho-behavioral symptoms of dementia patients, it is possible to explain how to cope with aggressive behavior.
- (5)
- Preparations: HMD (Head Mount Display), PC.
- Situation Introduction
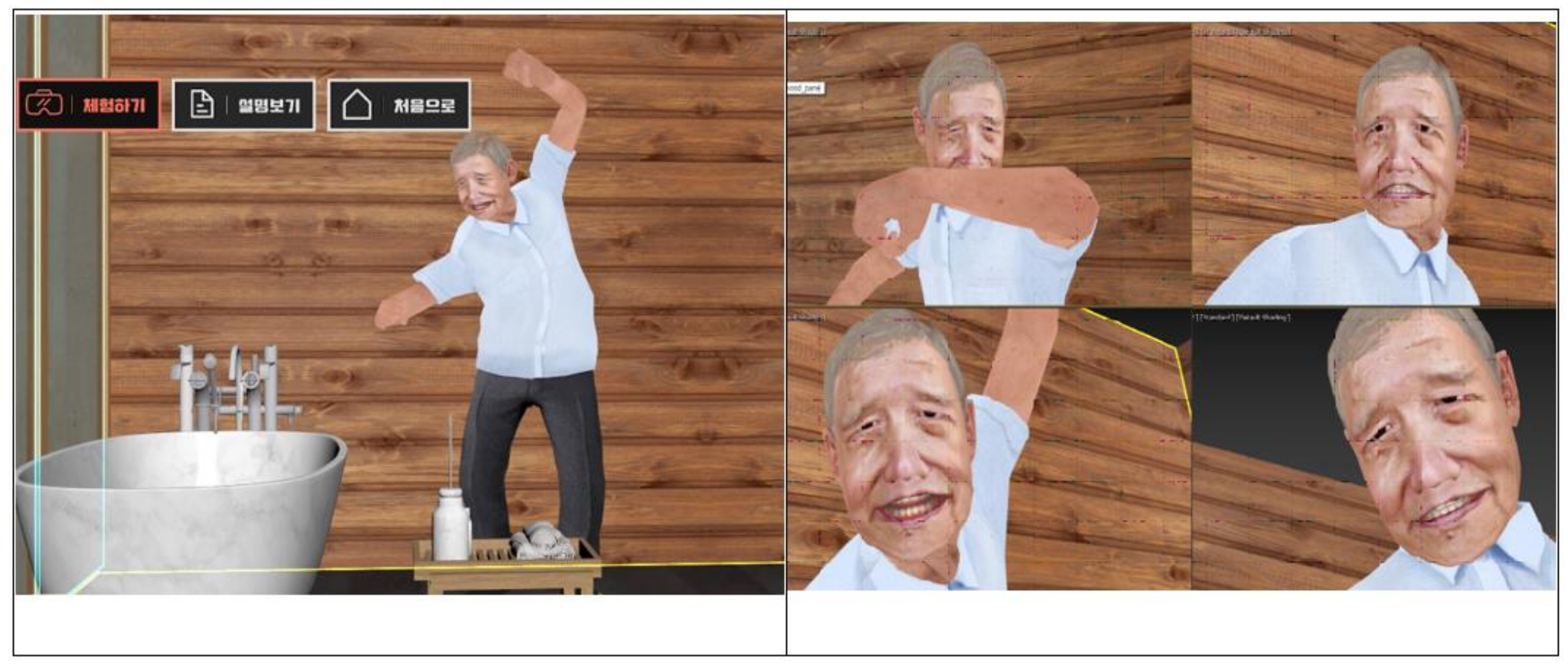
- 3.
- Virtual reality implementation image.
References
- Ministry of Health and Welfare. LivinG HAPPILY in our NEIGHBORHood with Dementia. (Study on the Third Dementia Management Comprehensive Plan (2016–2020). Available online: http://www.mohw.go.kr/ (accessed on 20 May 2021).
- Ministry of Health and Welfare. A Study on the Prevalence of Dementia in 2012. Available online: http://www.mohw.go.kr/react/al/sal0301vw.jsp?PAR_MENU_ID=04&MENU_ID=0403&CONT_SEQ=286138&page=1 (accessed on 20 May 2021).
- Ministry of Health and Welfare. A Study on the Activation of Dementia Management and Rehabilitation Services. Available online: http://www.mohw.go.kr/react/al/sal0301vw.jsp?PAR_MENU_ID=04&MENU_ID=0403&CONT_SEQ=215558&page=607 (accessed on 20 May 2021).
- Korean Statistical Information Service. The Number of Welfare Living Facilities for the Elderly and the Current Status of Living. Available online: https://kosis.kr/statHtml/statHtml.do?orgId=117&tblId=DT_117N_B00003 (accessed on 20 May 2021).
- Korean Statistical Information Service. Status of Long-Term Care Institutions by City and Province Salary Type by Year. Available online: http://kosis.kr/statHtml/statHtml.do?orgId=350&tblId=DT_35006_N019 (accessed on 20 May 2021).
- Ministry of Health and Welfare. Determination of the Number of New and Adjusted and Insurance Premium Rates Following the Reorganization of the Long-Term Care Insurance Rating System, Such as the Establishment of a Special Grade for Dementia. Available online: http://www.mohw.go.kr/react/al/sal0301vw.jsp?CONT_SEQ=300388&MENU_ID=0403&PAR_MENU_ID=04&page=1 (accessed on 20 May 2021).
- Korea Ministry of Government Legislation. Welfare of Older Persons Act. Article 39 and 2. Available online: https://www.law.go.kr/%EB%B2%95%EB%A0%B9/%EB%85%B8%EC%9D%B8%EB%B3%B5%EC%A7%80%EB%B2%95/(16243,20190115) (accessed on 20 May 2021).
- Korea Care Associaion. Curriculum. Available online: http://www.silvercare.org/edu/yoyang.asp?BID=yoyang2 (accessed on 10 May 2021).
- Lee, Y.J.; Park, K.H. Influencing Factors on Service Quality of Care Helpers Working or the Elderly in Long Term Care. Korean Acad. Soc. Occup. Health Nurs. 2012, 21, 145–217. [Google Scholar]
- Ha, E.H.; Cho, J.Y. Analysis of Knowledge About, Attitude Toward, and Educational Needs for Dementia in Certified Caregivers. J. Korean Acad. Soc. Nurs. Educ. 2015, 21, 108–118. [Google Scholar] [CrossRef] [Green Version]
- Kong, E.H. The effects of dementia education program on certified getriatric caregivers in a nursing hom. J. Korean Acad. Psychiatric Mental Health Nurs. 2010, 19, 349–358. [Google Scholar] [CrossRef] [Green Version]
- Elo, S.; Kyngäs, H. The qualitative content analysis process. J. Adv. Nurs. 2008, 62, 107–115. [Google Scholar] [CrossRef]
- Krippendorff, K. Content Analysis: An Introduction to its Methodology; Sage: Beverly Hills, CA, USA, 2004. [Google Scholar]
- Dey, I. Qualitative Data Analysis: A User-Friendly Guide for Social Scientists; Routledge: London, UK, 1993. [Google Scholar]
- Hyoung, H.K.; Ju, Y.S.; Im, S.I. A concept mapping study on clinical stress for nursing students during clinical practice. J. Korean Acad. Nurs. Adm. 2014, 20, 394–404. [Google Scholar] [CrossRef] [Green Version]
- Lee, A.K. Influencing Factors of Nursing Students in Clinical Practice Stress. Master’s Thesis, Chonnam National University, Gwangju, Korea, 2013. [Google Scholar]
- Hong, S.S.; Hong, J.A.; Jun, W.H. Spirituality and stress of clinical practice among nursing students. J. Korean Cont. Assoc. 2013, 13, 361–369. [Google Scholar] [CrossRef] [Green Version]
- Arai, Y.; Kumamoto, K.; Washio, M.; Ueda, T.; Miura, H.; Kudo, K. Factors related to feelings of burden among caregivers looking after impaired elderly in Japan under the Long-Term Care insurance system. Psychiatry Clin. Neurosci. 2004, 58, 396–402. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Kang, M.H.; Kim, C.E.; Lee, J.S.; Bae, J.N. The Relationship between Psychopathology of Demented Elderly People and Caregiver. J. Korean Neuropaychiatr. Assoc. 2003, 42, 131–140. [Google Scholar]
- Park, M.H.; Go, Y.H.; Jeong, M.R.; Lee, S.G.; Kim, S.H.; Kim, J.H.; Lee, D.Y. Influencing factors and risk of caregiver burden of family caregivers for patient with dementia. Kor. J. Family Welfare 2017, 22, 431–448. [Google Scholar] [CrossRef]
- Yoon, S.W.; Ryu, S.A. Impact of Dementia Knowledge, Burden from Behavioral Psychological Symptoms of Dementia and Empathy in the Caring Behavior of Certified Caregivers in Nursing Homes. Korean J. Res. Gerontolog. 2015, 17, 131–141. [Google Scholar] [CrossRef] [Green Version]
- Cho, C.Y. A study on securing professionalism of caregivers in long-term care insurance system for the elderly. Korean J. Res. Gerontolog. 2007, 16, 9–40. [Google Scholar]
- Seo, E.J.; Kim, S.Y. Workplace Violence Experiences among Care Helpers. Kor. Acad. Soc. Adult Nurs. 2012, 24, 607–614. [Google Scholar] [CrossRef] [Green Version]
- Ahn, I.S.; Kim, J.H.; Jung, H.M.; Kim, D.K. The Study of Factors Related to Care Burden of Caregivers in Patients with Dementia. J. Korean Neuropsychiatry Assoc. 2005, 44, 505–510. [Google Scholar]
- Shaji, K.S.; George, R.K.; Prince, M.J.; Jacob, K.S. Behavioral symptoms and caregiver burden in dementia. Ind. J. Psychiatry 2009, 51, 45–49. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H. A study on the revitalization of virtual reality-based education. J. Korean Soc. Design Cult. 2019, 25, 358–366. [Google Scholar]
- Ironside, P.M.; McNelis, A.M.; Ebright, P. Clinical education in nursing: Rethinking learning in practice settings. Nurs. Outlook 2014, 62, 185–191. [Google Scholar] [CrossRef]
- Dubovi, I.; Levy, S.T.; Dagan, E. Now I know how! The learning process of medication administration among nursing students with non-immersive desktop virtual reality simulation. Comput. Educ. 2017, 113, 16–27. [Google Scholar] [CrossRef]
- McCallum, J.; Ness, V.; Price, T. Exploring nursing students’ decision-making skills whilst in a Second Life clinical simulation laboratory. Nurs. Educ. Today 2011, 31, 699–704. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.M.; Yeom, Y.R. The effect of education integrating virtual reality simulation training and outside school clinical practice for nursing students. J. Converg. Inf. Technol. 2020, 10, 100–108. [Google Scholar]
- Kim, P.H.; Kim, K.N. A phenomenological study to the simulation class of adult nursing students. Asia Pacif. J. Multimed. Serv. Converg. Art Human. Soc. 2018, 8, 541–550. [Google Scholar]
- Kilmon, C.A.; Brown, L.; Ghosh, S.; Mikitiuk, A. Immersive virtual reality simulations in nursing education. Nurs. Educ. Perspect. 2010, 3, 314–317. [Google Scholar]
- Cant, R.P.; Cooper, S.J. Simulation in the Internet age: The place of web-based simulation in nursing education. An integrative review. Nurs. Educ. Today 2014, 34, 1435–1442. [Google Scholar] [CrossRef] [PubMed]
- Ulrich, D.; Farra, S.; Smith, S.; Hodgson, E. The Student Experience Using Virtual Reality Simulation to Teach Decontamination. Clin. Simul. Nurs. 2014, 10, 546–553. [Google Scholar] [CrossRef]
- Koivisto, J.M.; Niemi, H.; Multisilta, J.; Eriksson, E. Nursing students’ experiential learning processes using an online 3D simulation gam. Educ. Inf. Technol. 2017, 22, 383–398. [Google Scholar] [CrossRef]
- Guna, J.; Geršak, G.; Humar, I.; Song, J.; Drnovšek, J.; Pogacnik, M. Influence of video content type on users’ virtual reality sickness perception and physiological response. Future Gener. Comput. Syst. 2019, 91, 263–276. [Google Scholar] [CrossRef]
- Somrak, A.; Pogacnik, M.; Guna, J. Suitability and Comparison of Questionnaires Assessing Virtual Reality-Induced Symptoms and Effects and User Experience in Virtual Environments. Sensors 2021, 21, 1185. [Google Scholar] [CrossRef]
- Choi, S.H.; Won, J.S. The nature of flow in virtual reality education: Based on a grounded theory approach. J. Korean Cont. Assoc. 2017, 17, 446–460. [Google Scholar]
- Kourtesis, P.; Korre, D.; Collina, S.; Doumas, L.A.; MacPherson, S.E. Guidelines for the development of immersive virtual reality software for cognitive neuroscience and neuropsychology: The development of virtual reality everyday assessment lab (VR-EAL), a neuropsychological test battery in immersive virtual reality. Front. Comput. Sci. 2020, 1, 1–24. [Google Scholar] [CrossRef] [Green Version]
- Moreau, D.; Conway, A.R. The case for an ecological approach to cognitive training. Trends Cognit. Sci. 2014, 18, 334–336. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Type | Subject | Education | Contents | Theory | Practical |
|---|---|---|---|---|---|
| Theory Lecture (80 h)/ Practical Practice (80 h) | Nursing Care Introduction | Nursing Care Related Systems and Services |
| 5 | |
| Purpose and Function of Nursing Care Work |
| 2 | |||
| Caregiver Professional Ethics and Attitude |
| 8 | 6 | ||
| Understanding Nursing Care Recipients |
| 2 | |||
| Nursing Care Basic Knowledge | Medical Nursing Basic Knowledge |
| 12 | 3 | |
| Nursing Care Particular | Basic Nursing Care Technology(Ingestion, Excretion, Hygiene, Movement, Safety) |
| 4 | 6 | |
| 5 | 8 | |||
| 5 | 8 | |||
| 6 | 8 | |||
| 3 | 6 | |||
| Housework and Daily LifeSupport |
| 4 | 6 | ||
| Communication and Leisure Support |
| 5 | 6 | ||
| Service Support for Use |
| 3 | 4 | ||
| Nursing Care Work Record Report |
| 3 | 4 | ||
| Special Nursing Care Particular | Dementia Care Technology |
| 6 | 6 | |
| End-Of-Life/Hospice Care |
| 3 | 3 | ||
| First Aid Technology |
| 4 | 6 | ||
| Field Practice (80 h) | Elderly Care Facility Practice | Integrated Practice I | 40 | ||
| Home Care Service Practice | Integrated Practice II | 40 | |||
| Type | Category | Meaningful Content |
|---|---|---|
| Psychological symptoms | Delusion | I (patient) have to go find the man who had an affair with my wife (delusional jealousy of wife or husband). They (caregivers) told me to go on drugs (cups) to die quickly. Controversy over stealing a pension passbook and other passbooks. |
| Suspicion | Stole my money. I (patient) suspect that if you(caregiver) open the closet to change clothes, you will search through them. I (patient) continue to doubt the caregiver, saying who took what every day. Items that are missing from the kitchen are often taken by the caregiver who sees them. Suspicion, often stating that things are lost (almost every day). | |
| Anxiety, Nervousness | Call every 2 min. Until I (patient) go to sleep, I try not to fall off, so I’m just afraid of being alone. When the patient screams for me to take him and follows me to the end. | |
| Behavioral Symptom | Aggression | I (caregiver) feel mentally anxious and tired (suddenly attack). Physically dangerous, fearful when providing care. When yelling and holding a cane. Since there are only two patients and guardians in the house, there is no way to stop an attack (fear). |
| Hallucination | Auditory hallucinations (imitation)/visual hallucinations: saying that things that are not constantly appear to exist. He (patient) beats the whole house with a long stick and weeps, saying that he can see the faces of his dead relatives. Talking to an invisible object and doing what the invisible object tells you. Shouting out saying somebody here to kill me. The act of screaming for help. | |
| Swearing/ Wandering | Cursed, but still hard to ignore the personality of the patient. Repeatedly using verbal violence and saying that he would be willing to kill. Same time wandering/hallucinations keep trying to get out. Behavior that disappears quickly (trying to get out). | |
| Repetitive behavior | Repeating the same question multiple times. Same words (inappropriate behavior) throughout 2 h of service every day. Repeat the same words every day (name). | |
| Etc. | Excretion: discard anywhere in the feces/touching feces with your hands. Refusal to bathe: refusal to take a bath even though the visible hands and feet are blackened. Sleep disorder: I (patient) can’t sleep at night and I wake up constantly (every 2 h) to urinate. Sexual behavior: embarrassed by rude jokes and actions. |
| Type | Category | Meaningful Content |
|---|---|---|
| Knowledge (Theory) | Dementia related knowledge | Without knowledge (theoretical education), mentally problematic behavior cannot be understood and properly performed. It is also necessary to understand hospital prescription drugs (dementia patients) (when I actually took care of them). Dementia specialist programs are considered necessary on a regular basis. I want the country to have a system in which all working people must receive dementia education. Understanding dementia patients (understanding dementia disease). Symptoms and characteristics of dementia patients by stage. Appropriate drug treatment. What are the psychiatric behaviors of dementia? |
| Understanding dementia caregivers | Explaining the condition of the dementia patient to the caregiver. How to communicate with caregivers (how to deal with emotions). Talking and discussing care with the caregiver. | |
| Self-management education for caregivers with dementia | Self-management rather than knowledge (mental strengthening education to caregivers). Giving time to someone caring for someone with dementia (self-help group). How to share other people’s stories. How to deal with depression caused by caring for patients for a long time. How to manage sudden anger. How to be patient (requires a lot of patience). How to be professional, not compassionate. | |
| Practice (Training) | Implementation of dementia prevention management program | Cognitive stimulation activity program to maintain and enhance cognitive function. How to play according to the condition and level of dementia patients. Information that slows the progression of dementia patients (play, activity). Rhythms or recreational movements that increase concentration or enjoyment. Exercise program to maintain residual function, nutrition management. |
| Daily life care for dementia patients | Tips for changing diapers (difficult because the body is too big). Changing diapers when urinating, worrying about falls, difficult to do alone. Persuasion and understanding process for dementia patients (I want to see the process of persuasion actually). Bathing skills (rejection, risk of falls). Bedsore management, bath problems, meals, etc. | |
| How to take care of dementia patients | Caring for emergencies (response)/I am embarrassed and nervous about an emergency. How to deal with problem behavior (aggression, profanity). A variety of case-based education that can be used in case of emergency. How to respond when an elderly person finds a missing item. Due to the expansion of knowledge, it is necessary to conduct coping method education in theoretical education. Practical practice is required for each coping method according to the type of dementia. Skills to communicate with people with dementia. |
| Program Title | Korean-Style Virtual Reality Practice Program for Improving Core Practical Competencies of Caregivers | |||
|---|---|---|---|---|
| Program Purpose | The purpose of this program is to lower the burden of caring for caregivers taking care of dementia patients, and to improve the quality of care for dementia patients by understanding aggressive behavior among the mental behavioral symptoms of dementia patients and performing coping methods. | |||
| Program schedule | This program is a pilot test according to the development of a Korean-style virtual reality practice program for the improvement of core practical competencies of caregivers. The program will take about 70 min (60 min of program, 10 min of break time). | |||
| Time | Topic | Educational goals | Contents | Method |
| 10 min | Program introduction | Introduction of program schedule and progress. Pre-investigation (general characteristics, experience of caring for dementia patients). | Self introduction Pre-investigation | |
| 15 min | Understanding the psycho-behavioral symptoms of dementia patients | Explain the definition of psycho-behavioral symptoms in dementia patients. | Definition of psycho-behavioral symptoms in dementia patients. Types of psycho-behavioral symptoms in dementia patients. | Lecture |
| 5 min | Conduct virtual reality practice | To understand the psycho-behavioral symptoms of dementia patients. | One of the mental behavioral symptoms of dementia patients, aggression due to hallucinations, can be directly experienced through virtual reality implementation practice from the perspective of dementia patients. | Lectures and Practice |
| 10 min | Cases of mental behavior in dementia patients | Coping methods for psycho-behavioral symptoms of dementia patients can be performed. | Sharing of cases and experiences of psycho-behavioral symptoms that occur in actual caring of dementia patients. | Discussion |
| 10 min | Coping with psycho-behavioral symptoms of dementia patients | Educating and sharing experiences on how to cope with the psycho-behavioral symptoms of dementia patients. | Discussion and Lecture | |
| 10 min | Program summary | Program satisfaction survey (survey, interview). | Post test Group interview | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, D. Development and Effect of Virtual Reality Practice Program for Improving Practical Competency of Caregivers Specializing in Dementia. Healthcare 2021, 9, 1390. https://doi.org/10.3390/healthcare9101390
Kim D. Development and Effect of Virtual Reality Practice Program for Improving Practical Competency of Caregivers Specializing in Dementia. Healthcare. 2021; 9(10):1390. https://doi.org/10.3390/healthcare9101390
Chicago/Turabian StyleKim, Dooree. 2021. "Development and Effect of Virtual Reality Practice Program for Improving Practical Competency of Caregivers Specializing in Dementia" Healthcare 9, no. 10: 1390. https://doi.org/10.3390/healthcare9101390