Assessment of Cardiovascular Risk Factors in Young Adults through the Nursing Diagnosis: A Cross-Sectional Study among International University Students

 , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
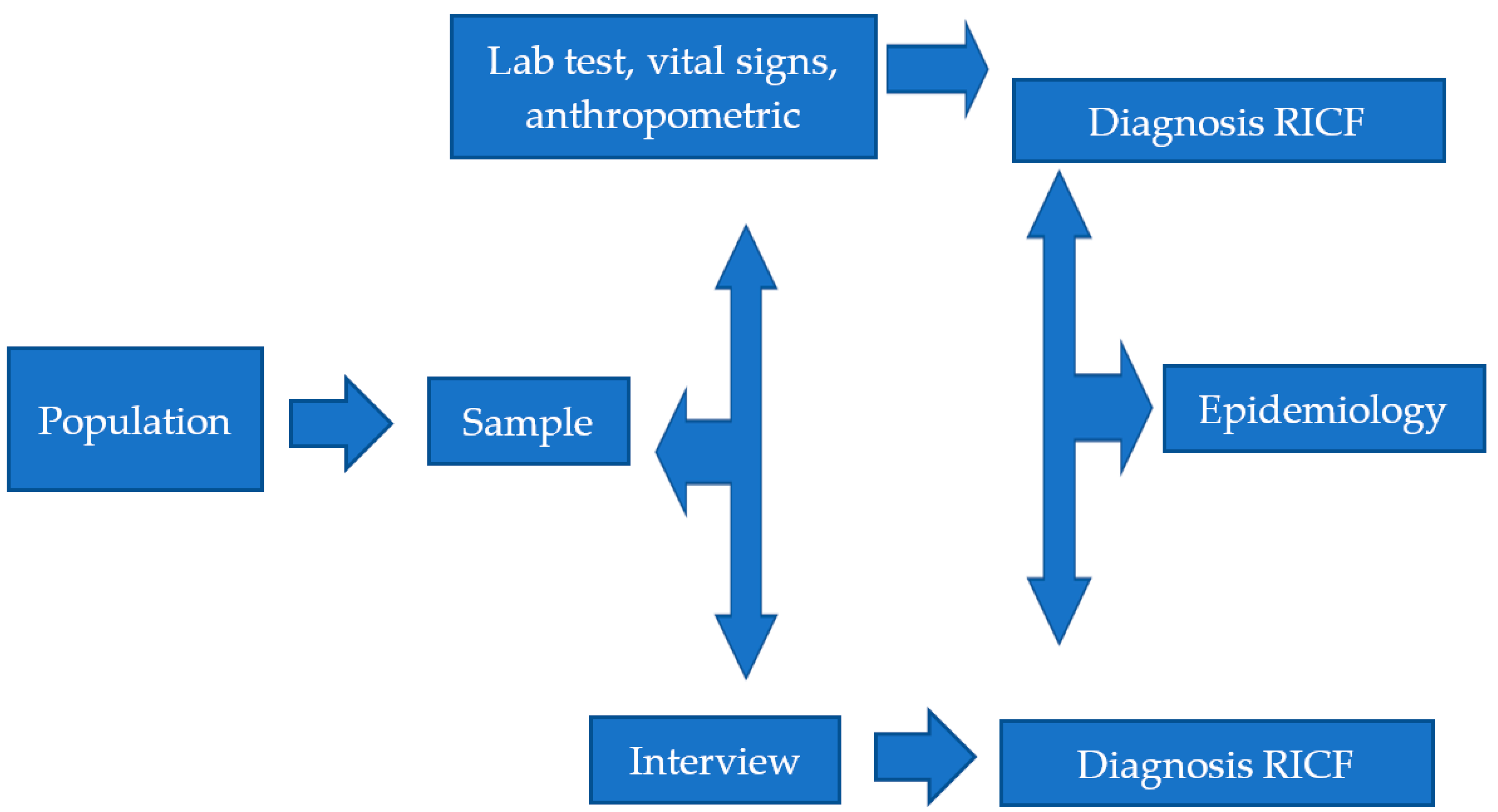
2.1. Design
2.2. Setting
2.3. Sample
2.4. Methodology
2.5. Data Analysis
2.5.1. Clinical Diagnosis Validity: Fehring Clinical Diagnostic Validity Model
2.5.2. Clinical Diagnosis Validity: Concordance between Observers, Kappa Index
2.5.3. Clinical Diagnosis Validity: Sensitivity and Specificity Analysis
2.5.4. Risk of Impaired Cardiovascular Function Risk Factors
2.6. Ethical Aspects
3. Results
3.1. Clinical Diagnosis Validity
3.2. Risk of Impaired-Cardiovascular Function Diagnostic Risk Factors
4. Discussion
4.1. Limitations
4.2. Future Perspective
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Health Topics: Cardiovascular Disease. Fact Sheet. Available online: http://www.who.int/cardiovascular_diseases/en/ (accessed on 11 December 2020).
- World Health Organization. The Health and Environment Linkages Initiative (HELI): Environment and Health in Developing Countries. Available online: https://www.who.int/heli/risks/ehindevcoun/en/ (accessed on 11 December 2020).
- Andersson, C.; Vasan, R.S. Epidemiology of cardiovascular disease in young individuals. Nat. Rev. Cardiol. 2018, 15, 230–240. [Google Scholar] [CrossRef]
- De Backer, G.G. Epidemiology and prevention of cardiovascular disease: Quo vadis? Eur. J. Prev. Cardiol. 2017, 24, 768–772. [Google Scholar] [CrossRef] [PubMed]
- Herdman, T.H.; Kamitsuru, S. Nursing Diagnoses: Definitions and Classification 2018–2020; Thieme: New York, NY, USA, 2018. [Google Scholar]
- Sánchez Gómez, M.B.; Duarte Clíments, G.D. Riesgo de Deterioro de la función Cardiovascular, nuevo diagnóstico NANDA. ENE revista de enfermería. 2013. Available online: http://www.index-f.com/ene/7/7302r.php (accessed on 24 September 2020).
- Genovesi, S.; Giussani, M.; Orlando, A.; Battaglino, M.G.; Nava, E.; Parati, G. Prevention of Cardiovascular Diseases in Children and Adolescents. High Blood Press. Cardiovasc. Prev. 2019, 26, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Redón, J. Global Cardiovascular Risk Assessment: Strengths and Limitations. High Blood Press. Cardiovasc. Prev. 2016, 23, 87–90. [Google Scholar] [CrossRef] [PubMed]
- Saeed, A.; Ballantyne, C.M. Assessing Cardiovascular Risk and Testing in Type 2 Diabetes. Curr. Cardiol. Rep. 2017, 19. [Google Scholar] [CrossRef] [PubMed]
- Silva, E.S.; Castro, D.S.; García, T.R.; Romero, W.G.; Primo, C.C. Care technology to people with colostomy: Diagnosis and nursing interventions. REME: Rev. Min. de Enferm. 2016, 20. [Google Scholar] [CrossRef] [Green Version]
- Sacramento-Pacheco, J.; Duarte-Clíments, G.; Gómez-Salgado, J.; Romero-Martín, M.; Sánchez-Gómez, M.B. Cardiovascular risk assessment tools: A scoping review. Aust. Crit. Care 2019, 32, 540–559. [Google Scholar] [CrossRef]
- Fehring, R.J. Methods to validate nursing diagnoses. Hear. Lung 1987, 16, 625–629. [Google Scholar]
- Echevarría-Pérez, P.; Romero-Sánchez, J.M.; Giró-Formatger, M.D.; Giménez-Fernández, M. Investigación en Metodología y Lenguajes Enfermeros; Elsevier: Madrid, Spain, 2016. [Google Scholar]
- Grove, S.; Gray, J.; Burns, N. Understanding Nursing Research E-Book: Building an Evidence-Based Practice, 6th ed.; Elsevier: St. Louis, MO, USA, 2014. [Google Scholar]
- Grove, S.; Cipher, D. Statistics for Nursing Research, 3rd ed.; Elsevier: St. Louis, MO, USA, 2019. [Google Scholar]
- Altman, D.G. Practical Statistics for Medical Research; Chapman and Hall: London, UK, 1991; pp. 403–405. [Google Scholar]
- Vischer, A.S.; Burkard, T. Principles of Blood Pressure Measurement—Current Techniques, Office vs Ambulatory Blood Pressure Measurement. Cannabinoids Neuropsychiatr. Disord. 2016, 956, 85–96. [Google Scholar] [CrossRef]
- Einarson, T.; Machado, M.; Hemels, M.E.H. Blood glucose and subsequent cardiovascular disease: Update of a meta-analysis. Curr. Med. Res. Opin. 2011, 27, 2155–2163. [Google Scholar] [CrossRef]
- Narwal, V.; Deswal, R.; Batra, B.; Kalra, V.; Hooda, R.; Sharma, M.; Rana, J. Cholesterol biosensors: A review. Steroids 2019, 143, 6–17. [Google Scholar] [CrossRef] [PubMed]
- de Sá Tinôco, J.D.; de Paiva, M.D.G.M.N.; de Queiroz Frazão, C.M.F.; Lucio, K.D.B.; Fernandes, M.I.D.C.D.; de Oliveira Lopes, M.V.; de Carvalho Lira, A.L.B. Clinical validation of the nursing diagnosis of ineffective protection in hemodialysis patients. J. Clin. Nurs. 2017, 27, e195–e202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nunes, M.M.; Lopes, M.V.D.O.; Da Silva, V.M.; Leandro, T.A.; Fróes, N.B.M.; Almeida, A.D.A.P.; Sobreira, B.A.; Nunes, V.M.; De Menezes, A.P.; Ferreira, G.D.L. Validation of Clinical Indicators of the Nursing Diagnosis of Ineffective Protection in Adolescents with Cancer. J. Pediatr. Nurs. 2018, 42, e58–e65. [Google Scholar] [CrossRef] [PubMed]
- Lucio, K.D.B.; Andriola, I.C.; Tinôco, J.D.D.S.; Fernandes, M.I.D.C.D.; De Macedo, B.M.; Cossi, M.S.; Lopes, M.V.D.O.; Lira, A.L.B.D.C. Delay in Growth in Adolescents: Clinical Validation of a Proposed Nursing Diagnosis. J. Pediatr. Nurs. 2019, 46, e72–e76. [Google Scholar] [CrossRef]
- Monteiro, F.P.M.; De Araujo, T.L.; Costa, F.B.C.; Leandro, T.A.; Cavalcante, T.F.; Lopes, M.V.D.O. Clinical validation of nursing diagnosis “Willingness for improved infant development”. Rev. Bras. Enferm. 2016, 69, 855–863. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, R.C.; Duran, E.C.M. Clinical validation of nursing diagnosis “00085 Impaired Physical Mobility” in multiple traumas victims. Rev. Lat.-Am. Enferm. 2019, 27, e3190. [Google Scholar] [CrossRef]
- Lopes, M.V.O.; Silva, V.M.; Herdman, H. Causation and Validation of Nursing Diagnoses: A Middle Range Theory. Int. J. Nurs. Knowl. 2015, 28, 53–59. [Google Scholar] [CrossRef]
- Gonçalves, J.L.; Giovanini, L.P.; Lopes, J.L.; Cornélio, M.E.; Lopes, M.V.O.; Oliveira-Kumakura, A.R.S. Clinical Validation of the Nursing Diagnosis, Decreased Cardiac Tissue Perfusion, in Patients with Coronary Artery Obstruction. Int. J. Nurs. Knowl. 2020, 31, 205–209. [Google Scholar] [CrossRef]
- Peltzer, K.; Pengpid, S.; Sychareun, V.; Ferrer, A.J.G.; Low, W.Y.; Nguyen, T.H.; Win, H.H.; Rochmawati, E.; Turnbull, N. Prehypertension and psychosocial risk factors among university students in ASEAN countries. BMC Cardiovasc. Disord. 2017, 17, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Cruz-Sánchez, E.; Orosio-Méndez, M.; Cruz-Ramírez, T.; Bernardino-García, A.; Vásquez-Domínguez, L.; Galindo-Palma, N.; Grajales-Alonso, I. Factores de riesgo cardiovascular en estudiantes de enfermería de una universidad pública. Enfermería Universitaria 2016, 13, 226–232. [Google Scholar] [CrossRef] [Green Version]
- Kalka, D.; Domagała, Z.A.; Rusiecki, L.; Gworys, B.; Kolęda, P.; Dąbrowski, P.; Szawrowicz-Pełka, T.; Bielous, A.; Micał-Strąk, M.; Pilecki, W. Cardiovascular Risk Factors Among Lower Silesian Students of the Faculty of Medicine: Knowledge and Distribution. Adv. Clin. Exp. Med. 2016, 25, 341–347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbosa, J.B.; Dos Santos, A.M.; Barbosa, M.M.; Barbosa, M.M.; Carvalho, C.A.; Fonseca, P.C.D.A.; Fonseca, J.M.; Barbosa, M.D.C.L.; Bogea, E.G.; Silva, A. Metabolic syndrome, insulin resistance and other cardiovascular risk factors in university students. Ciência Saúde Coletiva 2016, 21, 1123–1136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Sousa, L.S.N.; Macêdo, L.G.D.N.; Moura, J.R.A.; Guimarães, M.R.; Campelo, R.C.V.; Da Silva, A.R.V. Change in blood pressure levels in college students. Texto Context. Enferm. 2015, 24, 1087–1093. [Google Scholar] [CrossRef] [Green Version]
- Kane, A.E.; Howlett, S.E. Differences in Cardiovascular Aging in Men and Women. Adv. Exp. Med. Biol. 2018, 1065, 389–411. [Google Scholar] [CrossRef] [PubMed]
- Vilchez-Barboza, V.; Paravic-Klijn, T.; Salazar-Molina, A.; Saez-Carrillo, K.L. Effectiveness of personalized face-to-face and telephone nursing counseling interventions for cardiovascular risk factors: A controlled clinical trial. Rev. Lat.-Am. Enferm. 2016, 24, e2747. [Google Scholar] [CrossRef] [Green Version]
- Ramos-Lima, M.J.M.; Magalhães-Moreira, T.M.; Florêncio, R.; Braga, P. Factors associated with young adults’ knowledge regarding family history of Stroke. Rev. Latino-Am. Enferm. 2016, 24, e2814. [Google Scholar] [CrossRef] [Green Version]
- Arts, J.; Fernandez, M.L.; Lofgren, I.E. Coronary Heart Disease Risk Factors in College Students. Adv. Nutr. 2014, 5, 177–187. [Google Scholar] [CrossRef] [Green Version]
- Vornanen, M.; Konttinen, H.; Kääriäinen, H.; Männistö, S.; Salomaa, V.; Perola, M.; Haukkala, A. Family history and perceived risk of diabetes, cardiovascular disease, cancer, and depression. Prev. Med. 2016, 90, 177–183. [Google Scholar] [CrossRef] [Green Version]
- Imes, C.C.; Lewis, F.M. Family History of Cardiovascular Disease, Perceived Cardiovascular Disease Risk, and Health-Related Behavior. J. Cardiovasc. Nurs. 2014, 29, 108–129. [Google Scholar] [CrossRef] [Green Version]
- Valerio, L.; Peters, R.J.; Zwinderman, A.H.; Pinto-Sietsma, S.-J. Association of Family History with Cardiovascular Disease in Hypertensive Individuals in a Multiethnic Population. J. Am. Hear. Assoc. 2016, 5, 004260. [Google Scholar] [CrossRef]
- Moonesinghe, R.; Yang, Q.; Zhang, Z.; Khoury, M.J. Prevalence and Cardiovascular Health Impact of Family History of Premature Heart Disease in the United States: Analysis of the National Health and Nutrition Examination Survey, 2007–2014. J. Am. Hear. Assoc. 2019, 8, e012364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akhuemonkhan, E.; Lazo, M. Association between family history of diabetes and cardiovascular disease and lifestyle risk factors in the United States population: The 2009–2012 National Health and Nutrition Examination Survey. Prev. Med. 2017, 96, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Silva, D.; Werneck, A.D.O.; Collings, P.J.; Fernandes, R.A.; Barbosa, D.S.; Ronque, E.R.V.; Sardinha, L.B.; Cyrino, E.S. Family history of cardiovascular disease and parental lifestyle behaviors are associated with offspring cardiovascular disease risk markers in childhood. Am. J. Hum. Biol. 2017, 29, e22995. [Google Scholar] [CrossRef] [PubMed]
- Kashani, M.; Eliasson, A.; Vernalis, M.; Costa, L.; Terhaar, M. Improving Assessment of Cardiovascular Disease Risk by Using Family History. J. Cardiovasc. Nurs. 2013, 28, E18–E27. [Google Scholar] [CrossRef] [PubMed]
- Henriksson, P.; Henriksson, H.; Gracia-Marco, L.; Labayen, I.; Ortega, F.B.; Huybrechts, I.; Romero, V.E.; Manios, Y.; Widhalm, K.; Dallongeville, J.; et al. Prevalence of ideal cardiovascular health in European adolescents: The HELENA study. Int. J. Cardiol. 2017, 240, 428–432. [Google Scholar] [CrossRef] [PubMed]
- Leiva, A.M.; Martínez, M.A.; Cristi-Montero, C.; Salas, C.; Ramírez-Campillo, R.; Martínez, X.D.; Aguilar-Farías, N.; Celis-Morales, C. El sedentarismo se asocia a un incremento de factores de riesgo cardiovascular y metabólicos independiente de los niveles de actividad física. Revista médica de Chile 2017, 145, 458–467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Väistö, J.; Eloranta, A.-M.; Viitasalo, A.; Tompuri, T.T.; Lintu, N.; Karjalainen, P.; Lampinen, E.-K.; Ågren, J.; Laaksonen, D.E.; Lakka, H.-M.; et al. Physical activity and sedentary behaviour in relation to cardiometabolic risk in children: Cross-sectional findings from the Physical Activity and Nutrition in Children (PANIC) Study. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 55. [Google Scholar] [CrossRef] [Green Version]
- Del Pozo-Cruz, J.; García-Hermoso, A.; Alfonso-Rosa, R.M.; Alvarez-Barbosa, F.; Owen, N.; Chastin, S.; Del Pozo-Cruz, B. Replacing Sedentary Time: Meta-analysis of Objective-Assessment Studies. Am. J. Prev. Med. 2018, 55, 395–402. [Google Scholar] [CrossRef]
- Lee, D.-C.; Pate, R.R.; Lavie, C.J.; Sui, X.; Church, T.S.; Blair, S.N. Leisure-Time Running Reduces All-Cause and Cardiovascular Mortality Risk. J. Am. Coll. Cardiol. 2014, 64, 472–481. [Google Scholar] [CrossRef] [Green Version]
- Lacombe, J.; Armstrong, M.E.G.; Wright, F.L.; Foster, C. The impact of physical activity and an additional behavioural risk factor on cardiovascular disease, cancer and all-cause mortality: A systematic review. BMC Public Health 2019, 19, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Whitaker, K.M.; Buman, M.P.; Odegaard, A.; Carpenter, K.C.; Jacobs, D.R.; Sidney, S.; Pereira, M.A. Sedentary Behaviors and Cardiometabolic Risk: An Isotemporal Substitution Analysis. Am. J. Epidemiol. 2018, 187, 181–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palenzuela-Luis, N.; Gónzalez-Abreu, J.; Sánchez Gómez, M.B. Competencias enfermeras sobre el diagnóstico riesgo de deterioro de la función cardiovascular. Revista Iberoamericana de Enfermería Comunitaria 2017, 10, 40–51. [Google Scholar]
- Simão, A.F.; Precoma, D.B.; Andrade, J.P.; Correa, F.H.; Saraiva, J.F.K.; Oliveira, G.M.M.; Murro, A.L.B.; Campos, A.; Alessi, A.; Avezum Jr, A.; et al. I Diretriz Brasileira de Prevenção Cardiovascular. Arquivos Brasileiros de Cardiología 2013, 101 (Suppl. 2), 1–63. [Google Scholar] [CrossRef]
- Teston, E.F.; Cecilio, H.P.M.; Santos, A.L.; Arruda, G.O.; Radovanovic, C.A.T.; Marcon, S.S. Fatores associados às doenças cardiovascu-lares em adultos. Medicina 2016, 49, 95–102. [Google Scholar]
- Mohd-Nor, N.; Bit-Lian, Y. Knowledge, Attitude and Practices of Standard Precaution among Nurses in Middle-East Hospital. SciMed. J. 2019, 1, 189–198. [Google Scholar] [CrossRef]
- Zalite, G.G.; Zvirbule, A. Digital Readiness and Competitiveness of the EU Higher Education Institutions: The COVID-19 Pandemic Impact. Emerg. Sci. J. 2020, 4, 297–304. [Google Scholar] [CrossRef]
- Gamble, B.; Crouse, D. Strategies for Supporting and Building Student Resilience in Canadian Secondary and Post-Secondary Educational Institutions. SciMed. J. 2020, 2, 70–76. [Google Scholar] [CrossRef]
- Okunlola, M.A.; Lamptey, E.; Senkyire, E.K.; Dorcas, S.; Dooshima, B.A. Perceived Myths and Misconceptions about the Novel COVID-19 Outbreak. SciMed. J. 2020, 2, 108–117. [Google Scholar] [CrossRef]
- De Castro-Sampaio, F.; De Oliveira, P.P.; Da Mata, L.R.F.; Moraes, J.T.; Da Fonseca, D.F.; de Sousa Vieira, V.A. Profile of nursing diagnoses in people with hypertension and diabetes. Invest. Educ. Enferm. 2017, 35, 139–153. [Google Scholar] [CrossRef] [Green Version]
- Sartori, A.A.; Gaedke, M.Â.; Moreira, A.C.; Graeff, M.D.S. Nursing diagnoses in the hemodynamics sector: An adaptive perspective. Rev. Esc. Enferm. USP 2018, 52, e03381. [Google Scholar] [CrossRef]
- D’Agostino, F.; Zeffiro, V.; Vellone, E.; Ausili, D.; Belsito, R.; Leto, A.; Alvaro, R. Cross-Mapping of Nursing Care Terms Recorded in Italian Hospitals into the Standardized NNN Terminology. Int. J. Nurs. Knowl. 2020, 31, 4–13. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Rivas, F.J.; Martín-García, Á.; Sánz-Bayona, M.T.; Fernández-Díaz, M.C.; Barberá-Martín, A.; Cárdenas-Valladolid, J.; López-Palacios, S.; Rico-Blázquez, M. Establishing Technical Values for Nursing Diagnoses in Primary Healthcare. Int. J. Nurs. Knowl. 2019, 31, 124–133. [Google Scholar] [CrossRef] [PubMed]
- Butcher, H.; Bulechek, G.; Dochterman, J.M.; Wagner, C.H. Nursing Interventions Classification (NIC), 7th ed.; Elsevier: St. Louis, MO, USA, 2018. [Google Scholar]
- Moorhead, S.; Swanson, E.; Johnson, M.; Maas, M.L. Nursing Outcomes Classification (NOC). Measurement of Health Outcomes, 6th ed.; Elsevier: St. Louis, MO, USA, 2018. [Google Scholar]


{kind=link}
| Risk Factor | Source | GS 1 | F Ratio 2 | K Index 3 | I-K Interpretation |
|---|---|---|---|---|---|
| Diabetes Mellitus | Interview/Laboratory value | Laboratory value | 1 | 1 | Very good |
| Dyslipidemia | Interview/Laboratory value | Laboratory value | 0.53 | 0.5 | Moderate |
| Family history of CVD | Interview | Interview | 0.98 | 0.93 | Very good |
| Individual history of CVD | Interview | Interview | 0.6 | 0.72 | Good |
| Arterial hypertension | Interview/Physical examination | Physical examination | 0.93 | 0.83 | Very good |
| Lack of knowledge of modifiable risk factors | Interview | Interview | 0.79 | 0.9 | Very Good |
| Obesity | Interview/Physical examination | Physical examination | 0.92 | 0.97 | Very Good |
| Pharmacological agents | Interview | Interview | 0.98 | 0.93 | Very Good |
| Sedentarism | Interview | Interview | 0.96 | 0.99 | Very Good |
| Smoking habit | Interview | Interview | 0.94 | 1 | Very Good |
| Factors’ mean | 0.86 | 0.96 | Very Good | ||
| RICF 4 | Interview/Physical examination/Laboratory value | Interview/Physical examination/Laboratory value | 0.89 | 0.92 | Very Good |
| Students with Cardiovascular Risk | Students without Cardiovascular Risk | |
|---|---|---|
| Clinical judgement | n = 320 | n = 14 |
| Physical examination | n = 15 | n = 15 |
| Variable Outcome | Nursing Diagnosis: Risk of Impaired Cardiovascular Function | p-Value 1 | ||||
|---|---|---|---|---|---|---|
| Predictive Variables | Present | Absent | Total | |||
| n | [%] | n | [%] | |||
| Age group | ||||||
| ≥25 years old | 67 | [23.7] | 12 | [27.3] | 79 [23.7] | 0.544 |
| 18–24 years old | 223 | [76.9] | 32 | [72.7] | 255 [76.3] | |
| Nationality | ||||||
| Brazilian | 183 | [63.1] | 07 | [15.9] | 190 [56.9] | 0.000 * |
| International | 107 | [36.9] | 37 | [84.1] | 144 [43.1] | |
| Sex | ||||||
| Female | 162 | [55.9] | 11 | [25.0] | 173 [51.8] | 0.000 * |
| Male | 128 | [44.1] | 33 | [75.0] | 161 [48.2] | |
| Skin color | ||||||
| Yellow, White or Brown | 179 | [61.7] | 11 | [25.0] | 190 [56.9] | 0.000 * |
| Black | 111 | [38.3] | 33 | [75.0] | 144 [43.1] | |
| Marital status | ||||||
| Married/stable union | 17 | [5.9] | 00 | [0.0] | 17 [5.1] | 0.099 |
| Single | 273 | [94.1] | 44 | [100.0] | 317 [94.9] | |
| Living with | ||||||
| Friends or alone | 193 | [66.6] | 37 | [84.1] | 230 [68.9] | 0.019 * |
| Family or Partner | 97 | [33.4] | 07 | [15.9] | 104 [31.1] | |
| Occupation | ||||||
| Scholarship, formal, or informal job | 67 | [23.1] | 07 | [15.9] | 74 [22.2] | 0.284 |
| Unemployed Student | 223 | [76.9] | 37 | [84.1] | 260 [77.8] | |
| Nationality | Brazilian (n = 190) | p-Value 1 | International (n = 144) | p-Value 1 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Diagnosis | Present | Absent | Present | Absent | ||||||
| n | % | n | % | n | % | n | % | |||
| Age group | ||||||||||
| ≥25 years old | 36 | 19.7 | 01 | 14.3 | 0.724 | 31 | 29.2 | 11 | 29.7 | 0.930 |
| 18–24 years old | 147 | 80.3 | 06 | 85.7 | 76 | 71.0 | 26 | 70.3 | ||
| Sex | ||||||||||
| Female | 114 | 62.3 | 01 | 14.3 | 0.011 * | 48 | 44.9 | 10 | 40.3 | 0.057 |
| Male | 69 | 37.7 | 06 | 85.7 | 59 | 55.1 | 27 | 73.0 | ||
| Skin color | ||||||||||
| Yellow/White/Brown | 159 | 86.9 | 06 | 85.7 | 0.928 | 20 | 18.7 | 05 | 13.5 | 0.473 |
| Black | 24 | 13.1 | 01 | 14.3 | 87 | 81.3 | 32 | 86.5 | ||
| Marital status | ||||||||||
| Married/stable union | 14 | 7.7 | 00 | 0.0 | 0.447 | 03 | 2.8 | 00 | 0.0 | 0.303 |
| Single | 169 | 92.3 | 07 | 100 | 104 | 97.2 | 37 | 100 | ||
| Living with | ||||||||||
| Fiends or Alone | 93 | 50.8 | 04 | 57.1 | 0.743 | 100 | 93.5 | 33 | 89.2 | 0.399 |
| Family or Partner | 90 | 49.2 | 03 | 42.9 | 07 | 6.5 | 04 | 2.8 | ||
| Occupation | ||||||||||
| Scholarship/worker | 47 | 25.7 | 01 | 14.3 | 0.496 | 20 | 18.7 | 06 | 16.2 | 0.736 |
| Unemployed Student | 136 | 74.3 | 06 | 85.7 | 87 | 81.3 | 31 | 83.8 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Duarte-Clíments, G.; Mauricio, T.F.; Gómez-Salgado, J.; Moreira, R.P.; Romero-Martín, M.; Sánchez-Gómez, M.B. Assessment of Cardiovascular Risk Factors in Young Adults through the Nursing Diagnosis: A Cross-Sectional Study among International University Students. Healthcare 2021, 9, 91. https://doi.org/10.3390/healthcare9010091
Duarte-Clíments G, Mauricio TF, Gómez-Salgado J, Moreira RP, Romero-Martín M, Sánchez-Gómez MB. Assessment of Cardiovascular Risk Factors in Young Adults through the Nursing Diagnosis: A Cross-Sectional Study among International University Students. Healthcare. 2021; 9(1):91. https://doi.org/10.3390/healthcare9010091
Chicago/Turabian StyleDuarte-Clíments, Gonzalo, Tibelle Freitas Mauricio, Juan Gómez-Salgado, Rafaella Pessoa Moreira, Macarena Romero-Martín, and María Begoña Sánchez-Gómez. 2021. "Assessment of Cardiovascular Risk Factors in Young Adults through the Nursing Diagnosis: A Cross-Sectional Study among International University Students" Healthcare 9, no. 1: 91. https://doi.org/10.3390/healthcare9010091