The Association between Dietary Variety and Physical Frailty in Community-Dwelling Older Adults


 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
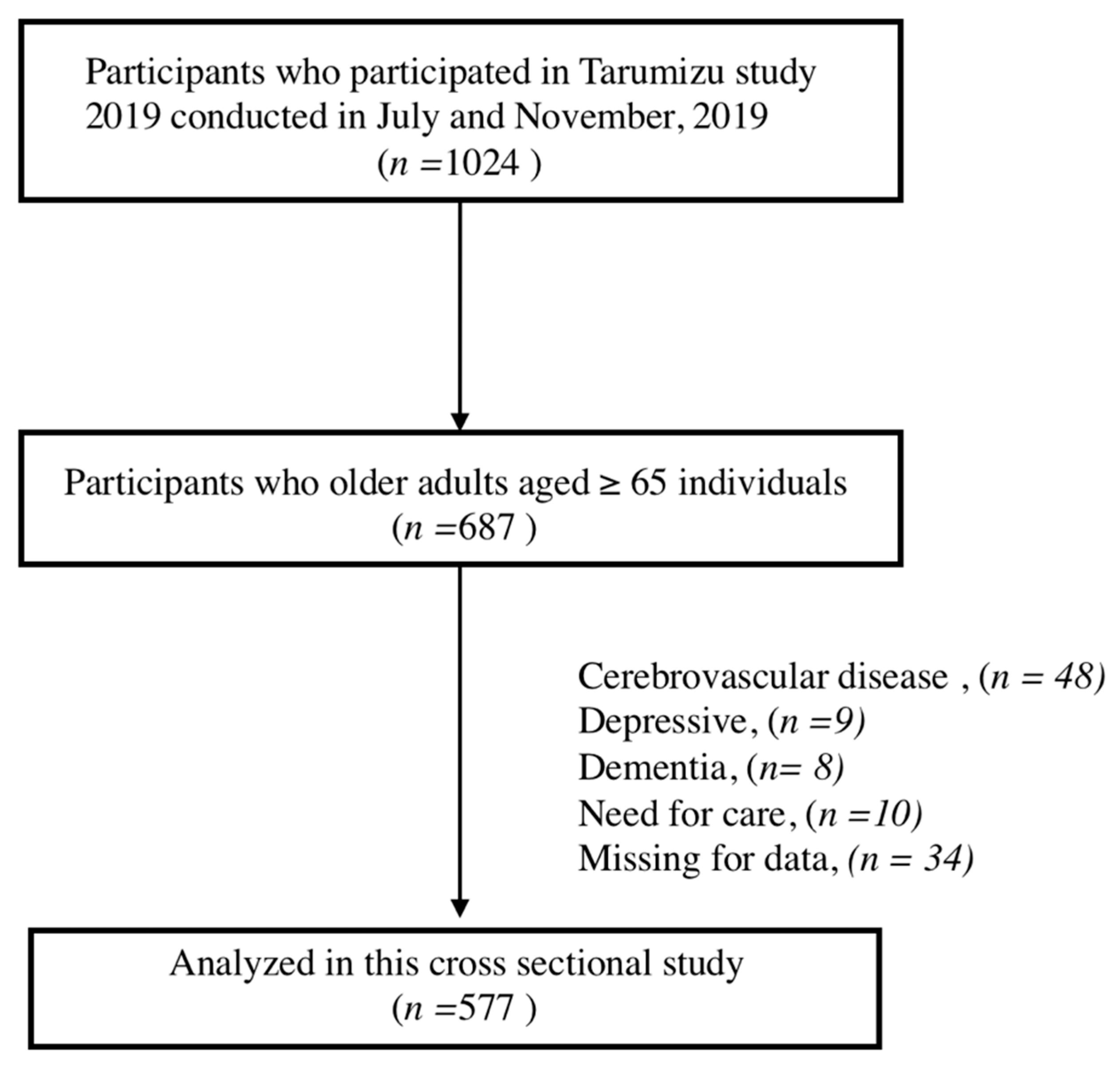
2.1. Participants
2.2. Measures
2.2.1. Physical Frailty
2.2.2. Assessment of Diet Variety
2.2.3. Demographic Variables and Covariates
2.2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Participants According to Frail Status
3.2. Association between Physical Frailty and Diet Score
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hoogendijk, E.O.; Afilalo, J.; Ensrud, K.E.; Kowal, P.; Onder, G.; Fried, L.P. Frailty: Implications for clinical practice and public health. Lancet 2019, 394, 1365–1375. [Google Scholar] [CrossRef]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef] [Green Version]
- Makizako, H.; Shimada, H.; Doi, T.; Tsutsumimoto, K.; Suzuki, T. Impact of physical frailty on disability in community-dwelling older adults: A prospective cohort study. BMJ Open 2015, 5, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Kelaiditi, E.; Van Kan, G.A.; Cesari, M. Frailty: Role of nutrition and exercise. Curr. Opin. Clin. Nutr. Metab. Care 2014, 17, 32–39. [Google Scholar] [CrossRef]
- Rasheed, S.; Woods, R.T. Malnutrition and quality of life in older people: A systematic review and meta-analysis. Ageing Res. Rev. 2013, 12, 561–566. [Google Scholar] [CrossRef]
- Ramsey, K.A.; Meskers, C.G.M.; Trappenburg, M.C.; Verlaan, S.; Reijnierse, E.M.; Whittaker, A.C.; Maier, A.B. Malnutrition is associated with dynamic physical performance. Aging Clin. Exp. Res. 2020, 32, 1085–1092. [Google Scholar] [CrossRef] [Green Version]
- Kant, A.K. Dietary patterns and health outcomes. J. Am. Diet. Assoc. 2004, 104, 615–635. [Google Scholar] [CrossRef]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef]
- Kant, A.K.; Schatzkin, A.; Graubard, B.I.; Schairer, C. A prospective study of diet quality and mortality in women. J. Am. Med. Assoc. 2000, 283, 2109–2115. [Google Scholar] [CrossRef] [Green Version]
- Kurotani, K.; Akter, S.; Kashino, I.; Goto, A.; Mizoue, T.; Noda, M.; Sasazuki, S.; Sawada, N.; Tsugane, S. Quality of diet and mortality among Japanese men and women: Japan Public Health Center based prospective study. BMJ 2016, 352. [Google Scholar] [CrossRef] [Green Version]
- Slattery, M.L. Defining dietary consumption: Is the sum greater than its parts? Am. J. Clin. Nutr. 2008, 88, 14–15. [Google Scholar] [CrossRef]
- Milte, C.M.; Ball, K.; Crawford, D.; McNaughton, S.A. Diet quality and cognitive function in mid-aged and older men and women. BMC Geriatr. 2019, 19, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Chan, R.; Leung, J.; Woo, J. A Prospective Cohort Study to Examine the Association Between Dietary Patterns and Sarcopenia in Chinese Community-Dwelling Older People in Hong Kong. J. Am. Med. Dir. Assoc. 2016, 17, 336–342. [Google Scholar] [CrossRef] [PubMed]
- Bollwein, J.; Diekmann, R.; Kaiser, M.J.; Bauer, J.M.; Uter, W.; Sieber, C.C.; Volkert, D. Dietary quality is related to frailty in community-dwelling older adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2013, 68, 483–489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsuyama, S.; Sawada, N.; Tomata, Y.; Zhang, S.; Goto, A.; Yamaji, T.; Iwasaki, M.; Inoue, M.; Tsuji, I.; Tsugane, S. Association between adherence to the Japanese diet and all-cause and cause-specific mortality: The Japan Public Health Center-based Prospective Study. Eur. J. Nutr. 2020. [Google Scholar] [CrossRef] [PubMed]
- Nomura, S.; Sakamoto, H.; Glenn, S.; Tsugawa, Y.; Abe, S.K.; Rahman, M.M.; Brown, J.C.; Ezoe, S.; Fitzmaurice, C.; Inokuchi, T.; et al. Population health and regional variations of disease burden in Japan, 1990–2015: A systematic subnational analysis for the Global Burden of Disease Study 2015. Lancet 2017, 390, 1521–1538. [Google Scholar] [CrossRef] [Green Version]
- Kobayashi, M.; Sasazuki, S.; Shimazu, T.; Sawada, N.; Yamaji, T.; Iwasaki, M.; Mizoue, T.; Tsugane, S. Association of dietary diversity with total mortality and major causes of mortality in the Japanese population: JPHC study. Eur. J. Clin. Nutr. 2020, 74, 54–66. [Google Scholar] [CrossRef]
- Suthutvoravut, U.; Takahashi, K.; Murayama, H.; Tanaka, T.; Akishita, M.; Iijima, K. Association Between Traditional Japanese Diet Washoku and Sarcopenia in Community-Dwelling Older Adults: Findings from the Kashiwa Study. J. Nutr. Heal. Aging 2020, 24, 282–289. [Google Scholar] [CrossRef]
- Tsuji, T.; Yamamoto, K.; Yamasaki, K.; Hayashi, F.; Momoki, C.; Yasui, Y.; Ohfuji, S.; Fukushima, W.; Habu, D. Lower dietary variety is a relevant factor for malnutrition in older Japanese home-care recipients: A cross-sectional study. BMC Geriatr. 2019, 19, 1–8. [Google Scholar] [CrossRef]
- Kimura, M.; Moriyasu, A.; Kumagai, S.; Furuna, T.; Akita, S.; Kimura, S.; Suzuki, T. Community-based intervention to improve dietary habits and promote physical activity among older adults: A cluster randomized trial. BMC Geriatr. 2013, 13, 8. [Google Scholar] [CrossRef] [Green Version]
- Taniguchi, Y.; Makizako, H.; Kiyama, R.; Tomioka, K.; Nakai, Y.; Kubozono, T.; Takenaka, T.; Ohishi, M. The association between osteoporosis and grip strength and skeletal muscle mass in community-dwelling older women. Int. J. Environ. Res. Public Health 2019, 16, 1228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Makizako, H.; Kubozono, T.; Kiyama, R.; Takenaka, T.; Kuwahata, S.; Tabira, T.; Kanoya, T.; Horinouchi, K.; Shimada, H.; Ohishi, M. Associations of social frailty with loss of muscle mass and muscle weakness among community-dwelling older adults. Geriatr. Gerontol. Int. 2019, 19, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Nakai, Y.; Makizako, H.; Kiyama, R.; Tomioka, K.; Taniguchi, Y.; Kubozono, T.; Takenaka, T.; Ohishi, M. Association between chronic pain and physical frailty in community-dwelling older adults. Int. J. Environ. Res. Public Health 2020, 17, 1330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in Older Adults: Evidence for a Phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M157. [Google Scholar] [CrossRef]
- Satake, S.; Shimada, H.; Yamada, M.; Kim, H.; Yoshida, H.; Gondo, Y.; Matsubayashi, K.; Matsushita, E.; Kuzuya, M.; Kozaki, K.; et al. Prevalence of frailty among community-dwellers and outpatients in Japan as defined by the Japanese version of the Cardiovascular Health Study criteria. Geriatr. Gerontol. Int. 2017, 17, 2615–2616. [Google Scholar] [CrossRef]
- Shimada, H.; Makizako, H.; Doi, T.; Yoshida, D.; Tsutsumimoto, K.; Anan, Y.; Uemura, K.; Ito, T.; Lee, S.; Park, H.; et al. Combined Prevalence of Frailty and Mild Cognitive Impairment in a Population ofElderly Japanese People. J. Am. Med. Dir. Assoc. 2013, 14, 518–524. [Google Scholar] [CrossRef]
- Chen, L.K.; Liu, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Bahyah, K.S.; Chou, M.Y.; Chen, L.Y.; Hsu, P.S.; Krairit, O.; et al. Sarcopenia in Asia: Consensus report of the Asian working group for sarcopenia. J. Am. Med. Dir. Assoc. 2014, 15, 95–101. [Google Scholar] [CrossRef]
- Fukutomi, E.; Okumiya, K.; Wada, T.; Sakamoto, R.; Ishimoto, Y.; Kimura, Y.; Chen, W.L.; Imai, H.; Kasahara, Y.; Fujisawa, M.; et al. Relationships between each category of 25-item frailty risk assessment (Kihon Checklist) and newly certified older adults under Long-Term Care Insurance: A 24-month follow-up study in a rural community in Japan. Geriatr. Gerontol. Int. 2015, 15, 864–871. [Google Scholar] [CrossRef]
- Kojima, T.; Akishita, M.; Kameyama, Y.; Yamaguchi, K.; Yamamoto, H.; Eto, M.; Ouchi, Y. High risk of adverse drug reactions in elderly patients taking six or more drugs: Analysis of inpatient database. Geriatr. Gerontol. Int. 2012, 12, 761–762. [Google Scholar] [CrossRef]
- Akobeng, A.K. Understanding diagnostic tests 3: Receiver operating characteristic curves. Acta Paediatr. Int. J. Paediatr. 2007, 96, 644–647. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean Diet and Survival in a Greek Population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Granic, A.; Sayer, A.A.; Robinson, S.M. Dietary patterns, skeletal muscle health, and sarcopenia in older adults. Nutrients 2019, 11, 745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milaneschi, Y.; Bandinelli, S.; Corsi, A.M.; Lauretani, F.; Paolisso, G.; Dominguez, L.J.; Semba, R.D.; Tanaka, T.; Abbatecola, A.M.; Talegawkar, S.A.; et al. Mediterranean diet and mobility decline in older persons. Exp. Gerontol. 2011, 46, 303–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yokoyama, Y.; Nishi, M.; Murayama, H.; Amano, H.; Taniguchi, Y.; Nofuji, Y.; Narita, M.; Matsuo, E.; Seino, S.; Kawano, Y.; et al. Association of dietary variety with body composition and physical function in community-dwelling elderly Japanese. J. Nutr. Heal. Aging 2016, 20, 691–696. [Google Scholar] [CrossRef] [PubMed]
- Mendonça, N.; Kingston, A.; Granic, A.; Jagger, C. Protein intake and transitions between frailty states and to death in very old adults: The Newcastle 85+ study. Age Ageing 2019, 49, 32–38. [Google Scholar] [CrossRef] [Green Version]
- Hernández Morante, J.J.; Martínez, C.G.; Morillas-Ruiz, J.M. Dietary factors associated with frailty in old adults: A review of nutritional interventions to prevent frailty development. Nutrients 2019, 11, 102. [Google Scholar] [CrossRef] [Green Version]
- Volpi, E.; Kobayashi, H.; Sheffield-Moore, M.; Mittendorfer, B.; Wolfe, R.R. Essential amino acids are primarily responsible for the amino acid stimulation of muscle protein anabolism in healthy elderly adults. Am. J. Clin. Nutr. 2003, 78, 250–258. [Google Scholar] [CrossRef]
- Hackney, K.J.; Trautman, K.; Johnson, N.; McGrath, R.; Stastny, S. Protein and muscle health during aging: Benefits and concerns related to animal-based protein. Anim. Front. 2019, 9, 12–17. [Google Scholar] [CrossRef] [Green Version]
- Aspell, N.; Laird, E.; Healy, M.; Lawlor, B.; O’sullivan, M. Vitamin D deficiency is associated with impaired muscle strength and physical performance in community-dwelling older adults: Findings from the english longitudinal study of ageing. Clin. Interv. Aging 2019, 14, 1751–1761. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, K.; Nashimoto, M.; Okuda, Y.; Ota, T.; Yamamoto, M. Fish as a major source of vitamin D in the Japanese diet. Nutrition 2002, 18, 415–416. [Google Scholar] [CrossRef]
- Hashimoto, R.; Sakai, A.; Murayama, M.; Ochi, A.; Abe, T.; Hirasaka, K.; Ohno, A.; Teshima-Kondo, S.; Yanagawa, H.; Yasui, N.; et al. Effects of dietary soy protein on skeletal muscle volume and strength in humans with various physical activities. J. Med. Investig. 2015, 62, 177–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khairallah, R.J.; O’Shea, K.M.; Ward, C.W.; Butteiger, D.N.; Mukherjea, R.; Krul, E.S. Chronic dietary supplementation with soy protein improves muscle function in rats. PLoS ONE 2017, 12, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, R.; Leung, J.; Woo, J. Associations of Dietary Protein Intake on Subsequent Decline. J. Nutr. Health Aging 2014, 18, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Beasley, J.M.; Lacroix, A.Z.; Neuhouser, M.L.; Huang, Y.; Tinker, L.; Woods, N.; Michael, Y.; Curb, J.D.; Prentice, R.L. Protein intake and incident frailty in the women’s health initiative observational study. J. Am. Geriatr. Soc. 2010, 58, 1063–1071. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perry, G.; Nunomura, A.; Hirai, K.; Zhu, X.; Prez, M.; Avila, J.; Castellani, R.J.; Atwood, C.S.; Aliev, G.; Sayre, L.M.; et al. Is oxidative damage the fundamental pathogenic mechanism of Alzheimer’s and other neurodegenerative diseases? Free Radic. Biol. Med. 2002, 33, 1475–1479. [Google Scholar] [CrossRef]
- Floyd, R.A.; Hensley, K. Oxidative stress in brain aging: Implications for therapeutics of neurodegenerative diseases. Neurobiol. Aging 2002, 23, 795–807. [Google Scholar] [CrossRef]
- Bartali, B.; Frongillo, E.A.; Guralnik, J.M.; Stipanuk, M.H.; Allore, H.G.; Cherubini, A.; Bandinelli, S.; Ferrucci, L.; Gill, T.M. Serum micronutrient concentrations and decline in physical function among older persons. JAMA J. Am. Med. Assoc. 2008, 299, 308–315. [Google Scholar] [CrossRef] [Green Version]
- Kobayashi, S.; Suga, H.; Sasaki, S. Diet with a combination of high protein and high total antioxidant capacity is strongly associated with low prevalence of frailty among old Japanese women: A multicenter cross-sectional study. Nutr. J. 2017, 16, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Yokoyama, Y.; Nishi, M.; Murayama, H.; Amano, H.; Taniguchi, Y.; Nofuji, Y.; Narita, M.; Matsuo, E.; Seino, S.; Kawano, Y.; et al. Dietary variety and decline in lean mass and physical performance in community-dwelling older Japanese: A 4-year follow-up study. J. Nutr. Heal. Aging 2017, 21, 11–16. [Google Scholar] [CrossRef]
- Kumagai, S.; Watanabe, S.; Shibata, H.; Amano, H.; Fujiwara, Y.; Shinkai, S.; Yoshida, H.; Suzuki, T.; Yukawa, H.; Yasumura, S.; et al. Effects of dietary variety on declines in high-level functional capacity in elderly people living in a community. Nihon Koshu Eisei Zasshi 2003, 50, 1117–1124. [Google Scholar] [CrossRef]
- Rodrigo, C.P.; Aranceta, J.; Salvador, G.; Varela-Moreiras, G. Food Frequency Questionnaires. Nutr. Hosp. 2015, 31, 49–56. [Google Scholar] [CrossRef]
- Narita, M.; Kitamura, A.; Yukari, T.; Yokoyama, Y.; Morita, A.; Shoji, S. Food diversity and its relationship with nutrient intakes and meal days involving staple foods, main dishes, and side dishes in community-dwelling elderly adults. Jpn. J. Public Health 2020, 67, 171–182. [Google Scholar]
- Shahar, S.; Vanoh, D.; Mat Ludin, A.F.; Singh, D.K.A.; Hamid, T.A. Factors associated with poor socioeconomic status among Malaysian older adults: An analysis according to urban and rural settings. BMC Public Health 2019, 19, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Variable | Overall | Non-Frailty | Pre-Frailty | Frailty | p |
|---|---|---|---|---|---|
| (n = 577) | (n = 268) | (n = 271) | (n = 38) | ||
| Age (years) | 74.0 ± 6.3 | 72.4 ± 5.2 | 74.9 ± 6.7 | 78.3 ± 7.4 | <0.01 |
| Women, n (%) | 361, (62.5%) | 181, (67.5%) | 152, (56.1%) | 28, (73.7%) | 0.02 |
| Education (years) | 11.5 ± 2.2 | 11.8 ± 2.0 | 11.4 ± 2.4 | 10.1 ± 1.8 | <0.01 |
| BMI, kg/m2 | 23.1 ± 3.2 | 23.0 ± 3.0 | 23.3 ± 3.3 | 22.4 ± 3.9 | 0.25 |
| Medication (n/day) | 3.1 ± 3.0 | 2.3 ± 2.6 | 3.6 ± 3.1 | 5.0 ± 3.7 | <0.01 |
| FFS | 20.3 ± 4.6 | 21.2 ± 4.4 | 19.7 ± 4.7 | 18.4 ± 4.5 | <0.01 |
| Chronic disease, n (%) | |||||
| Hypertension | 317, (55.0%) | 135, (50.4%) | 156, (57.6%) | 26, (68.4%) | 0.02 |
| Diabetes mellitus | 72, (12.5%) | 21, (7.8%) | 46, (17.0%) | 5, (13.2%) | <0.01 |
| Hyperlipidemia | 162, (28.0%) | 73, (27.2%) | 76, (28.0%) | 13, (34.2%) | 0.47 |
| Dependent Value: Presence of Physical Frailty | ||||
|---|---|---|---|---|
| Independent Variable | Model 1 | Model 2 | ||
| OR | (95% CI) | OR | (95% CI) | |
| FFS | 0.89 ** | (0.83–0.96) | 0.90 * | (0.84–0.97) |
| Age | 1.11 ** | (1.01–1.17) | 1.09 ** | (1.03–1.15) |
| Sex (women) | 1.95 | (0.89–4.26) | 1.59 | (0.71–3.56) |
| Educations | 0.79 * | (0.65–0.96) | ||
| BMI | 0.89 * | (0.80–0.99) | ||
| polypharmacy (vs. 6 or less medications) | 1.50 | (0.69–3.28) | ||
| Dependent Value: Each of Subitems of Physical Frailty | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Independent Variable | Weight Loss | Exhaustion | Physical Inactivity | Weakness | Slowness | |||||
| OR | (95% CI) | OR | (95% CI) | OR | (95% CI) | OR | (95% CI) | OR | (95% CI) | |
| FFS | 0.95 * | (0.91–1.00) | 0.98 | (0.93–1.03) | 0.90 ** | (0.86–0.95) | 0.91 ** | (0.87–0.96) | 0.87 ** | (0.82–0.93) |
| Age | 1.01 | (0.97–1.04) | 1.01 | (0.98–1.05) | 1.02 | (0.99–1.06) | 1.16 ** | (1.16–1.20) | 1.21 ** | (1.15–1.27) |
| Sex (women) | 0.68 | (0.43–1.06) | 0.88 | (0.56–1.38) | 0.66 | (0.42–1.06) | 1.72 * | (1.06–2.78) | 2.11 * | (1.05–4.23) |
| Dependent Value: Presence of Physical Frailty | ||||
|---|---|---|---|---|
| Independent Variable | Model 1 | Model 2 | ||
| OR | (95% CI) | OR | (95% CI) | |
| Food frequency score | ||||
| FFS > 17 | Reference | Reference | ||
| FFS < 16 | 3.87 ** | (1.85–8.07) | 3.46 * | (1.60–7.50) |
| Age | 1.11 ** | (1.05–1.16) | 1.08 * | (1.02–1.14) |
| Sex (women) | 2.04 | (0.93–4.45) | 1.69 | (0.75–3.81) |
| Educations | 0.79 * | (0.65–0.97) | ||
| BMI | 0.89 * | (0.80–0.99) | ||
| polypharmacy (vs. 6 or less medications) | 1.49 | (0.68–3.26) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kiuchi, Y.; Makizako, H.; Nakai, Y.; Tomioka, K.; Taniguchi, Y.; Kimura, M.; Kanouchi, H.; Takenaka, T.; Kubozono, T.; Ohishi, M. The Association between Dietary Variety and Physical Frailty in Community-Dwelling Older Adults. Healthcare 2021, 9, 32. https://doi.org/10.3390/healthcare9010032
Kiuchi Y, Makizako H, Nakai Y, Tomioka K, Taniguchi Y, Kimura M, Kanouchi H, Takenaka T, Kubozono T, Ohishi M. The Association between Dietary Variety and Physical Frailty in Community-Dwelling Older Adults. Healthcare. 2021; 9(1):32. https://doi.org/10.3390/healthcare9010032
Chicago/Turabian StyleKiuchi, Yuto, Hyuma Makizako, Yuki Nakai, Kazutoshi Tomioka, Yoshiaki Taniguchi, Mika Kimura, Hiroaki Kanouchi, Toshihiro Takenaka, Takuro Kubozono, and Mitsuru Ohishi. 2021. "The Association between Dietary Variety and Physical Frailty in Community-Dwelling Older Adults" Healthcare 9, no. 1: 32. https://doi.org/10.3390/healthcare9010032