
Risk Factors and Outcomes of Heart Failure Following First-Episode of Acute Myocardial Infarction—A Case Series Study of 161,384 Cases

Abstract
:1. Introduction
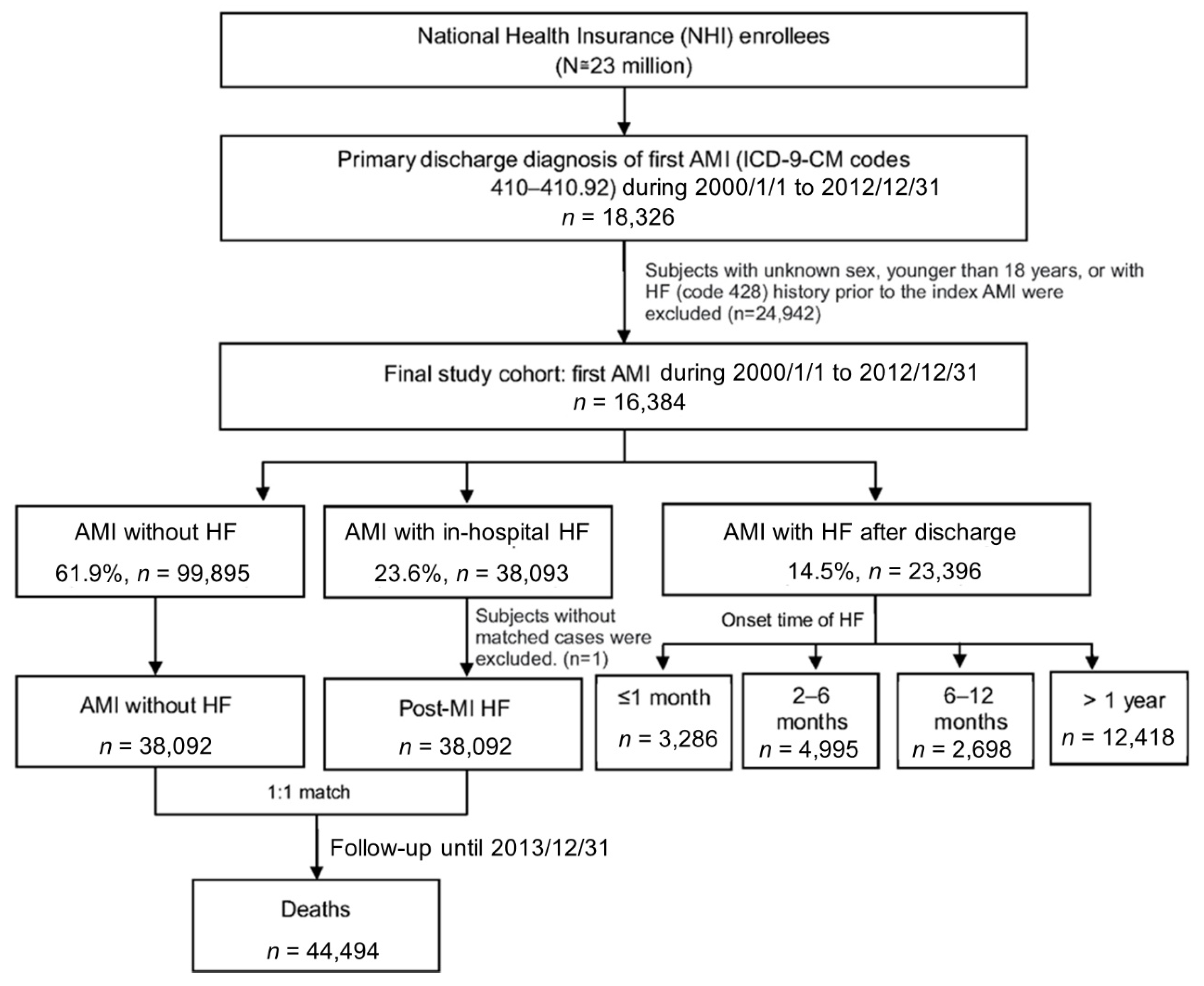
2. Materials and Methods
Statistical Analysis
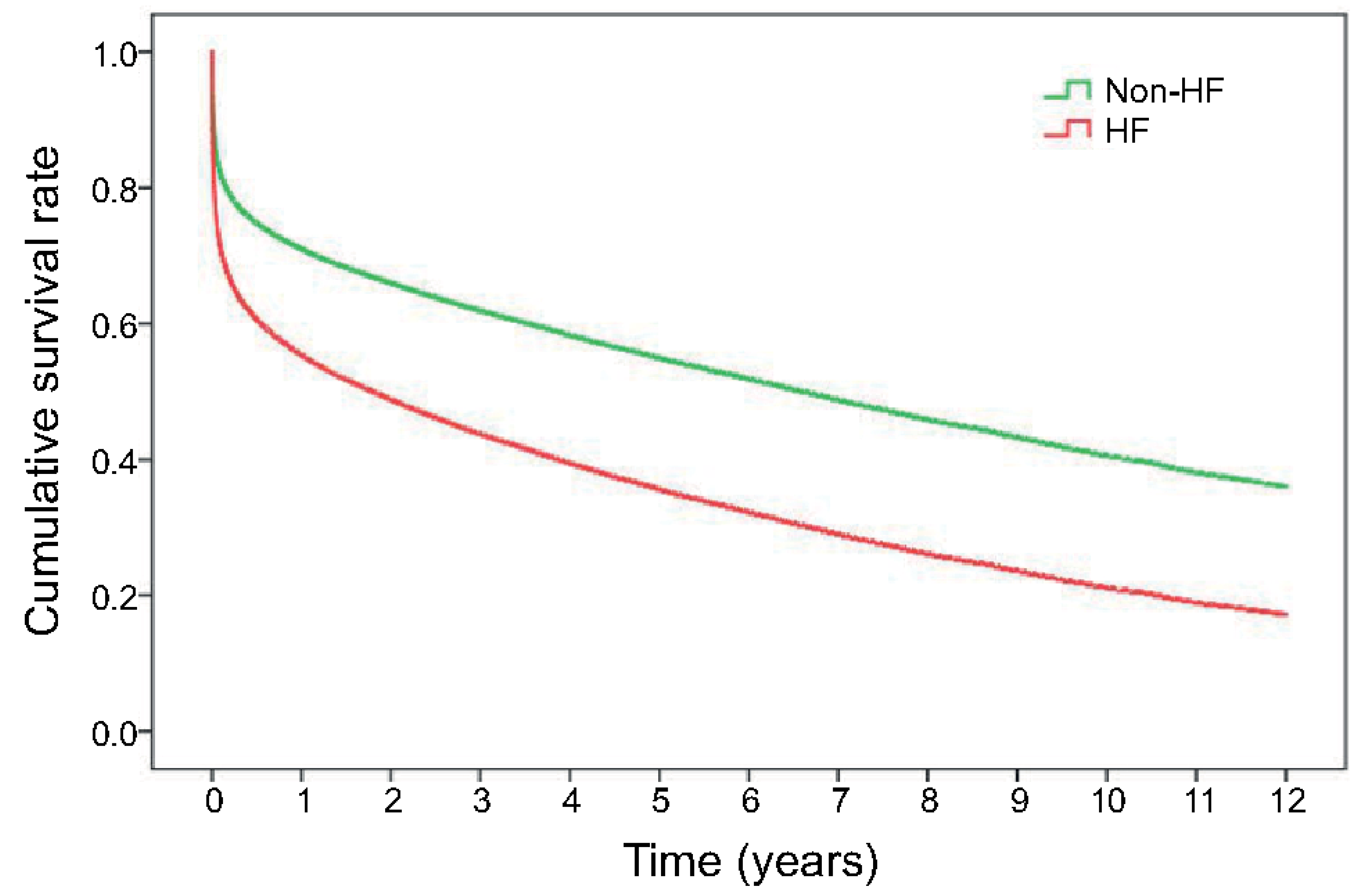
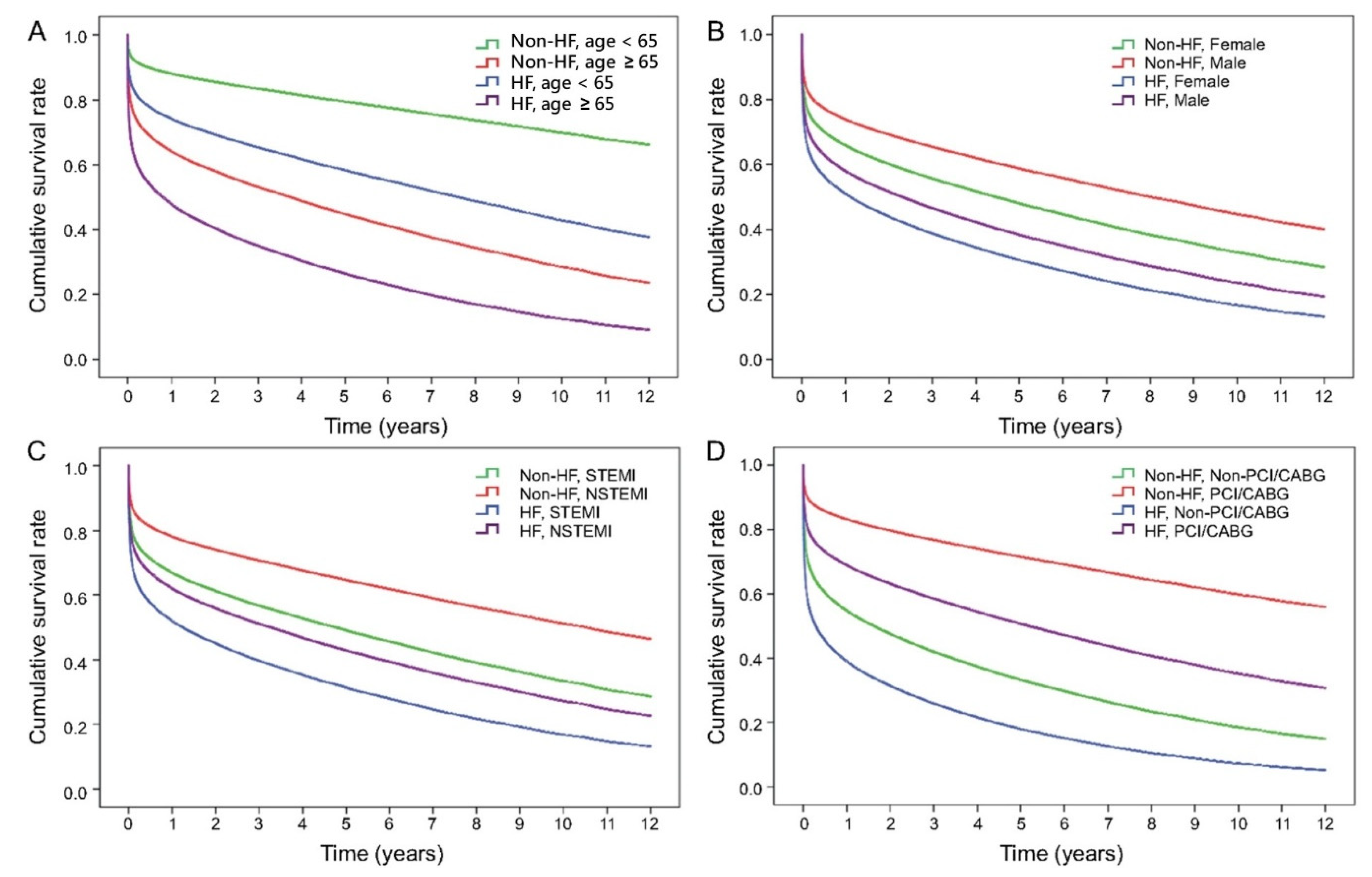
3. Results
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
List of Abbreviations
| ACEI/ARB | Angiotensin-converting enzyme inhibitors/angiotensin II receptor blockers |
| AMI | acute myocardial infarction |
| CABG | coronary artery bypass graft |
| HF | heart failure |
| NHIRD | National Health Insurance Research Database |
| PCI | percutaneous coronary intervention |
| NSTEMI | Non-ST elevation myocardial infarction |
| STEMI | ST elevation myocardial infarction |
| VT/VF | ventricular tachycardia/ventricular flutter |
References
- Johansson, S.; Rosengren, A.; Young, K.; Jennings, E. Mortality and morbidity trends after the first year in survivors of acute myocardial infarction: A systematic review. BMC Cardiovasc. Disord. 2017, 17, 53. [Google Scholar] [CrossRef] [Green Version]
- Tung, Y.C.; Chang, G.M.; Chang, H.Y.; Yu, T.-H. Relationship between early physician follow-up and 30-day readmission after acute myocardial infarction and heart failure. PLoS ONE 2017, 12, e0170061. [Google Scholar]
- Choi, H.; Seo, J.Y.; Shin, J.; Choi, B.Y.; Kim, Y.M. A long-term incidence of heart failure and predictors following newly developed acute myocardial infarction: A 10 Years retrospective cohort study with Korean National Health Insurance Data. Int. J. Environ. Res. Public Health 2021, 18, 6207. [Google Scholar] [CrossRef]
- Desta, L.; Jernberg, T.; Lofman, I.; Hofman-Bang, C.; Hagerman, I.; Spaak, J.; Persson, H. Incidence, temporal trends, and prognostic impact of heart failure complicating acute myocardial infarction. The SWEDEHEART Registry (Swedish Web-System for Enhancement and Development of Evidence-Based Care in Heart Disease Evaluated According to Recommended Therapies): A study of 199,851 patients admitted with index acute myocardial infarctions, 1996 to 2008. JACC Heart Fail. 2015, 3, 234–242. [Google Scholar]
- Sulo, G.; Igland, J.; Vollset, S.E.; Nygard, O.; Ebbing, M.; Sulo, E.; Egeland, G.M.; Tell, G.S. Heart Failure Complicating Acute Myocardial Infarction; Burden and Timing of Occurrence: A nation-wide analysis including 86,771 patients from the Cardiovascular Disease in Norway (CVDNOR) Project. J. Am. Heart Assoc. 2016, 5, e002667. [Google Scholar] [CrossRef] [Green Version]
- Santoro, G.M.; Carrabba, N.; Migliorini, A.; Parodi, G.; Valenti, R. Acute heart failure in patients with acute myocardial infarction treated with primary percutaneous coronary intervention. Eur. J. Heart Fail. 2008, 10, 780–785. [Google Scholar] [CrossRef] [PubMed]
- Cenko, E.; van der Schaar, M.; Yoon, J.; Manfrini, O.; Vasiljevic, Z.; Vavlukis, M.; Kedev, S.; Miličić, D.; Badimon, L.; Bugiardini, R. sex-related differences in heart failure after ST-segment elevation myocardial infarction. J. Am. Coll. Cardiol. 2019, 74, 2379–2389. [Google Scholar] [CrossRef]
- Otten, A.M.; Maas, A.H.; Ottervanger, J.P.; Kloosterman, A.; van’t Hof, A.W.; Dambrink, J.H.E.; Gosselink, A.M.; Hoorntje, J.C.; Suryapranata, H.; de Boer, M.J.; et al. Is the difference in outcome between men and women treated by primary percutaneous coronary intervention age dependent? Gender difference in STEMI stratified on age. Eur. Heart J. Acute Cardiovasc. Care 2013, 2, 334–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bulluck, H.; Zheng, H.; Chan, M.Y.; Foin, N.; Foo, D.C.; Lee, C.W.; Lim, S.T.; Sahlen, A.; Tan, H.C.; Tan, J.W.; et al. Independent predictors of cardiac mortality and hospitalization for heart failure in a multi-ethnic Asian ST-segment elevation myocardial infarction population treated by primary percutaneous coronary intervention. Sci. Rep. 2019, 9, 10072. [Google Scholar] [CrossRef] [PubMed]
- Kaul, P.; Ezekowitz, J.A.; Armstrong, P.W.; Leung, B.K.; Savu, A.; Welsh, R.C.; Quan, H.; Knudtson, M.L.; McAlister, F. Incidence of heart failure and mortality after acute coronary syndromes. Am. Heart J. 2013, 165, 379–385.e2. [Google Scholar] [CrossRef] [PubMed]
- Persson, H.; Linder-Klingsell, E.; Eriksson, S.V.; Erhardt, L. Heart failure after myocardial infarction: The importance of diastolic dysfunction. A prospective clinical and echocardiographic study. Eur. Heart J. 1995, 16, 496–505. [Google Scholar] [CrossRef] [PubMed]
- Beygui, F.; Cayla, G.; Roule, V.; Roubille, F.; Delarche, N.; Silvain, J.; Van Belle, E.; Belle, L.; Galinier, M.; Motreff, P.; et al. Early aldosterone blockade in acute myocardial infarction: The ALBATROSS randomized clinical trial. J. Am. Coll. Cardiol. 2016, 67, 1917–1927. [Google Scholar] [CrossRef] [PubMed]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [PubMed] [Green Version]
- DeBoer, L.; Rude, R.E.; Kloner, R.A.; Ingwall, J.S.; Maroko, P.R.; Davis, M.A.; Braunwald, E. A flow-and time-dependent index of ischemic injury after experimental coronary occlusion and reperfusion. Proc. Natl. Acad. Sci. USA 1983, 80, 5784–5788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaper, J.; Schaper, W. Reperfusion of ischemic myocardium: Ultrastructural and histochemical aspects. J. Am. Coll. Cardiol. 1983, 1, 1037–1046. [Google Scholar] [CrossRef]
- Bernier, M.; Curtis, M.J.; Hearse, D.J. Ischemia-induced and reperfusion-induced arrhythmias: Importance of heart rate. Am. J. Physiol. Heart Circ. Physiol. 1989, 256, H21–H31. [Google Scholar] [CrossRef] [PubMed]
- Tosaki, A.; Braquet, P. DMPO and reperfusion injury: Arrhythmia, heart function, electron spin resonance, and nuclear magnetic resonance studies in isolated working guinea pig hearts. Am. Heart J. 1990, 120, 819–830. [Google Scholar] [CrossRef]
- Tosaki, A.; Blasig, I.E.; Pali, T.; Ebert, B. Heart protection and radical trapping by DMPO during reperfusion in isolated working rat hearts. Free Radic. Biol. Med. 1990, 8, 363–372. [Google Scholar] [CrossRef]
- Kloner, R.A.; Braunwald, E. Observations on experimental myocardial ischaemia. Cardiovasc. Res. 1980, 14, 371–395. [Google Scholar] [CrossRef]
- Goldberg, S.; Greenspon, A.J.; Urban, P.L.; Muza, B.; Berger, B.; Walinsky, P.; Maroko, P.R. Reperfusion arrhythmia: A marker of restoration of antegrade flow during intracoronary thrombolysis for acute myocardial infarction. Am. Heart J. 1983, 105, 26–32. [Google Scholar] [CrossRef]
- Kloner, R.A.; Przyklenk, K.; Whittaker, P. Deleterious effects of oxygen radicals in ischemia/reperfusion. Resolved and unresolved issues. Circulation 1989, 80, 1115–1127. [Google Scholar] [CrossRef] [Green Version]
- Pearl, J.M.; Drinkwater, D.C., Jr.; Laks, H.; Stein, D.G.; Capouya, E.R.; Bhuta, S. Leukocyte-depleted reperfusion of transplanted human hearts prevents ultrastructural evidence of reperfusion injury. J. Surg. Res. 1992, 52, 298–308. [Google Scholar] [CrossRef]
- Forman, M.B.; Ingram, D.A.; Murray, J.J. Role of perfluorochemical emulsions in the treatment of myocardial reperfusion injury. Am. Heart J. 1992, 124, 1347–1357. [Google Scholar] [CrossRef]
- Kloner, R.A. Does reperfusion injury exist in humans? J. Am. Coll. Cardiol. 1993, 21, 537–545. [Google Scholar] [CrossRef]
- Salerno, T.; Chiong, M.; Neilson, I.; Charrette, E. Cardioplegic rearrest: Clinical experience with 12 patients. Can. J. Plast Surg. 1981, 24, 649–650, 655. [Google Scholar]
- Verma, S.; Fedak, P.W.; Weisel, R.D.; Butany, J.; Rao, V.; Maitland, A.; Li, R.K.; Dhillon, B.; Yau, T.M. Fundamentals of reperfusion injury for the clinical cardiologist. Circulation 2002, 105, 2332–2336. [Google Scholar] [CrossRef]
- Turer, A.T.; Hill, J.A. Pathogenesis of myocardial ischemia-reperfusion injury and rationale for therapy. Am. J. Cardiol. 2010, 106, 360–368. [Google Scholar] [CrossRef] [Green Version]
- Jenča, D.; Melenovský, V.; Stehlik, J.; Staněk, V.; Kettner, J.; Kautzner, J.; Adámková, V.; Wohlfahrt, P. Heart failure after myocardial infarction: Incidence and predictors. ESC Heart Fail. 2021, 8, 222–237. [Google Scholar] [CrossRef] [PubMed]
- Gerber, Y.; Weston, S.A.; Enriquez-Sarano, M.; Berardi, C.; Chamberlain, A.M.; Manemann, S.M.; Jiang, R.; Dunlay, S.M.; Roger, V.L. Mortality associated with heart failure after myocardial infarction: A contemporary community perspective. Circ. Heart Fail. 2016, 9, e002460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewis, E.F.; Moye, L.A.; Rouleau, J.L.; Sacks, F.M.; Arnold, J.M.; Warnica, J.W.; Flaker, G.C.; Braunwald, E.; Pfeffer, M.A. Predictors of late development of heart failure in stable survivors of myocardial infarction: The CARE study. J. Am. Coll. Cardiol. 2003, 42, 1446–1453. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| No HF (n = 99,895) | HF (in Hospital) (n = 38,092) | OR | 95% CI | p Value | |||
|---|---|---|---|---|---|---|---|
| Variables | n | (%) | n | (%) | |||
| Sex | <0.0001 | ||||||
| Male | 74,491 | (74.57) | 24,097 | (63.26) | 1.00 | — | |
| Female | 25,404 | (25.43) | 13,486 | (35.40) | 1.64 | (1.59–1.69) | |
| Age | <0.0001 | ||||||
| <65 | 49,404 | (49.46) | 11,310 | (29.69) | 1.00 | — | |
| ≥65 years old | 50,491 | (50.54) | 26,783 | (70.31) | 2.32 | (2.26–2.38) | |
| Type | <0.0001 | ||||||
| STEMI | 43,486 | (43.53) | 13,830 | (36.31) | 1.00 | — | |
| NSTEMI | 56,409 | (56.47) | 24,263 | (63.69) | 1.35 | (1.32–1.41) | |
| Comorbidities | |||||||
| Hypertension | 54,298 | (54.36) | 20,276 | (53.23) | 0.96 | (0.93–0.98) | <0.0001 |
| Dyslipidemia | 48,079 | (48.13) | 15,193 | (39.88) | 0.72 | (0.70–0.73) | <0.0001 |
| Diabetes mellitus | 32,322 | (32.36) | 16,131 | (42.35) | 1.54 | (1.50–1.57) | <0.0001 |
| Peripheral vascular disease | 2552 | (2.55) | 1581 | (4.15) | 1.65 | (1.55–1.76) | <0.0001 |
| End-stage renal disease | 2317 | (2.32) | 1125 | (2.95) | 1.28 | (1.19–1.38) | <0.0001 |
| Stroke | 3192 | (3.20) | 832 | (2.18) | 0.68 | (0.63–0.73) | <0.0001 |
| COPD | 9101 | (9.11) | 4311 | (11.32) | 1.27 | (1.23–1.32) | <0.0001 |
| Atrial fibrillation | 5230 | (5.24) | 3190 | (8.37) | 1.65 | (1.58–1.73) | <0.0001 |
| VT/VF | 3446 | (3.45) | 2782 | (7.30) | 2.21 | (2.10–2.32) | <0.0001 |
| Reperfusion intervention | |||||||
| PCI | 56,499 | (56.56) | 17,058 | (44.78) | 0.62 | (0.61–0.64) | <0.0001 |
| In-hospital medication | |||||||
| Antiplatelets † | 85,264 | (85.35) | 32,918 | (86.41) | 1.09 | (1.06–1.13) | <0.0001 |
| ACEI or ARB | 61,092 | (61.16) | 23,340 | (61.27) | 1.01 | (0.98–1.03) | 0.6954 |
| Statin | 38,949 | (38.99) | 12,104 | (31.77) | 0.73 | (0.71–0.75) | <0.0001 |
| Beta blocker | 53,653 | (53.71) | 17,743 | (46.58) | 0.75 | (0.73–0.77) | <0.0001 |
| Spironolactone | 5751 | (5.76) | 8469 | (22.23) | 4.68 | (4.52–4.85) | <0.0001 |
| Follow-up period years, mean (SD) | 4.42 | (3.80) | 2.64 | (3.19) | — | — | <0.0001 |
| Variables | Adjusted HR | 95% CI | p Value |
|---|---|---|---|
| In-hospital HF (ref = no HF) | 1.85 | (1.81–1.88) | <0.0001 |
| Male (ref = female) | 1.04 | (1.02–1.06) | <0.0001 |
| age ≥ 65 years (ref = < 65 years) | 2.35 | (2.30–2.42) | <0.0001 |
| STEMI (ref = NSTEMI) | 0.94 | (0.92–0.96) | <0.0001 |
| Comorbidities | |||
| Hypertension | 1.07 | (1.05–1.09) | <0.0001 |
| Dyslipidemia | 0.94 | (0.91–0.97) | <0.0001 |
| Diabetes mellitus | 1.28 | (1.26–1.31) | <0.0001 |
| Peripheral vascular disease | 1.46 | (1.41–1.53) | <0.0001 |
| End-stage renal disease | 1.52 | (1.45–1.60) | <0.0001 |
| Stroke | 1.19 | (1.12–1.26) | <0.0001 |
| COPD | 1.16 | (1.13–1.19) | <0.0001 |
| Atrial fibrillation | 0.97 | (0.94–1.00) | 0.0381 |
| VT/VF | 1.33 | (1.28–1.38) | <0.0001 |
| Primary reperfusion intervention | |||
| PCI/CABG | 0.48 | (0.47–0.49) | <0.0001 |
| In-hospital medication | |||
| Antiplatelets † | 0.71 | (0.69–0.73) | <0.0001 |
| ACEI or ARB | 0.69 | (0.68–0.71) | <0.0001 |
| Statin | 0.75 | (0.73–0.85) | <0.0001 |
| Beta blocker | 0.83 | (0.81–0.85) | <0.0001 |
| Spironolactone | 1.04 | (1.01–1.06) | 0.0114 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, W.-H.; Mar, G.-Y.; Wei, K.-C.; Cheng, C.-C.; Huang, W.-C. Risk Factors and Outcomes of Heart Failure Following First-Episode of Acute Myocardial Infarction—A Case Series Study of 161,384 Cases. Healthcare 2021, 9, 1382. https://doi.org/10.3390/healthcare9101382
Wang W-H, Mar G-Y, Wei K-C, Cheng C-C, Huang W-C. Risk Factors and Outcomes of Heart Failure Following First-Episode of Acute Myocardial Infarction—A Case Series Study of 161,384 Cases. Healthcare. 2021; 9(10):1382. https://doi.org/10.3390/healthcare9101382
Chicago/Turabian StyleWang, Wen-Hwa, Guang-Yuan Mar, Kai-Che Wei, Chin-Chang Cheng, and Wei-Chun Huang. 2021. "Risk Factors and Outcomes of Heart Failure Following First-Episode of Acute Myocardial Infarction—A Case Series Study of 161,384 Cases" Healthcare 9, no. 10: 1382. https://doi.org/10.3390/healthcare9101382