Prevalence and Associated Factors of Malnutrition and Sarcopenia in a Daycare Facility: A Cross-Sectional Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Population
2.2. Diagnosis of Malnutrition
2.3. Diagnosis of Sarcopenia
2.4. Assessment of Covariates
2.5. Statistical Analyses
3. Results
3.1. Population and Diagnosis of Malnutrition and Sarcopenia
3.2. Evaluation of Comorbid Conditions and Daily Physical Activity
3.3. Factors Associated with Malnutrition and Sarcopenia
3.4. Factors Associated with Nutrition Status and Sarcopenia
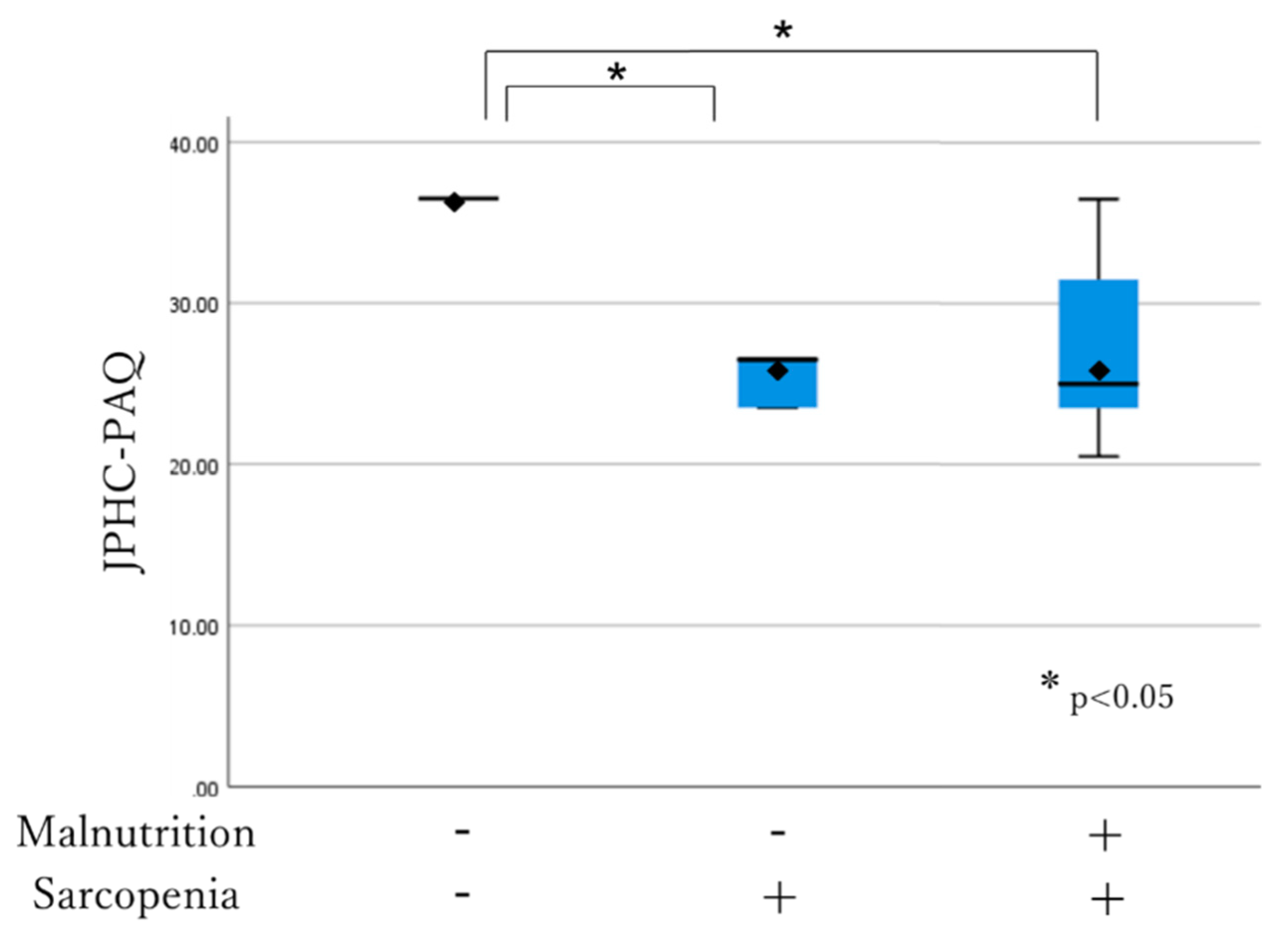
3.5. MNA-SF Score, Comorbidity, JPHC-PAQ Association with Nutritional and Sarcopenia Status
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Cederholm, T.; Bosaeus, I.; Barazzoni, R.; Bauer, J.; Van Gossum, A.; Klek, S.; Muscaritoli, M.; Nyulasi, I.; Ockenga, J.; Schneider, S.M.; et al. Diagnostic criteria for malnutrition- an ESPEN consensus statement. Clin. Nutr. 2015, 34, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Söderström, L.; Rosenblad, A.; Adolfsson, E.T.; Bergkvist, L. Malnutrition is associated with increased mortality in older adults regardless of the cause of death. Br. J. Nutr. 2017, 117, 532–540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malafarina, V.; Reginster, J.Y.; Cabrerizo, S.; Bruyère, O.; Kanis, J.A.; Martinez, J.A.; Zulet, M.A. Nutritional status and nutritional treatment are related to outcomes and mortality in older adults with hip fracture. Nutrients 2018, 10, 555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Volkert, D.; Beck, A.M.; Cederholm, T.; Cruz-Jentoft, A.; Goisser, S.; Hooper, L.; Kiesswetter, E.; Maggio, M.; Raynaud-Simon, A.; Sieber, C.C.; et al. ESPEN guideline on clinical nutrition and hydration in geriatrics. Clin. Nutr. 2018, 38, 10–47. [Google Scholar] [CrossRef] [Green Version]
- Morley, J.E. Anorexia, weight loss, and frailty. J. Am. Med. Dir. Assoc. 2010, 11, 225–228. [Google Scholar] [CrossRef]
- Fried, L.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar]
- Sánchez-Rodríguez, D.; Marco, E.; Ronquillo-Moreno, N.; Maciel-Bravo, L.; Gonzales-Carhuancho, A.; Duran, X.; Guillén-Solà, A.; Vázquez-Ibar, O.; Escalada, F.; Muniesa, J.M. ASPEN-AND-ESPEN: A postacute-care comparison of the basic definition of malnutrition from the American Society of Parenteral and Enteral Nutrition and Academy of Nutrition and Dietetics with the European Society for Clinical Nutrition and Metabolism definition. Clin. Nutr. 2019, 38, 297–302. [Google Scholar]
- Sanchez-Rodriguez, D.; Locquet, M.; Reginster, J.Y.; Cavalier, E.; Bruyère, O.; Beaudart, C. Mortality in malnourished older adults diagnosed by ESPEN and GLIM criteria in the SarcoPhAge study. J. Cachexia Sarcopenia Muscle 2020, 11, 1200–1211. [Google Scholar] [CrossRef]
- Maeda, K.; Ishida, Y.; Nonogaki, T.; Mori, N. Reference body mass index values and the prevalence of malnutrition according to the Global Leadership Initiative on Malnutrition criteria. Clin. Nutr. 2020, 39, 180–184. [Google Scholar] [CrossRef]
- Morley, J.E.; Abbatecola, A.M.; Argiles, J.M.; Baracos, V.; Bauer, J.; Bhasin, S.; Cederholm, T.; Coats, A.J.; Cummings, S.R.; Evans, W.J.; et al. Sarcopenia with limited mobility: An international consensus. J. Am. Med. Dir. Assoc. 2011, 12, 403–409. [Google Scholar] [CrossRef] [Green Version]
- Landi, F.; Cruz-Jentoft, A.J.; Liperoti, R.; Russo, A.; Giovannini, S.; Tosato, M.; Capoluongo, E.; Bernabei, R.; Onder, G. Sarcopenia and mortality risk in frail older persons aged 80 years and older: Results from ilSIRENTE study. Age Ageing 2013, 42, 203–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landi, F.; Liperoti, R.; Russo, A.; Giovannini, S.; Tosato, M.; Barillaro, C.; Capoluongo, E.; Bernabei, R.; Onder, G. Association of anorexia with sarcopenia in a community-dwelling elderly population: Results from the ilSIRENTE study. Eur. J. Nutr. 2013, 52, 1261–1268. [Google Scholar] [CrossRef]
- Lee, W.J.; Liu, L.K.; Peng, L.N.; Lin, M.H.; Chen, L.K. Comparisons of sarcopenia defined by IWGS and EWGSOP criteria among older people: Results from the I-Lan longitudinal aging study. J. Am. Med. Dir. Assoc. 2013, 14, 528.e1–528.e7. [Google Scholar] [CrossRef] [PubMed]
- Legrand, D.; Vaes, B.; Mathei, C.; Swine, C.; Degryse, J.M. The prevalence of sarcopenia in very old individuals according to the European consensus definition: Insights from the BELFRAIL study. Age Ageing 2013, 42, 727–734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, R.A.; Ip, E.H.; Zhang, Q.; Boudreau, R.M.; Cawthon, P.M.; Newman, A.B.; Tylavsky, F.A.; Visser, M.; Goodpaster, B.H.; Harris, T.B.; et al. Transition to sarcopenia and determinants of transitions in older adults: A population-based study. J. Gerontol. A Biol. Sci. Med. Sci. 2014, 69, 751–758. [Google Scholar] [CrossRef]
- Patel, H.P.; Syddall, H.E.; Jameson, K.; Robinson, S.; Denison, H.; Roberts, H.C.; Edwards, M.; Dennison, E.; Cooper, C.; Aihie Sayer, A. Prevalence of sarcopenia in community-dwelling older people in the UK using the European Working Group on Sarcopenia in Older People (EWGSOP) definition: Findings from the Hertfordshire Cohort Study (HCS). Age Ageing 2013, 42, 378–384. [Google Scholar] [CrossRef] [Green Version]
- Tanimoto, Y.; Watanabe, M.; Sun, W.; Sugiura, Y.; Tsuda, Y.; Kimura, M.; Hayashida, I.; Kusabiraki, T.; Kono, K. Association between sarcopenia and higher-level functional capacity in daily living in community-dwelling elderly subjects in Japan. Arch. Gerontol. Geriatr. 2012, 55, e9–e13. [Google Scholar] [CrossRef] [PubMed]
- Volpato, S.; Bianchi, L.; Cherubini, A.; Landi, F.; Maggio, M.; Savino, E.; Bandinelli, S.; Ceda, G.P.; Guralnik, J.M.; Zuliani, G.; et al. Prevalence and clinical correlates of sarcopenia in community-dwelling older people: Application of the EWGSOP definition and diagnostic algorithm. J. Gerontol. A Biol. Sci. Med. Sci. 2014, 69, 438–446. [Google Scholar] [CrossRef]
- Bastiaanse, L.P.; Hilgenkamp, T.I.; Echteld, M.A.; Evenhuis, H.M. Prevalence and associated factors of sarcopenia in older adults with intellectual disabilities. Res. Dev. Disabil. 2012, 33, 2004–2012. [Google Scholar] [CrossRef]
- Landi, F.; Liperoti, R.; Fusco, D.; Mastropaolo, S.; Quattrociocchi, D.; Proia, A.; Russo, A.; Bernabei, R.; Onder, G. Prevalence and risk factors of sarcopenia among nursing home older residents. J. Gerontol. A Biol. Sci. Med. Sci. 2012, 67, 48–55. [Google Scholar] [CrossRef] [Green Version]
- Senior, H.E.; Henwood, T.R.; Beller, E.M.; Mitchell, G.K.; Keogh, J.W. Prevalence and risk factors of sarcopenia among adults living in nursing homes. Maturitas 2015, 82, 418–423. [Google Scholar] [CrossRef] [Green Version]
- Bahat, G.; Saka, B.; Tufan, F.; Akin, S.; Sivrikaya, S.; Yucel, N.; Erten, N.; Karan, M.A. Prevalence of sarcopenia and its association with functional and nutritional status among male residents in a nursing home in Turkey. Aging Male 2010, 13, 211–214. [Google Scholar] [CrossRef] [PubMed]
- Gariballa, S.; Alessa, A. Sarcopenia: Prevalence and prognostic significance in hospitalized patients. Clin. Nutr. 2013, 32, 772–776. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Landi, F.; Schneider, S.M.; Zúñiga, C.; Arai, H.; Boirie, Y.; Chen, L.K.; Fielding, R.A.; Martin, F.C.; Michel, J.P.; et al. Prevalence of and interventions for sarcopenia in ageing adults: A systematic review. Report of the International Sarcopenia Initiative (EWGSOP and IWGS). Age Ageing 2014, 43, 748–759. [Google Scholar] [CrossRef] [PubMed]
- Verschueren, S.; Gielen, E.; O’Neill, T.W.; Pye, S.R.; Adams, J.E.; Ward, K.A.; Wu, F.C.; Szulc, P.; Laurent, M.; Claessens, F.; et al. Sarcopenia and its relationship with bone mineral density in middle-aged and elderly European men. Osteoporos. Int. 2013, 24, 87–98. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.K.; Liu, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Bahyah, K.S.; Chou, M.Y.; Chen, L.Y.; Hsu, P.S.; Krairit, O.; et al. Sarcopenia in Asia: Consensus report of the Asian Working Group for Sarcopenia. J. Am. Med. Dir. Assoc. 2014, 15, 95–101. [Google Scholar] [CrossRef]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307. [Google Scholar] [CrossRef]
- Sieber, C.C. Malnutrition and sarcopenia. Aging Clin. Exp. Res. 2019, 31, 793–798. [Google Scholar] [CrossRef]
- HP of the Japan Ministry of Health, Labour and Welfare. Available online: https://www.mhlw.go.jp/content/10904750/000340975.pdf (accessed on 29 November 2020).
- Statistics of Long-Term Care Benefit Expenditures. Available online: https://www.mhlw.go.jp/toukei/itiran/eiyaku.html (accessed on 22 February 2020). (In Japanese).
- Orellana, K.; Manthorpe, J.; Tinker, A. Day centres for older people: A systematically conducted scoping review of literature about their benefits, purposes and how they are perceived. Ageing Soc. 2018, 41, 1–32. [Google Scholar] [CrossRef] [Green Version]
- Jensen, G.L.; Cederholm, T.; Correia, M.I.T.; Fukushima, R.; Higashiguchi, T.; De Baptista, G.A.; Barazzoni, R.; Blaauw, R.; Coats, A.J.; Crivelli, A.; et al. GLIM criteria for the diagnosis of malnutrition–a consensus report from the global clinical nutrition community. J. Parenter. Enteral. Nutr. 2019, 43, 32–40. [Google Scholar] [CrossRef] [Green Version]
- Woo, J.; Leung, J.; Morley, J.E. Validating the SARC-F: A suitable community screening tool for sarcopenia? J. Am. Med. Dir. Assoc. 2014, 15, 630–634. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Jiang, J.; Zeng, Y.; Tang, H. Sarcopenia for predicting mortality among elderly nursing home residents: SARC-F versus SARC-CalF. Medicine 2019, 98, e14546. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Fujii, H.; Yamamoto, S.; Takeda-Imai, F. Validity and applicability of a simple questionnaire for the estimation of total and domain-specific physical activity. Diabetol. Int. 2011, 2, 47–54. [Google Scholar] [CrossRef]
- Kikuchi, H.; Inoue, S.; Odagiri, Y.; Ihira, H.; Inoue, M.; Sawada, N.; Noda, M.; Tsugane, S. Intensity-specific validity and reliability of the Japan Public Health Center-based prospective study-physical activity questionnaire. Prev. Med. Rep. 2020, 20, 101169. [Google Scholar]
- Sasai, H.; Nakata, Y.; Murakami, H.; Kawakami, R.; Nakae, S.; Tanaka, S.; Ishikawa-Takata, K.; Yamada, Y.; Miyachi, M. Simultaneous validation of seven physical activity questionnaires used in Japanese cohorts for estimating energy expenditure: A doubly labeled water study. J. Epidemiol. 2018, 28, 437–442. [Google Scholar] [CrossRef] [Green Version]
- Ishikawa-Takata, K.; Naito, Y.; Tanaka, S.; Ebine, N.; Tabata, I. Use of doubly labeled water to validate a physical activity questionnaire developed for the Japanese population. J. Epidemiol. 2011, 21, 114–121. [Google Scholar] [CrossRef] [Green Version]
- Hayasaka, S.; Shibata, Y.; Ishikawa, S.; Kayaba, K.; Gotoh, T.; Noda, T.; Murata, C.; Yamada, T.; Goto, Y.; Nakamura, Y.; et al. Physical activity and all-cause mortality in Japan: The Jichi Medical School (JMS) cohort study. J. Epidemiol. 2009, 19, 24–27. [Google Scholar] [CrossRef] [Green Version]
- Bellanti, F.; Lo Buglio, A.; Quiete, S.; Pellegrino, G.; Dobrakowski, M.; Kasperczyk, A.; Kasperczyk, S.; Vendemiale, G. Comparison of Three Nutritional Screening Tools with the New Glim Criteria for Malnutrition and Association with Sarcopenia in Hospitalized Older Patients. J. Clin. Med. 2020, 9, 1898. [Google Scholar] [CrossRef]
- Gomi, I.; Sugiyama, M.; Kajii, F. Protein-Energy Malnutrition in complexed nursing facility. Jpn. J. Health Nutr. Syst. 2005, 4, 147–156. [Google Scholar]
- Deutz, N.E.P.; Bauer, J.M.; Barazzoni, R.; Biolo, G.; Boirie, Y.; Bosy-Westphal, A.; Cederholm, T.; Cruz-Jentoft, A.; Krznariç, Z.; Nair, K.S.; et al. Protein intake and exercise for optimal muscle function with aging: Recommendations from the ESPEN Expert Group. Clin. Nutr. 2014, 33, 929–936. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bauer, J.M.; Biolo, G.; Cederholm, T.; Cesari, M.; Cruz-Jentoft, A.J.; Morley, J.E.; Phillips, S.; Sieber, C.; Stehle, P.; Teta, D.; et al. Evidence-based recommendations for optimal dietary protein intake in older people: A position paper from the PROT-AGE Study Group. J. Am. Med. Dir. Assoc. 2013, 14, 542–559. [Google Scholar] [CrossRef] [PubMed]
- Wakabayashi, H. Rehabilitation nutrition in general and family medicine. J. Gen. Fam. Med. 2017, 18, 153–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wakabayashi, H.; Sashika, H. Association of nutrition status and rehabilitation outcome in the disuse syndrome: A Retrospective Cohort Study. Gen. Med. 2011, 12, 69–74. [Google Scholar] [CrossRef]
- Wakabayashi, H. Presbyphasia and sarcopenic dysphasia: Association between aging, sarcopenia, and deglutition disorders. J. Frailty Aging 2014, 3, 97–103. [Google Scholar] [PubMed]
- Wakabayashi, H.; Sakura, K. Rehabilitation nutrition for sarcopenia with disability: A combination of both rehabilitation and nutrition care management. J. Cachexia Sarcopenia Muscle 2014, 5, 269–277. [Google Scholar] [CrossRef]
- Mori, T.; Fujishima, I.; Wakabayashi, H.; Itoda, M.; Kunieda, K.; Kayashita, J.; Nishioka, S.; Sonoda, A.; Kuroda, Y.; Yamada, M. Development, reliability, and validity of a diagnostic algorithm for sarcopenicdysphasia. J. CSM Clin. Rep. 2017, 2, e00017. [Google Scholar]
- Chen, Y.C.; Chen, P.Y.; Wang, Y.C.; Wang, T.G. Decreased swallowing function in the sarcopenic elderly without clinical dysphagia: A cross-sectional study. BMC Geriatr. 2020, 20, 419. [Google Scholar] [CrossRef]
- Japan Ministry of Internal Affairs and Communications. Available online: https://www.stat.go.jp/data/topics/topi1261.html (accessed on 1 December 2020).
- Naruse, T.; Kitano, A.; Matsumoto, H.; Nagata, S. A Logic Model for Evaluation and Planning in an Adult Day Care for Disabled Japanese Old People. Int. J. Environ. Res. Public Health 2020, 17, 2061. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total (n = 62) | |
|---|---|---|
| Age, years, mean (SD) | 86.6 (7.0) | |
| Female sex, n (%) | 46 (74.2) | |
| Nursing care level, n (%) | grade1 | 4 (6.5) |
| grade2 | 5 (8.1) | |
| grade3 | 10 (16.1) | |
| grade4 | 20 (32.3) | |
| grade5 | 14 (22.6) | |
| grade6 | 9 (14.5) | |
| grade7 | 0 (0.0) | |
| BMI, kg/m2, mean (SD) | 23.6 (4.1) | |
| BMI category, n (%) | underweight (<22) | 23 (37.1) |
| normal weight (22–25) | 15 (24.2) | |
| overweight (>25) | 24 (38.7) | |
| MNA-SF, n (%) | malnourished | 2 (3.2) |
| at risk of malnutrition | 34 (54.8) | |
| wellnourished | 26 (41.9) | |
| GLIM, n (%) | malnourished | 37 (59.7) |
| wellnourished | 25 (40.3) | |
| Sarcopenia, n (%) | no-sarcopenia | 8 (12.9) |
| sarcopenia | 15 (24.2) | |
| severe sarcopenia | 39 (62.9) | |
| JPHC-PAQ score, mean (SD) | 28.1 (6.0) | |
| Charlson Comorbidity Index, mean (SD) | 1.1 (1.1) |
| Mean (±SD) | GLIM Criteria | p-Value | |
|---|---|---|---|
| Well Nourished (n = 37) | Malnourished (n = 25) | ||
| Age years * | 84.92 (7.1) | 89.24 (6.2) | 0.0017 |
| Nursing care level | 2.95 (1.2) | 3.08 (1.5) | 0.71 |
| BMI, kg/m2 * | 25.34 (3.6) | 21.13 (3.6) | <0.001 |
| MNA-SF * | 11.89 (1.5) | 9.88 (3.6) | <0.001 |
| Charlson Comorbidity Index | 0.94 (1.1) | 1.28 (1.1) | 0.259 |
| JPHC-PAQ score | 28.79 (6.1) | 27.25 (5.7) | 0.332 |
| CC (cm) * | 33.65 (3.2) | 29.6 (2.1) | <0.001 |
| Hand grip strength (kg) | 14.25 (5.3) | 12.8 (6.4) | 0.343 |
| Five time chairstand up test (s) | 15.91 (7.0) | 15.37 (5.5) | 0.797 |
| SARC-F | 3.37 (3.0) | 4.68 (3.5) | 0.129 |
| SARC-CaIF * | 7.97 (6.1) | 14.68 (3.5) | <0.001 |
| TUG (s) | 16.03 (7.0) | 17.27 (5.2) | 0.574 |
| Mean(±SD) | AWGS2019 | p-Value | |
|---|---|---|---|
| Non-Sarcopenia (n = 9) | Sarcopenia (n = 53) | ||
| Age years | 84.11 (6.3) | 87.09 (7.1) | 0.24 |
| Nursing care level * | 2.33 (0.7) | 3.11 (1.4) | 0.018 |
| BMI, kg/m2 * | 28.01 (2.8) | 22.90 (3.9) | <0.001 |
| MNA-SF * | 13.11 (1.0) | 10.73 (1.7) | <0.001 |
| Charlson Comorbidity Index | 0.66 (0.7) | 1.15 (1.1) | 0.259 |
| JPHC-PAQ score * | 33.61 (5.7) | 27.22 (5.5) | 0.01 |
| CC (cm) * | 36.22 (2.9) | 31.31 (3.0) | <0.001 |
| Hand grip strength (kg) * | 18.87 (5.5) | 12.78 (5.3) | 0.003 |
| Five time chairstand up test (s) * | 12.21 (2.2) | 16.66 (6.9) | 0.003 |
| SARC-F * | 0.55 (0.8) | 4.47 (3.2) | <0.001 |
| SARC-CaIF * | 0.55(0.8) | 12.39 (4.8) | <0.001 |
| TUG (s) * | 12.08 (2.2) | 17.65 (6.7) | 0.021 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shiota, A.; Nakayama, N.; Saito, Y.; Maeda, T.; Maeda, Y.; Nakayama, K. Prevalence and Associated Factors of Malnutrition and Sarcopenia in a Daycare Facility: A Cross-Sectional Study. Healthcare 2020, 8, 576. https://doi.org/10.3390/healthcare8040576
Shiota A, Nakayama N, Saito Y, Maeda T, Maeda Y, Nakayama K. Prevalence and Associated Factors of Malnutrition and Sarcopenia in a Daycare Facility: A Cross-Sectional Study. Healthcare. 2020; 8(4):576. https://doi.org/10.3390/healthcare8040576
Chicago/Turabian StyleShiota, Aya, Naomi Nakayama, Yuki Saito, Tamako Maeda, Yukie Maeda, and Kentaro Nakayama. 2020. "Prevalence and Associated Factors of Malnutrition and Sarcopenia in a Daycare Facility: A Cross-Sectional Study" Healthcare 8, no. 4: 576. https://doi.org/10.3390/healthcare8040576