
A Theory-Based Analysis of COVID-19 Vaccine Hesitancy among African Americans in the United States: A Recent Evidence




Abstract
:1. Introduction
1.1. Study Design and Participants
1.2. Recruitement and Data Collection
1.3. Ethical Considerations
1.4. Survey Instrument
1.5. Statistical Analysis
2. Results
3. Discussion
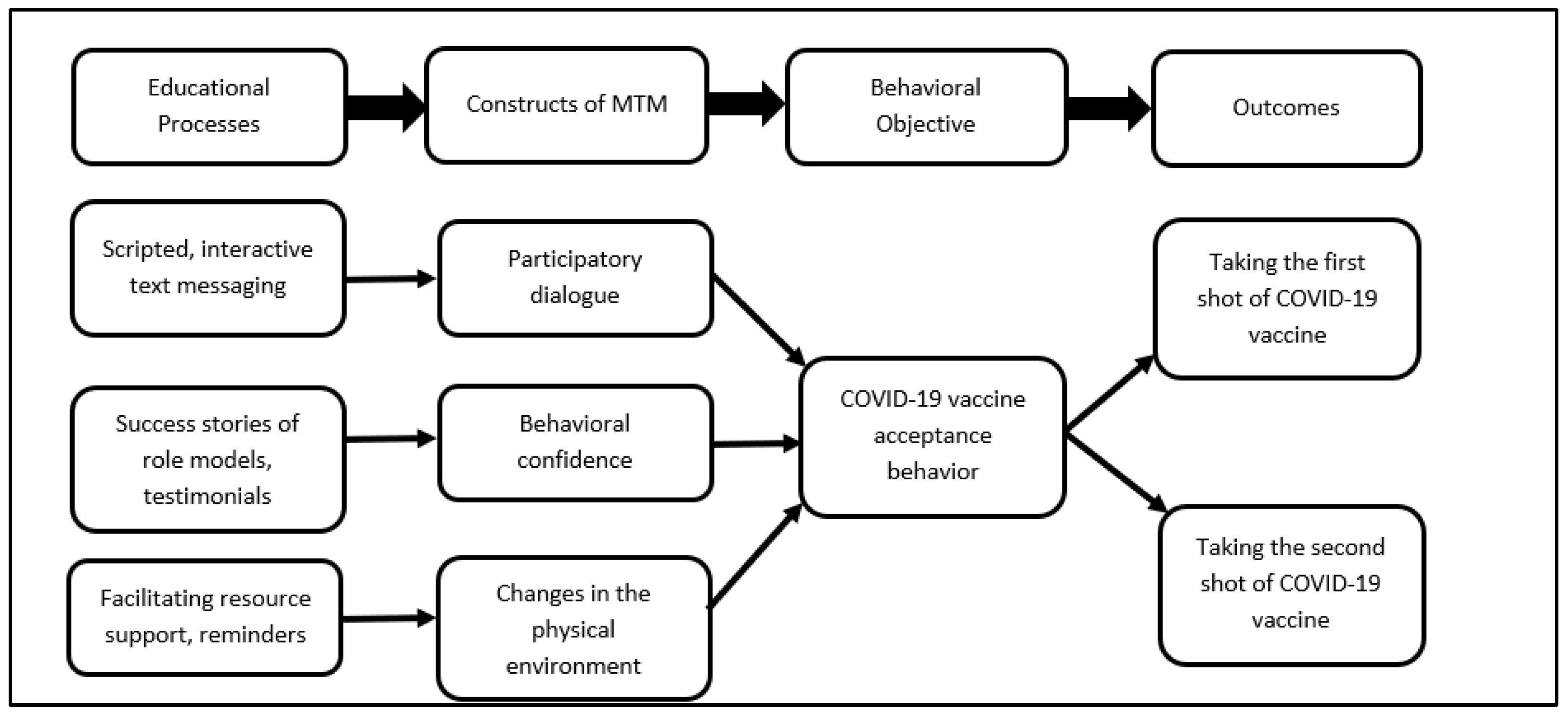
3.1. Proposition of a m-Health (Mobile Phone-Based Intervention)
3.2. Strengths and Limitations
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Variable | New Variable 1 (X1) | New Variable 2 (X2) | New Variable 3 (X3) |
|---|---|---|---|
| Region | |||
| 1 Midwest | 1 | 0 | 0 |
| 2 West | 0 | 1 | 0 |
| 3 Northeast | 0 | 0 | 1 |
| 4 South | 0 | 0 | 0 |
| Religion | |||
| 1 Christianity | 0 | 0 | - |
| 2 Atheist | 0 | 1 | - |
| 3 Others | 1 | 0 | - |
| Political affiliation | |||
| 1 Democrat | 1 | 0 | - |
| 2 Republicans | 0 | 0 | - |
| 3 Others | 0 | 1 | - |
References
- Centers for Disease Control and Prevention. Vaccination Offers Higher Protection Than Previous COVID-19 Infection. 2021. Available online: https://www.cdc.gov/media/releases/2021/s0806-vaccination-protection.html (accessed on 25 August 2021).
- United States Government Accountability Office. Operation Warp Speed. 2021. Available online: https://www.gao.gov/assets/gao-21-319.pdf (accessed on 11 July 2021).
- National Institutes of Health. COVID-19 Vaccines NIH’s Role in Vaccine Development and Vaccine Studies to Prevent COVID-19. 2021. Available online: https://covid19.nih.gov/treatments-and-vaccines/covid-19-vaccines (accessed on 23 August 2021).
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Oliver, S.E.; Gargano, J.W.; Scobie, H.; Wallace, M.; Hadler, S.C.; Leung, J.; Blain, A.E.; McClung, N.; Campos-Outcalt, D.; Morgan, R.L.; et al. The Advisory Committee on Immunization Practices’ Interim Recommendation for Use of Janssen COVID-19 Vaccine—United States, February 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 329–332. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Marc, G.P.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Badur, S.; Ota, M.; Öztürk, S.; Adegbola, R.; Dutta, A. Vaccine confidence: The keys to restoring trust. Hum. Vaccines Immunother. 2020, 16, 1007–1017. [Google Scholar] [CrossRef]
- Ball, P. Anti-vaccine movement could undermine efforts to end coronavirus pandemic, researchers warn. Nature 2020, 581, 251. [Google Scholar] [CrossRef]
- Dror, A.A.; Eisenbach, N.; Taiber, S.; Morozov, N.G.; Mizrachi, M.; Zigron, A.; Srouji, S.; Sela, E. Vaccine hesitancy: The next challenge in the fight against COVID-19. Eur. J. Epidemiol. 2020, 35, 775–779. [Google Scholar] [CrossRef] [PubMed]
- McAteer, J.; Yildirim, I.; Chahroudi, A. The VACCINES Act: Deciphering Vaccine Hesitancy in the Time of COVID-19. Clin. Infect. Dis. 2020, 71, 703–705. [Google Scholar] [CrossRef] [PubMed]
- Our World in Data. Coronavirus (COVID-19) Vaccination. 2021. Available online: https://ourworldindata.org/covid-vaccinations?country=USA (accessed on 25 August 2021).
- White House. Fact Sheet: President Biden to Announce Goal to Administer at Least One Vaccine Shot to 70% of the U.S. Adult Population by 4 July. 2021. Available online: https://www.whitehouse.gov/briefing-room/statements-releases/2021/05/04/fact-sheet-president-biden-to-announce-goal-to-administer-at-least-one-vaccine-shot-to-70-of-the-u-s-adult-population-by-july-4th/ (accessed on 11 August 2021).
- Khubchandani, J.; Sharma, S.; Price, J.H.; Wiblishauser, M.J.; Sharma, M.; Webb, F.J. COVID-19 vaccination hesitancy in the United States: A rapid national assessment. J. Community Health 2021, 46, 270–277. [Google Scholar] [CrossRef] [PubMed]
- Khubchandani, J.; Macias, Y. COVID-19 vaccination hesitancy in Hispanics and African-Americans: A review and recommendations for practice. Brain Behav. Immunity-Health 2021, 15, 100277. [Google Scholar] [CrossRef] [PubMed]
- Corbie-Smith, G.; Thomas, S.B.; George, M.M. Distrust, Race, and Research. JAMA 2002, 162, 2458–2463. [Google Scholar] [CrossRef] [Green Version]
- Dawson, M.A.; Giger, J.N.; Powell-Young, Y.; Brannon, C.B. Why African-Americans are hesitant to take the newly proposed COVID-19 vaccines: Tuskegee revisited. J. Natl. Black Nurses Assoc. 2020, 31, 6–8. [Google Scholar]
- Ferdinand, K.C.; Nedunchezhian, S.; Reddy, T.K. The COVID-19 and influenza “twindemic”: Barriers to influenza vaccination and potential acceptance of SARS-CoV2 vaccination in African Americans. J. Natl. Med. Assoc. 2020, 112, 681–687. [Google Scholar] [CrossRef] [PubMed]
- Webb, F.J.; Khubchandani, J.; Striley, C.W.; Cottler, L.B. Black-White differences in willingness to participate and perceptions about health research: Results from the population-based HealthStreet study. J. Immigr. Minority Health 2019, 21, 299–305. [Google Scholar] [CrossRef]
- Woko, C.; Siegel, L.; Hornik, R. An investigation of low COVID-19 vaccination intentions among Black Americans: The role of behavioral beliefs and trust in COVID-19 information sources. J. Health Commun. 2020, 25, 819–826. [Google Scholar] [CrossRef] [PubMed]
- Millett, G.A.; Jones, A.T.; Benkeser, D.; Baral, S.; Mercer, L.; Beyrer, C.; Honermann, B.; Lankiewicz, E.; Mena, L.; Crowley, J.S.; et al. Assessing differential impacts of COVID-19 on black communities. Ann. Epidemiol. 2020, 47, 37–44. [Google Scholar] [CrossRef]
- Burger, A.E.; Reither, E.N.; Mamelund, S.-E.; Lim, S. Black-white disparities in 2009 H1N1 vaccination among adults in the United States: A cautionary tale for the COVID-19 pandemic. Vaccine 2021, 39, 943–951. [Google Scholar] [CrossRef] [PubMed]
- Glanz, K.; Bishop, D.B. The Role of Behavioral Science Theory in Development and Implementation of Public Health Interventions. Annu. Rev. Public Health 2010, 31, 399–418. [Google Scholar] [CrossRef] [Green Version]
- Sharma, M. Theoretical Foundations of Health Education and Health Promotion, 4th ed.; Jones & Bartlett Learning: Sudbury, ON, Canada, 2021. [Google Scholar]
- Sharma, M. Multi-theory model (MTM) for health behavior change. WebmedCentral Behav. 2015, 6, WMC004982. [Google Scholar]
- United States Census Bureau. Quick Facts. Available online: https://www.census.gov/quickfacts/fact/table/US/PST045219 (accessed on 25 August 2021).
- NRC Health. Updated COVID Vaccinations Study: Have Consumers’ Opinions about the Vaccine Changed with an Upcoming Release? 2020. Available online: https://nrchealth.com/updated-covid-vaccinations-study-have-consumers-opinions-about-the-vaccine-changed-with-an-upcoming-release/ (accessed on 12 August 2021).
- Press Ganey Media. Press Ganey COVID-19 Vaccine Hesitancy Research Finds Black/African American Patients Far Less Willing Than Asian or White Patients to Get the Vaccine. Business Wire. 2021. Available online: https://www.businesswire.com/news/home/20210204005712/en/Press-Ganey-COVID-19-Vaccine-Hesitancy-Research-Finds-BlackAfrican-American-Patients-Far-Less-Willing-Than-Asian-or-White-Patients-to-Get-the-Vaccine/?feedref=JjAwJuNHiystnCoBq_hl-aWOJSq7maz1kUlsOIrkZM4xz5QOdfJiTifxwfmkU5A67fxFuNFTHSunhvli30RlBNXya2izy9YOgHlBiZQk2LPgxNjXHjsNmKaXEz4koEK2KQOELXF1Klv27yoigQe38g= (accessed on 25 August 2021).
- ESOMAR. Data Protection Checklist. Available online: https://www.esomar.org/ (accessed on 10 August 2021).
- Qualtrics Market Research Panel Survey. 2021. Available online: https://www.qualtrics.com/market-research/ (accessed on 22 August 2021).
- Sharma, M.; Davis, R.E.; Wilkerson, A.H. COVID-19 Vaccine Acceptance among College Students: A Theory-Based Analysis. Int. J. Environ. Res. Public Health 2021, 18, 4617. [Google Scholar] [CrossRef]
- Hayes, T.; Sharma, M.; Shahbazi, M.; Sung, J.H.; Bennett, R.; Reese-Smith, J. The evaluation of a fourth-generation multi-theory model (MTM) based intervention to initiate and sustain physical activity. Health Promot. Perspect. 2019, 9, 13–23. [Google Scholar] [CrossRef] [Green Version]
- Williams, J.L.; Sharma, M.; Mendy, V.L.; Leggett, S.; Akil, L.; Perkins, S. Using multi theory model (MTM) of health behavior change to explain intention for initiation and sustenance of the consumption of fruits and vegetables among African American men from barbershops in Mississippi. Health Promot. Perspect. 2020, 10, 200–206. [Google Scholar] [CrossRef]
- Sharma, M.; Batra, K.; Davis, R.E.; Wilkerson, A.H. Explaining Handwashing Behavior in a Sample of College Students during COVID-19 Pandemic Using the Multi-Theory Model (MTM) of Health Behavior Change: A Single Institutional Cross-Sectional Survey. Healthcare 2021, 9, 55. [Google Scholar] [CrossRef] [PubMed]
- Sharma, M.; Batra, K.; Flatt, J. Testing the Multi-Theory Model (MTM) to Predict the Use of New Technology for Social Connectedness in the COVID-19 Pandemic. Healthcare 2021, 9, 838. [Google Scholar] [CrossRef]
- Thompson, B. The Use of Statistical Significance Tests in Research. J. Exp. Educ. 2014, 61, 361–377. [Google Scholar] [CrossRef]
- Office of the Assistant Secretary for Planning and Evaluation. 2021. Available online: https://aspe.hhs.gov/reports/vaccine-hesitancy-covid-19-state-county-local-estimates (accessed on 25 August 2021).
- Mansournia, M.A.; Collins, G.S.; Nielsen, R.O.; Nazemipour, M.; Jewell, N.P.; Altman, D.G.; Campbell, M.J. A Checklist for statistical Assessment of Medical Papers (the CHAMP statement): Explanation and elaboration. Br. J. Sports Med. 2021, 55, 1009–1017. [Google Scholar] [CrossRef] [PubMed]
- Laurencin, C.T. Addressing Justified Vaccine Hesitancy in the Black Community. J. Racial Ethn. Health Disparities 2021, 8, 543–546. [Google Scholar] [CrossRef]
- Fisher, K.A.; Bloomstone, S.J.; Walder, J.; Crawford, S.; Fouayzi, H.; Mazor, K.M. Attitudes toward a potential SARS-CoV-2 vaccine: A survey of U.S. Adults. Ann. Intern. Med. 2020, 173, 964–973. [Google Scholar] [CrossRef]
- Mercadante, A.R.; Law, A.V. Will they, or won’t they? Examining patients’ vaccine intention for flu and COVID-19 using the health belief model. Res. Soc. Adm. Pharm. 2021, 17, 1596–1605. [Google Scholar] [CrossRef]
- Ruiz, J.B.; Bell, R.A. Predictors of intention to vaccinate against COVID-19: Results of a nationwide survey. Vaccine 2021, 39, 1080–1086. [Google Scholar] [CrossRef]
- Troiano, G.; Nardi, A. Vaccine hesitancy in the era of COVID-19. Public Health 2021, 194, 245–251. [Google Scholar] [CrossRef]
- Bogart, L.M.; Ojikutu, B.O.; Tyagi, K.; Klein, D.J.; Mutchler, M.G.; Dong, L.; Lawrence, S.J.; Thomas, D.R.; Kellman, S. COVID-19 related medical mistrust, health impacts, and potential vaccine hesitancy among Black Americans living with HIV. J. Acquir. Immune Defic. Syndr. 2021, 86, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Mayo Clinic. U.S. COVID-19 Vaccine Tracker: See Your State’s Progress. Available online: https://www.mayoclinic.org/coronavirus-covid-19/vaccine-tracker (accessed on 22 August 2021).
- Pew Research Center. Facts about the U.S. Black Population. Available online: https://www.pewresearch.org/social-trends/fact-sheet/facts-about-the-us-black-population/ (accessed on 22 August 2021).
- Agarwal, R.; Dugas, M.; Ramaprasad, J.; Luo, J.; Li, G.; Gao, G.G. Socioeconomic privilege and political ideology are associated with racial disparity in COVID-19 vaccination. Proc. Natl. Acad. Sci. USA 2021, 118, e2107873118. [Google Scholar] [CrossRef] [PubMed]
- Allen, J.D.; Feng, W.; Corlin, L.; Porteny, T.; Acevedo, A.; Schildkraut, D.; King, E.; Ladin, K.; Fu, Q.; Stopka, T.J. Why are some people reluctant to be vaccinated for COVID-19? A cross-sectional survey among U.S. Adults in May–June 2020. Prev. Med. Rep. 2021, 24, 101494. [Google Scholar] [CrossRef] [PubMed]
- Fridman, A.; Gershon, R.; Gneezy, A. COVID-19 and vaccine hesitancy: A longitudinal study. PLoS ONE 2021, 16, e0250123. [Google Scholar] [CrossRef]
- Viswanath, K.; Bekalu, M.; Dhawan, D.; Pinnamaneni, R.; Lang, J.; McLoud, R. Individual and social determinants of COVID-19 vaccine uptake. BMC Public Health 2021, 21, 818. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, B.; Diament, J. Black Muslims Account for a Fifth of All U.S. Muslims, and about Half Are Converts to Islam. Available online: https://www.pewresearch.org/fact-tank/2019/01/17/black-muslims-account-for-a-fifth-of-all-u-s-muslims-and-about-half-are-converts-to-islam/ (accessed on 22 August 2021).



| Domain | Constructs | Description (s) | |
|---|---|---|---|
| Intention of initiating COVID-19 vaccination | Participatory dialogue (Difference of advantages and disadvantages) | Advantages | Perceived advantages of COVID-19 vaccination |
| Disadvantages | Perceived disadvantages of COVID-19 vaccination | ||
| Behavioral confidence | Confidence of taking COVID-19 vaccination despite external and internal restrictive factors | ||
| Changes in the physical environment | COVID-19 vaccination by facilitating enabling factors from the environment | ||
| Variable Name | Categories | Overall Sample | COVID-19 Vaccine Hesitancy | Test Statistics | p Value | Effect Size | |
|---|---|---|---|---|---|---|---|
| Yes (n = 208) | No (n = 220) | ||||||
| Age (Mean ± SD) | - | 43.43 ± 16.9 | 40.5 ± 15.8 | 46.2 ± 17.4 | −3.475 * | 0.001 | 0.34 |
| Gender | Male | 203 (47.4) | 101 (48.6) | 102 (46.4) | 1.202 | 0.5 | 0.053 |
| Female | 225 (52.6) | 107 (51.4) | 118 (53.6) | ||||
| Marital status | Divorced/Separated/Widowed | 70 (16.4) | 30 (14.4) | 40 (18.2) | 6.822 | 0.07 | 0.126 |
| Married | 195 (45.6) | 106 (24.8) | 89 (20.8) | ||||
| Never married | 120 (28.0) | 41 (23.6) | 79 (32.3) | ||||
| Other | 43 (10.0) | 23 (11.1) | 20 (9.1) | ||||
| Education | High school diploma or GED | 68 (15.9) | 30 (14.4) | 38 (17.3) | 5.048 | 0.7 | 0.109 |
| Associate degree | 46 (10.7) | 20 (9.6) | 26 (11.8) | ||||
| Bachelor degree | 96 (22.4) | 45 (21.6) | 51 (23.2) | ||||
| Master degree | 68 (15.9) | 37 (17.8) | 31 (14.1) | ||||
| Doctoral degree | 18 (4.2) | 9 (4.3) | 9 (4.1) | ||||
| Professional degree | 14 (3.3) | 5 (2.4) | 9 (4.1) | ||||
| Some college but no degree | 88 (20.6) | 47 (22.6) | 41 (18.6) | ||||
| Trade school | 15 (3.5) | 6 (2.9) | 9 (4.1) | ||||
| Less than a high school diploma | 15 (3.5) | 9 (4.3) | 6 (2.7) | ||||
| Annual Income | Less than $25,000 | 87 (20.3) | 38 (18.3) | 49 (22.3) | 3.910 | 0.7 | 0.096 |
| $25,001–$50,000 | 89 (20.8) | 42 (20.2) | 47 (21.4) | ||||
| $50,001–$75,000 | 76 (17.8) | 38 (18.3) | 38 (17.3) | ||||
| $75,001–$100,000 | 45 (10.5) | 25 (12.0) | 20 (9.1) | ||||
| $100,001–$125,000 | 42 (9.8) | 22 (10.6) | 20 (9.1) | ||||
| $125,001–$150,000 | 39 (9.1) | 22 (10.6) | 17 (7.7) | ||||
| $150,000+ | 50 (11.7) | 21 (10.1) | 29 (13.2) | ||||
| Employed | Yes | 273 (63.8) | 139 (66.8) | 134 (60.9) | 1.621 | 0.2 | 0.062 |
| No | 155 (36.2) | 69 (16.1) | 86 (20.1) | ||||
| Region | Midwest | 94 (22.0) | 44 (21.2) | 50 (22.7) | 16.322 | 0.7 | 0.195 |
| Northeast | 79 (18.5) | 54 (26.0) | 25 (11.4) | <0.001 | |||
| South | 164 (38.3) | 72 (34.6) | 92 (41.8) | 0.1 | |||
| West | 90 (21.0) | 38 (18.3) | 52 (23.6) | 0.2 | |||
| Political affiliation | Democrat | 276 (64.5) | 116 (55.8) | 160 (72.7) | 15.923 | <0.001 | 0.193 |
| Republican | 68 (15.9) | 46 (22.1) | 22 (10.0) | <0.001 | |||
| Others, including independent | 84 (19.6) | 46 (22.1) | 38 (17.3) | 0.2 | |||
| Religion | Christianity | 309 (72.2) | 147 (70.7) | 162 (73.6) | 5.734 | 0.5 | 0.116 |
| Atheist | 45 (10.5) | 17 (8.2) | 28 (12.7) | 0.13 | |||
| Others | 74 (17.3) | 44 (21.2) | 30 (13.6) | 0.04 | |||
| Location of residence | Urban | 240 (56.1) | 114 (54.8) | 126 (57.3) | 2.60 | 0.3 | 0.078 |
| Semi urban | 122 (28.5) | 56 (26.9) | 66 (30.0) | ||||
| Rural | 66 (15.4) | 38 (18.3) | 28 (12.7) | ||||
| MTM Construct | Vaccine Hesitancy | p Value | Effect Size (Cohen d) | |
|---|---|---|---|---|
| Yes (n = 208) | No (n = 220) | |||
| Overall Initiation Score | 1.68 ± 1.47 | 3.06 ± 1.30 | <0.001 | 0.9 [Large] |
| Subscales | ||||
| Perceived Advantages | 7.07 ± 3.60 | 9.01 ± 3.10 | <0.001 | 0.6 [Medium] |
| Perceived Disadvantages | 8.36 ± 3.02 | 5.15 ± 3.12 | <0.001 | 1.0 [Large] |
| Participatory Dialogue | 1.66 ± 1.08 | 4.12 ± 1.01 | <0.001 | 0.2 [Small] |
| Behavior Confidence | 5.67 ± 4.09 | 8.84 ± 3.76 | <0.001 | 0.8 [Large] |
| Changes in the Physical Environment | 7.36 ± 3.65 | 9.21 ± 3.50 | <0.001 | 0.5 [Medium] |
| Variables | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|
| 1. Advantages | - | 0.27 ** | 0.64 ** | 0.57 ** | 0.15 ** |
| 2. Disadvantages | 0.27 ** | - | 00.31 ** | −0.18 ** | 0.15 ** |
| 3. Behavioral Confidence | 0.64 ** | 0.31 ** | - | 0.76 ** | 0.21 ** |
| 4. Physical Environment | 0.57 ** | 0.18 ** | 0.76 ** | - | 0.24 ** |
| 5. Age | 0.15 ** | 0.15 ** | 0.21 ** | 0.24 ** | - |
| Mean | 8.07 | 6.71 | 7.3 | 8.3 | 43.43 |
| Standard Deviation | 3.5 | 3.4 | 4.2 | 3.7 | 16.9 |
| α | 0.91 | 0.77 | 0.91 | 0.93 | - |
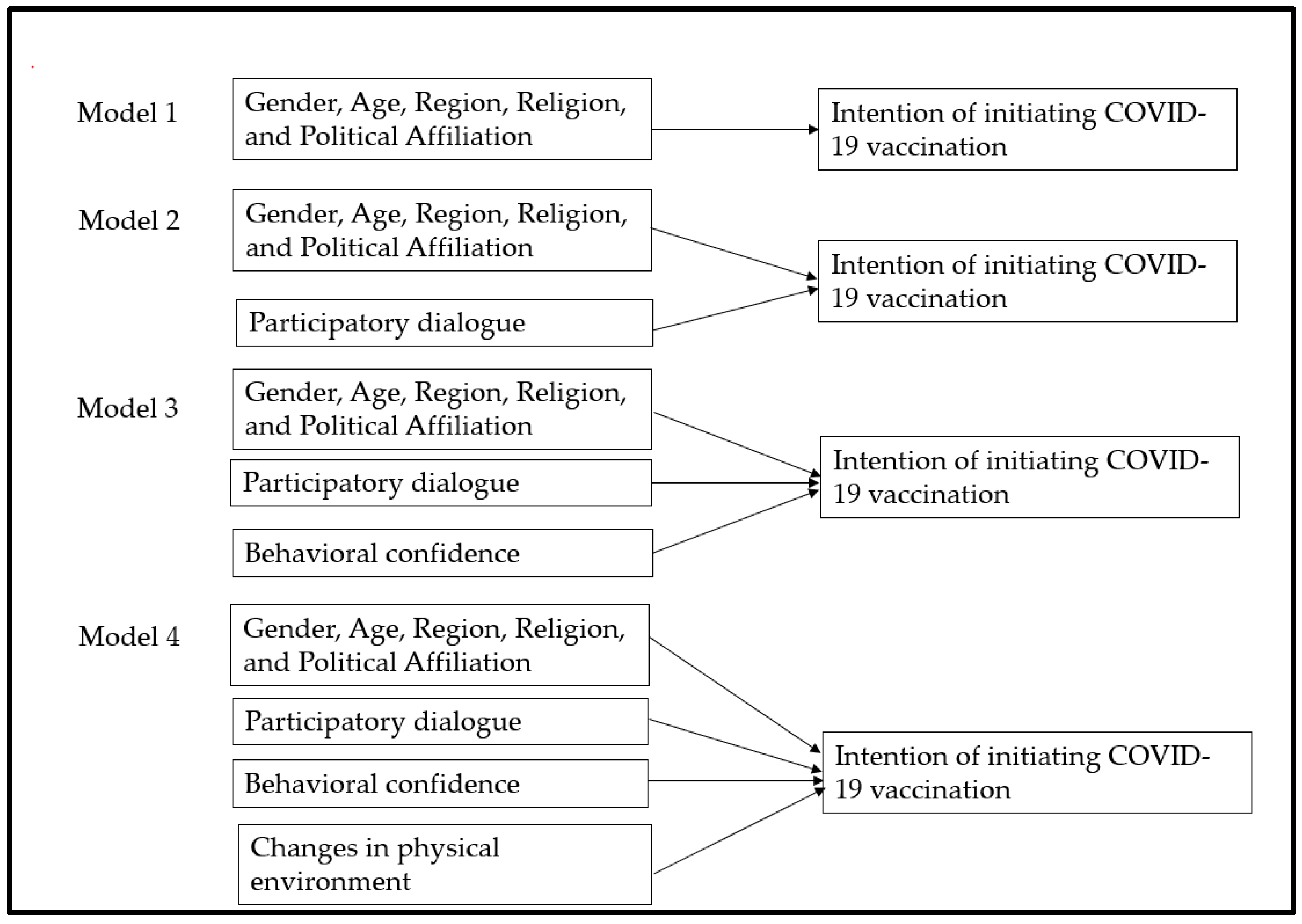
| Variables | Model 1 | Model 2 | Model 3 | Model 4 | ||||
|---|---|---|---|---|---|---|---|---|
| B | β | B | β | B | β | B | β | |
| Vaccine-hesitant group (n = 228) | ||||||||
| Constant | 1.748 | 2.452 | 1.538 | 1.355 | ||||
| Age | −0.020 * | −0.214 | −0.019 ** | −0.199 | −0.018 ** | −0.195 | −0.018 ** | −0.193 |
| Gender (ref: Female) | ||||||||
| Male | 0.332 | 0.112 | −0.057 | −0.019 | −0.017 | −0.006 | −0.029 | −0.010 |
| Political Affiliation (ref: Republicans) | ||||||||
| Democrats | 0.739 | 0.249 | 0.317 | 0.107 | 0.074 | 0.025 | 0.069 | 0.023 |
| Other, including independent | −0.128 | −0.036 | −0.331 | −0.093 | −0.194 | −0.055 | −0.222 | −0.062 |
| Religion Affiliation (ref: Christianity) | ||||||||
| Atheist | −0.288 | −0.054 | −0.157 | −0.029 | 0.262 | 0.049 | .238 | 0.044 |
| Others | 0.399 | 0.110 | 0.343 | 0.095 | 0.159 | 0.044 | 0.164 | 0.045 |
| Region (ref: South) | ||||||||
| Midwest | 0.349 | 0.097 | 0.235 | 0.065 | −0.036 | −0.010 | 0.002 | 0.010 |
| West | 0.165 | 0.043 | 0.073 | 0.019 | −0.284 | −0.074 | −0.245 | −0.064 |
| Northeast | 0.155 | 0.046 | 0.036 | 0.011 | −0.196 | −0.058 | −0.144 | −0.043 |
| MTM Constructs | ||||||||
| Participatory dialogue | - | - | 0.169 ** | 0.587 | 0.106 ** | 0.367 | 0.106 ** | 0.370 |
| Behavioral confidence | - | - | - | - | 0.192 ** | 0.531 | 0.166 ** | 0.460 |
| Changes in the physical environment | - | - | - | - | - | - | 0.042 | 0.104 |
| R2 | 0.159 | - | 0.470 | - | 0.663 | - | 0.670 | - |
| F | 4.156 ** | - | 17.464 ** | - | 35.133 ** | - | 32.944 ** | - |
| Δ R2 | 0.159 | - | 0.311 | - | 0.194 | - | 0.006 | - |
| Δ F | 4.156 ** | - | 115.586 ** | - | 112.750 ** | - | 3.648 ** | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sharma, M.; Batra, K.; Batra, R. A Theory-Based Analysis of COVID-19 Vaccine Hesitancy among African Americans in the United States: A Recent Evidence. Healthcare 2021, 9, 1273. https://doi.org/10.3390/healthcare9101273
Sharma M, Batra K, Batra R. A Theory-Based Analysis of COVID-19 Vaccine Hesitancy among African Americans in the United States: A Recent Evidence. Healthcare. 2021; 9(10):1273. https://doi.org/10.3390/healthcare9101273
Chicago/Turabian StyleSharma, Manoj, Kavita Batra, and Ravi Batra. 2021. "A Theory-Based Analysis of COVID-19 Vaccine Hesitancy among African Americans in the United States: A Recent Evidence" Healthcare 9, no. 10: 1273. https://doi.org/10.3390/healthcare9101273