
Development and Validation of the Nursing Students’ Rights Awareness Scale in Clinical Practice: A Scale Development Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Approach
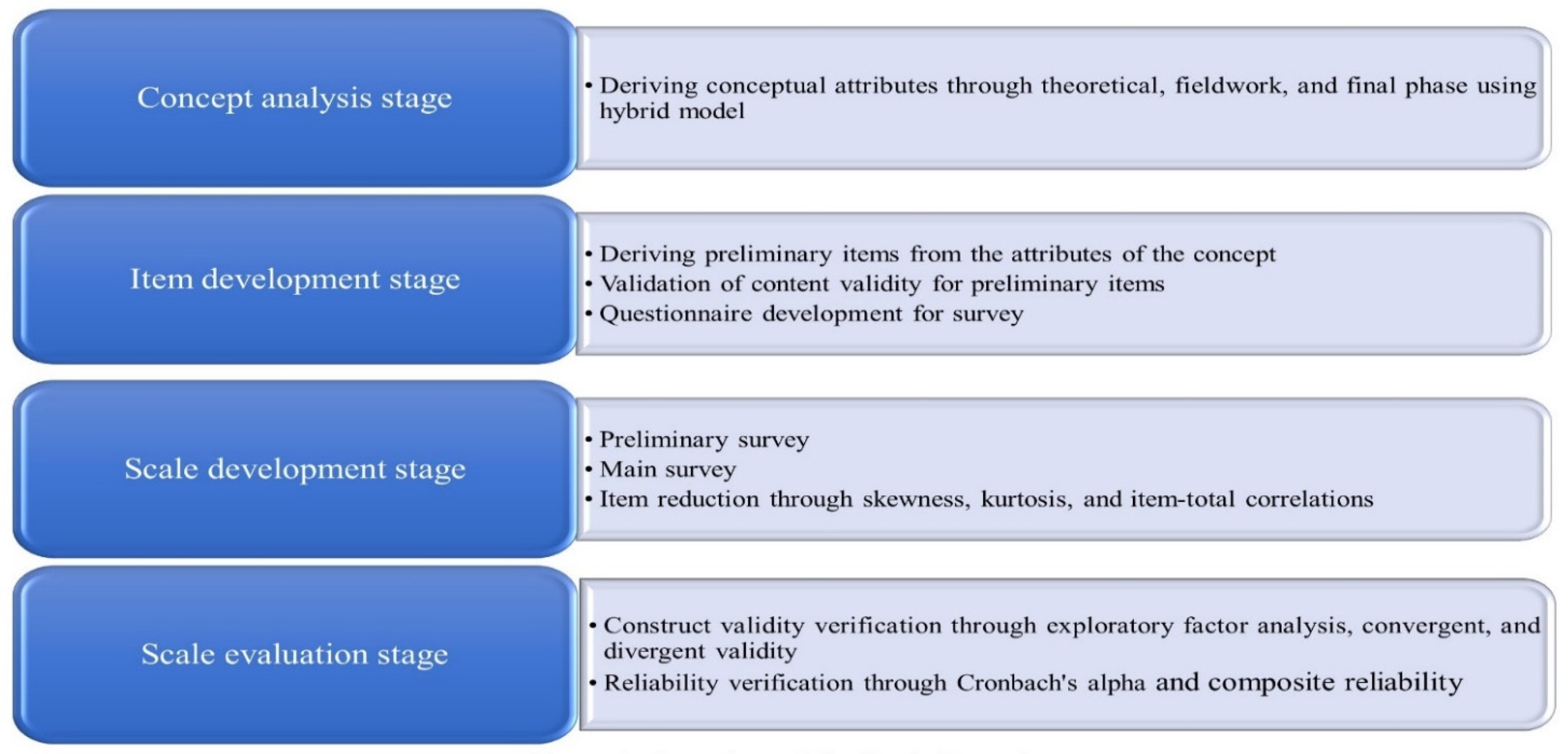
2.2. Study Procedure
2.2.1. Concept Analysis Stage
2.2.2. Item Development Stage
Questionnaire Development
2.2.3. Scale Development Stage
2.2.4. Scale Evaluation Stage
2.3. Study Participants
2.4. Data Collection
2.4.1. In-Depth Interviews
2.4.2. Main Survey
2.5. Data Analysis
2.6. Ethical Considerations
3. Results
3.1. Characteristics of the Participants
3.2. Item Analysis
3.3. Test of Construct Validity
3.4. Test of Reliability
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- National Student Nurses Association the Bill of Rights and Responsibilities for Students of Nursing. 2020. Available online: https://www.dropbox.com/s/a229ong58d5jx4p/Code%20of%20Ethics.pdf?dl=0 (accessed on 7 August 2021).
- Park, S.H.; Cho, H.Y. Experiences of perception of nursing students’ rights in clinical practice. J. Korean Acad. Soc. Nurs. Educ. 2019, 25, 471–483. [Google Scholar] [CrossRef] [Green Version]
- Kalyani, M.N.; Jamshidi, N.; Molazem, Z.; Torabizadeh, C.; Sharif, F. How do nursing students experience the clinical learning environment and respond to their experiences? A qualitative study. BMJ Open 2019, 9, e028052. [Google Scholar] [CrossRef] [Green Version]
- Peters, A.B.; Quinn, B.; Moreno, R. Undergraduate nursing clinical absences: A review. Teach. Learn. Nurs. 2019, 14, 37–42. [Google Scholar] [CrossRef]
- Kapucu, S.; Bulut, H. Turkish Nursing Students’ Views of Their Clinical Learning Environment: A Focus Group Study. Park. J. Med. Sci. 2011, 27, 1149–1153. [Google Scholar]
- Miligi, E.; Selim, A.; Salem, S.S.; Prince, J. Experience of nursing students in clinical practice: A qualitative study. Int. J. Nurs. 2019, 6, 19–24. [Google Scholar] [CrossRef]
- Kang, J.; Jeong, Y.J.; Kong, K.R. Threats to identity: A grounded theory approach on student nurses’ experience of incivility during clinical placement. J. Korean Acad. Nurs. 2018, 48, 85–95. [Google Scholar] [CrossRef] [Green Version]
- Mamaghani, E.A.; Rahmani, A.; Hassankhani, H.; Zamanzadeh, V.; Campbell, S.; Fast, O.; Irajpour, A. Experiences of Iranian nursing students regarding their clinical learning environment. Asian Nurs. Res. 2018, 12, 216–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.W.; Ha, N.S. Nursing students’ clinical experiences. J. Korean Acad. Psychiatr. Ment. Health Nurs. 2003, 12, 27–35. [Google Scholar] [CrossRef]
- Oh, D.N.; Um, Y.; Kim, C.; Ju, S.; Choi, J.H.; Park, M.S. The coping experience of nursing students in clinical practice: Trying to be a meaningful presence. J. Korean Acad. Soc. Nurs. Educ. 2016, 22, 430–440. [Google Scholar] [CrossRef] [Green Version]
- Esmaeili, M.; Cheraghi, M.A.; Salsali, M.; Ghiyasvandian, S. Nursing students’ expectations regarding effective clinical education: A qualitative study. Int. J. Nurs. Pract. 2014, 20, 460–467. [Google Scholar] [CrossRef]
- Schwartz-Barcott, D.; Kim, H.S. An Expansion and Elaboration of the Hybrid Model of Concept Development. In Concept Development in Nursing: Foundations, Techniques, and Applications; Rodgers, B.L., Knafl, K.A., Eds.; WB Saunders: Philadelphia, PA, USA, 2000; pp. 129–159. [Google Scholar]
- Ko, I.; Choi, S.; Kim, J.S. Development and validation of the new version of spirituality assessment scale. J. Korean Acad. Nurs. 2020, 50, 132–146. [Google Scholar] [CrossRef]
- Boateng, G.O.; Neilands, T.B.; Frongillo, E.A.; Melgar-Quiñonez, H.R.; Young, S.L. Best practices for developing and validating scales for health, social, and behavioral research: A primer. Front. Public Health 2018, 6, 149. [Google Scholar] [CrossRef] [PubMed]
- Nunnally, J.C. Psychometric Theory, 2nd ed.; McGraw-Hill Companies: New York, NY, USA, 1978. [Google Scholar]
- Polit, D.F.; Beck, C.T.; Owen, S.V. Is the CVI an acceptable indicator of content validity? Appraisal and recommendations. Res. Nurs. Health 2007, 30, 459–467. [Google Scholar] [CrossRef]
- Hoyle, R.H. Structural Equation Modeling: Concepts, Issues, and Applications; Sage: Thousand Oaks, CA, USA, 1995. [Google Scholar]
- Lim, L.; Lee, P.; Bae, K.; Lee, E.O.; Lee, N.Y.; Park, H.A.; Lee, I.S.; Kim, J.I.; Bae, J.I.; Lee, S.M.; et al. Nursing Research and Statistical Analysis; Soomoonsa: Paju, Korea, 2009; p. 263. [Google Scholar]
- Williams, B.; Onsman, A.; Brown, T. Exploratory factor analysis: A five-step guide for novices. Australas. J. Paramed. 2010, 8. [Google Scholar] [CrossRef] [Green Version]
- Hair, J.F.; Sarstedt, M.; Hopkins, L.; Kuppelwieser, V. Partial least squares structural equation modeling (PLS-SEM): An emerging tool in business research. Eur. Bus. Rev. 2014, 26, 106–121. [Google Scholar] [CrossRef]
- Ab Hamid, M.R.; Sami, W.; Mohmad Sidek, M.H. Discriminant validity assessment: Use of Fornell & Larcker criterion versus HTMT criterion. J. Phys. Conf. Ser. 2017, 890, 1–5. [Google Scholar] [CrossRef]
- Ramirez, R.R.; Palos-Sanchez, P.R. Environmental firms’ better attitude towards nature in the context of corporate compliance. Sustainability 2018, 10, 3321. [Google Scholar] [CrossRef] [Green Version]
- Bawadi, H.A.; Al-Hamdan, Z.M.; Nabolsi, M.; Abu-Moghli, F.; Zumot, A.; Walsh, A. Jordanian nursing student and instructor perceptions of the clinical learning environment. Int. J. Nurs. Educ. Scholarsh. 2019, 16, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J.; Kim, E.J. An exploratory study on the rights of students in their social work field practicum: In the aspect of the rights to learn and the rights to work. Korean J. Soc. Welf. 2017, 69, 147–174. [Google Scholar]
- Rajeswaran, L. Clinical experiences of nursing students at a selected institute of health sciences in Botswana. Health Sci. J. 2016, 10, 471–476. [Google Scholar] [CrossRef]
- Kim, H.J.; Huh, J.S. The right of the clinical training for the medical students and privacy of the patients. Korean J. Med. Law 2013, 21, 107–123. [Google Scholar]
- Jamshidi, N.; Molazem, Z.; Sharif, F.; Torabizadeh, C.; Najafi Kalyani, M. The challenges of nursing students in the clinical learning environment: A qualitative study. Sci. World J. 2016, 2016, 1846178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karatas, H.; Ozturk, C.; Bektas, M. A study of bullying against nursing students. J. Nurs. Res. 2017, 25, 198–202. [Google Scholar] [CrossRef] [PubMed]
- Canadian Nursing Students’ Association Bill of Rights and Responsibilities. Available online: https://cnsa.ca/publication/nursing-students-bill-of-rights-and-responsibilities/ (accessed on 5 January 2021).
- Arkan, B.; Ordin, Y.; Yılmaz, D. Undergraduate nursing students’ experience related to their clinical learning environment and factors affecting to their clinical learning process. Nurse Educ. Pract. 2018, 29, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Arribas-Marín, J.; Hernández-Franco, V.; Plumed-Moreno, C. Nursing students’ perception of academic support in the practicum: Development of a reliable and valid measurement instrument. J. Prof. Nurs. 2017, 33, 387–395. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | n (%) | M ± SD |
|---|---|---|
| Gender | ||
| Female | 210 (94.6) | |
| Male | 12 (5.4) | |
| Age (years) | ||
| 20–29 | 210 (94.6) | 23.76 ±3.52 |
| >30 | 12 (5.4) | |
| Clinical training experience | ||
| 22 weeks | 32 (14.4) | 24.79 ±1.46 |
| 24 weeks | 70 (31.5) | |
| 26 weeks | 120 (54.1) | |
| Satisfaction with nursing | ||
| Satisfied | 135 (60.8) | |
| Moderate | 77 (34.7) | |
| Dissatisfied | 10 (4.5) | |
| Satisfaction with clinical training | ||
| Satisfied | 79 (35.6) | |
| Moderate | 110 (49.5) | |
| Dissatisfied | 33 (14.9) | |
| School location | ||
| Jeonbuk | 34 (15.3) | |
| Seoul | 151 (68.0) | |
| Gyeonggi-do | 37 (16.7) | |
| Previous clinical training | ||
| 1 year | 34 (15.3) | |
| Over 1 year | 188 (84.7) | |
| Participation period of clinical training | ||
| Spring and fall semester | 188 (84.7) | |
| Summer and winter semester | 34 (15.3) | |
| Completion of rights-related training | ||
| Yes | 144 (64.9) | |
| No | 78 (35.1) |
| (Item Number) Item | Factor Loading | ||
|---|---|---|---|
| Factor 1 | Factor 2 | Factor 3 | |
| (11) I have the rights to receive information in advance on the response instructions in case of an incident or an accident. | 0.74 | 0.36 | 0.20 |
| (20) I have the rights to be treated respectfully. | 0.72 | 0.21 | 0.29 |
| (16) Universities must have a system implemented for students to report any disadvantages or injustices experienced immediately. | 0.67 | 0.28 | 0.30 |
| (13) The clinical instructor must pay attention to solving the students’ suggestions or requests. | 0.65 | 0.19 | 0.40 |
| (15) The university must have a system to respond systematically to the clinical training institution by representing the students in case of incidents and accidents that occur during the clinical training period, and to advocate for the students. | 0.65 | 0.34 | 0.21 |
| (10) I have the rights to receive information about infection status of patients in advance. | 0.65 | 0.42 | 0.16 |
| (19) I have the right to be free from verbal, physical, and sexual assault. | 0.65 | 0.24 | 0.25 |
| (18) The clinical instructor must provide attention and support in guiding the students during clinical training. | 0.55 | 0.32 | 0.45 |
| (2) I have the rights to ask questions to the nurse during clinical training and hear the answers. | 0.20 | 0.77 | 0.16 |
| (3) I have the rights to learn according to the standardized clinical training manual. | 0.24 | 0.72 | 0.16 |
| (4) I have the rights to receive a systematic orientation from a unit manager at the beginning of the clinical training. | 0.38 | 0.70 | 0.09 |
| (23) I have the rights to be addressed by a title that shows respect to the students (e.g., a student nurse). | 0.23 | 0.14 | 0.88 |
| (22) I have the rights to not perform tasks that are not directly relevant to the clinical training. | 0.20 | 0.16 | 0.73 |
| (25) I have the rights to have the mealtime guaranteed. | 0.34 | 0.13 | 0.61 |
| Eigen value | 7.31 | 1.52 | 1.06 |
| Explained variance (%) | 29.6 | 17.3 | 16.4 |
| Total explained variance (%) | 29.6 | 46.9 | 63.3 |
| Factors | Factor 1 r2 (p) | Factor 2 r2 (p) | Factor r2 (p) | AVE\ |
|---|---|---|---|---|
| Factor 1 | 1 | 0.77 | ||
| Factor 2 | 0.50 (<0.01) | 1 | 0.86 | |
| Factor 3 | 0.41 (<0.01) | 0.18 (<0.01) | 1 | 0.86 |
| Subfactors | Item Number | Cronbach’s Alpha | Composite Reliability |
|---|---|---|---|
| Factor 1: The rights to be protected, cared, supported, and respected | 11 20 16 13 15 10 19 18 | 0.92 | 0.96 |
| Factor 2: The rights to learn | 2 3 4 | 0.83 | 0.95 |
| Factor 3: The rights to be recognized as a member of a nursing team | 23 22 25 | 0.82 | 0.95 |
| Total | 0.92 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, S.-H.; Choi, M.-Y. Development and Validation of the Nursing Students’ Rights Awareness Scale in Clinical Practice: A Scale Development Study. Healthcare 2021, 9, 1323. https://doi.org/10.3390/healthcare9101323
Park S-H, Choi M-Y. Development and Validation of the Nursing Students’ Rights Awareness Scale in Clinical Practice: A Scale Development Study. Healthcare. 2021; 9(10):1323. https://doi.org/10.3390/healthcare9101323
Chicago/Turabian StylePark, Sung-Hee, and Mi-Young Choi. 2021. "Development and Validation of the Nursing Students’ Rights Awareness Scale in Clinical Practice: A Scale Development Study" Healthcare 9, no. 10: 1323. https://doi.org/10.3390/healthcare9101323