Professional Quality of Life and Perceived Stress in Health Professionals before COVID-19 in Spain: Primary and Hospital Care


 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Instruments
2.3. Procedure
2.4. Ethical Considerations
2.5. Data Analysis
3. Results
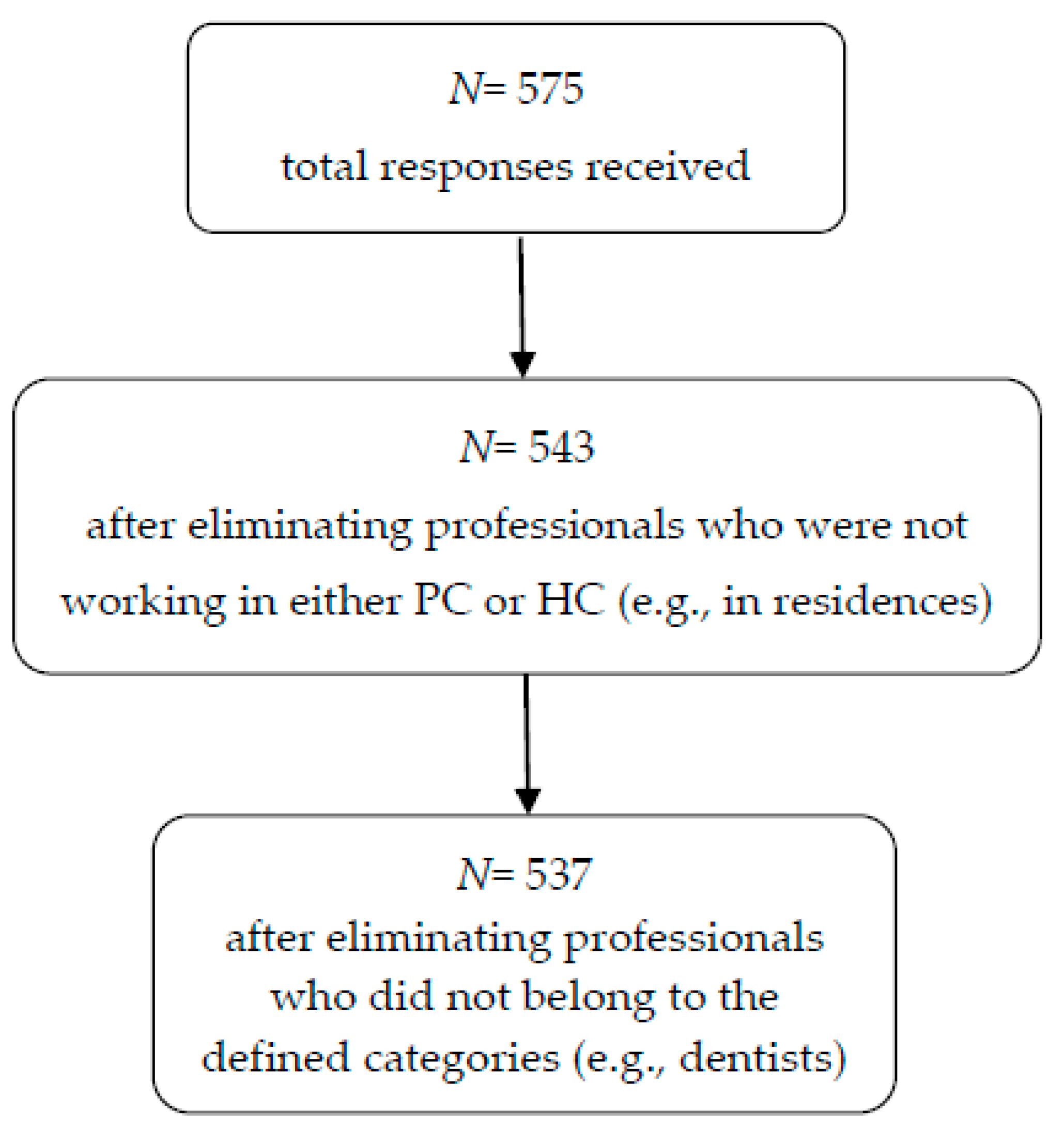
3.1. Socio-Demographic Characteristics of the Participants
3.2. Professional Quality of Life and Perceived Stress in PC and HC Professionals
3.3. Correlations between the Professional Quality of Life Subscales and the Perceived Stress Scale
4. Discussion
Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Rothan, H.A.; Byrareddy, S.N. The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak. J. Autoimmun 2020, 109, 102433. [Google Scholar] [CrossRef] [PubMed]
- Tejedor, S.; Cervi, L.; Tusa, F.; Portales, M.; Zabotina, M. Information on the COVID-19 Pandemic in Daily Newspapers’ Front Pages: Case Study of Spain and Italy. Int. J. Env. Res. Public Health 2020, 17, 6330. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.C.; Wang, C.Y.; Wang, Y.H.; Hsueh, S.C.; Ko, W.C.; Hsueh, P.R. Global epidemiology of coronavirus disease 2019 (COVID-19): Disease incidence, daily cumulative index, mortality, and their association with country healthcare resources and economic status. Int. J. Antimicrob. Agents 2020, 55, 105946. [Google Scholar] [CrossRef] [PubMed]
- Xiang, Y.T.; Yang, Y.; Li, W.; Zhang, L.; Zhang, Q.; Cheung, T.; Ng, C.H. Timely mental health care for the 2019 novel coronavirus outbreak is urgently needed. Lancet Psychiatry 2020, 7, 228–229. [Google Scholar] [CrossRef] [Green Version]
- Shanafelt, T.; Ripp, J.; Trockel, M. Understanding and Addressing Sources of Anxiety among Health Care Professionals during the COVID-19 Pandemic. JAMA 2020, 323, 2133–2134. [Google Scholar] [CrossRef]
- Rivas-García, F. Bioética y profesionales sanitarios en el abordaje de la pandemia provocada por COVID-19 en España. Rev. Iberoam. Bioét. 2020, 13, 1–14. [Google Scholar] [CrossRef]
- O’Neill, D.J. Covid-19: Clinicians need continuing professional development in ethics. BMJ 2020, 370, m2793. [Google Scholar] [CrossRef]
- Alharbi, J.; Jackson, D.; Usher, K. The potential for COVID-19 to contribute to compassion fatigue in critical care nurses. J. Clin. Nurs. 2020, 29, 2762–2764. [Google Scholar] [CrossRef]
- Montemurro, N. The emotional impact of COVID-19: From medical staff to common people. Brain Behav. Immun. 2020, 87, 23–24. [Google Scholar] [CrossRef]
- Roney, L.N.; Acri, M.C. The Cost of Caring: An Exploration of Compassion Fatigue, Compassion Satisfaction, and Job Satisfaction in Pediatric Nurses. J. Pediatr. Nurs. 2018, 40, 74–80. [Google Scholar] [CrossRef]
- Stamm, B. The Professional Quality of Life Scale: Compassion Satisfaction, Burnout & Compassion Fatigue/Secondary Trauma Scales; The Center for Victims of Torture: Lutherville, MD, USA, 2005; Available online: https://www.proqol.org/ (accessed on 20 September 2020).
- Ruiz-Fernández, M.D.; Pérez-García, E.; Ortega-Galán, Á.M. Quality of life in nursing professionals: Burnout, fatigue, and compassion satisfaction. Int. J. Environ. Res. Public Health 2020, 17, 1253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodrigues, H.; Cobucci, R.; Oliveira, A.; Cabral, J.V.; Medeiros, L.; Gurgel, K.; Souza, T.; Gonçalves, A.K. Burnout syndrome among medical residents: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0206840. [Google Scholar] [CrossRef] [Green Version]
- Alharbi, J.; Jackson, D.; Usher, K. Personal characteristics, coping strategies, and resilience impact on compassion fatigue in critical care nurses: A cross-sectional study. Nurs. Health Sci. 2020, 22, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Kweon, Y. Psychological Capital Mediates the Association between Job Stress and Burnout of among Korean Psychiatric Nurses. Healthcare 2020, 8, 199. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Fernández, M.D.; Ramos-Pichardo, J.D.; Ibáñez-Masero, O.; Cabrera-Troya, J.; Carmona-Rega, M.I.; Ortega-Galán, Á.M. Compassion fatigue, burnout, compassion satisfaction and perceived stress in healthcare professionals during the COVID-19 health crisis in Spain. J. Clin. Nurs. 2020, 29, 4321–4330. [Google Scholar] [CrossRef] [PubMed]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors Associated With Mental Health Outcomes Among Health Care Workers Exposed to Coronavirus Disease 2019. JAMA Netw. Open. 2020, 3, e203976. [Google Scholar] [CrossRef] [PubMed]
- Berlinger, N.; Wynia, M.; Powell, T.; Micah Hester, D.; Milliken, A.; Fabi, R.; Jenks, N.P. Source Ethical Framework for Health Care Institutions Responding to Novel Coronavirus SARS-CoV-2 (COVID-19). Guidelines for Institutional Ethics Services Responding to COVID-19 Managing Uncertainty, Safeguarding Communities, Guiding Practice; The Hastings Center: Garrison, NY, USA, 2020. [Google Scholar]
- Galiana, L.; Arena, F.; Oliver, A.; Sansó, N.; Benito, E. Compassion Satisfaction, Compassion Fatigue, and Burnout in Spain and Brazil: ProQoL Validation and Cross-cultural Diagnosis. J. Pain Symptom. Manag. 2017, 53, 598–604. [Google Scholar] [CrossRef] [Green Version]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Remor, E. Psychometric properties of a European Spanish version of the Perceived Stress Scale (PSS). Span J. Psychol. 2006, 9, 86–93. [Google Scholar] [CrossRef] [Green Version]
- Andalusian Health Service. Andalusian Health Service Staff. Available online: https://www.sspa.juntadeandalucia.es/servicioandaluzdesalud/archivo-estadisticas/plantilla-del-servicio-andaluz-de-salud-3 (accessed on 12 November 2020).
- Zhang, Y.Y.; Han, W.L.; Qin, W.; Yin, H.X.; Zhang, C.F.; Kong, C.; Wang, Y.L. Extent of compassion satisfaction, compassion fatigue and burnout in nursing: A meta-analysis. J. Nurs. Manag. 2018, 26, 810–819. [Google Scholar] [CrossRef]
- Powell, S.K. Compassion Fatigue. Prof. Case Manag. 2020, 25, 53–55. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Padilla, J.M.; Ruiz-Fernández, M.D.; Granero-Molina, J.; Ortíz-Amo, R.; López Rodríguez, M.M.; Fernández-Sola, C. Perceived health, caregiver overload and perceived social support in family caregivers of patients with Alzheimer’s: Gender differences. Health Soc. Care Community 2020, 1–9. [Google Scholar] [CrossRef]
- Portero de la Cruz, S.; Cebrino, J.; Herruzo, J.; Vaquero-Abellán, M. A Multicenter Study into Burnout, Perceived Stress, Job Satisfaction, Coping Strategies, and General Health among Emergency Department Nursing Staff. J. Clin. Med. 2020, 9, 1007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coronado-Vázquez, V.; Gómez-Salgado, J. The error of not planning public health emergencies. Gac. Sanit. 2020, 34, 416. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.O.S.; Ping, L.; Wah-Pun Sin, E. The effects of nonconventional palliative and end-of-life care during COVID-19 pandemic on mental health-Junior doctors’ perspective. Psychol. Trauma 2020, 12, S146–S147. [Google Scholar] [CrossRef]
- Sacco, T.L.; Copel, L.C. Compassion satisfaction: A concept analysis in nursing. Nurs. Forum. 2018, 53, 76–83. [Google Scholar] [CrossRef]
- Brito-Pons, G.; Librada-Flores, S. Compassion in palliative care: A review. Curr. Opin. Support Palliat. Care 2018, 12, 472–479. [Google Scholar] [CrossRef]
- Li, Z.; Ge, J.; Yang, M.; Feng, J.; Liu, C.; Yang, C. Vicarious traumatization: A psychological problem that cannot be ignored during the COVID-19 pandemic. Brain Behav. Immun. 2020, 87, 74. [Google Scholar] [CrossRef]
- Liang, Y.; Chen, M.; Zheng, X.; Liu, J. Screening for Chinese medical staff mental health by SDS and SAS during the outbreak of COVID-19. J. Psychosom. Res. 2020, 133, 110102. [Google Scholar] [CrossRef]
- Joob, B.; Wiwanitkit, V. Traumatization in medical staff helping with COVID-19 control. Brain Behav. Immun. 2020, 87, 10. [Google Scholar] [CrossRef]
- Carbone, S.R. Flattening the curve of mental ill-health: The importance of primary prevention in managing the mental health impacts of COVID-19. Ment. Health Prev. 2020, 19, 200185. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Fernández, M.D.; Ortíz-Amo, R.; Ortega-Galán, Á.M.; Ibáñez-Masero, O.; Rodríguez-Salvador, M.d.M.; Ramos-Pichardo, J.D. Mindfulness therapies on health professionals. Int. J. Ment. Health Nurs. 2020, 29, 127–140. [Google Scholar]
- Auserón, G.A.; Viscarret, M.R.E.; Goñi, C.F.; Rubio, V.G.; Pascual, P.P.; Galdeano, E.S.D.M.G.D. Evaluation of the effectiveness of a Mindfulness and Self-Compassion program to reduce stress and prevent burnout in Primary Care health professionals. Aten. Primaria 2018, 50, 141–150. [Google Scholar] [CrossRef]
- Hevezi, J.A. Evaluation of a Meditation Intervention to Reduce the Effects of Stressors Associated With Compassion Fatigue Among Nurses. J. Holist. Nurs. 2016, 34, 343–350. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Variables | HC | PC | Mann–Whitney U |
|---|---|---|---|---|
| Age (years) | 44.29 ± 9.71 | 49.70 ± 9.74 | 26,999.50 | |
| Gender | Female | 226 (76.9%) | 178 (73.3%) | |
| Male | 68 (23.1%) | 65 (26.7%) | ||
| Marital status | Married/Domestic partner | 193 (65.6%) | 199 (8.6%) | 23,400.50 *** |
| Single | 35 (11.9%) | 21 (8.6%) | ||
| Widowed/Divorced | 66 (22.4%) | 23 (9.5%) | ||
| Profession | Nurse | 215 (73.1%) | 160 (65.8%) | 25,772.50 |
| Doctor | 43 (14.6%) | 65 (26.7%) | ||
| Technicians | 36 (12.2%) | 18 (7.4%) | ||
| Type of employment contract | Permanent | 137 (46.6%) | 153 (63%) | 22,179.00 *** |
| Temporary | 157 (53.4%) | 90 (37%) | ||
| Work shift | Rotating without nights | 47 (16%) | 3 (1.2%) | 15,159.50 *** |
| Daytime with nights/guards | 162 (55.1%) | 93 (38.3%) | ||
| Constant day shift | 79 (26.9%) | 147 (60.5%) | ||
| Constant night shift | 6 (2%) | 0% |
| Variables | Variables | HC | PC | Mann–Whitney U | ||
|---|---|---|---|---|---|---|
| Mean ± SD | N (%) | Mean ± SD | N (%) | |||
| CS | 39.58 (6.25) | 38.98 (6.64) | 25,450.50 | |||
| Low | 42 (14.3%) | 42 (17.2%) | ||||
| Medium | 127 (43.2%) | 106 (43.6%) | ||||
| High | 125 (42.5%) | 95 (39.1%) | ||||
| CF | 19.64 (7.59) | 19.87 (7.75) | 27,698.00 | |||
| Low | 21 (7.1%) | 14 (5.8%) | ||||
| Medium | 84 (28.6%) | 14 (30.5%) | ||||
| High | 189 (64.3%) | 155 (63.8%) | ||||
| BO | 24.70 (5.96) | 24.43 (6.05) | 27,094.00 | |||
| Low | 45 (15.3%) | 45 (18.5%) | ||||
| Medium | 141 (48%) | 116 (47.7%) | ||||
| High | 108 (36.7%) | 82 (33.7%) | ||||
| PSS-14 | 25.98 (9.16) | 26.44 (9.21) | ||||
| Characteristcs | Variables | CS | CF | BO | PSS-14 | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variables | Variables | HC | PC | HC | PC | HC | PC | HC | PC | ||||||||
| Mean ± SD | p-Value | Mean ± SD | p-Value | Mean ± SD | p-Value | Mean ± SD | p-Value | Mean ± SD | p-Value | Mean ± SD | p-Value | Mean ± SD | p-value | Mean ± SD | p-Value | ||
| Gender | Female | 39.52 ± 6.52 | 0.767 a | 39.19 ± 6.03 | 0.475 a | 20.18 ± 7.51 | 0.028 a,* | 20.21 ± 7.81 | 0.252 a | 24.95 ± 5.80 | 0.191 a | 24.77 ± 6.04 | 0.151 a | 27.02 ± 9.17 | 0.000 a,** | 27.06 ± 6.40 | 0.130 a |
| Male | 39.78 ± 5.34 | 38.40 ± 8.12 | 17.87 ± 7.67 | 18.92 ± 7.59 | 23.87 ± 6.46 | 23.51 ± 6.04 | 22.54 ± 8.33 | 24.75 ± 11.03 | |||||||||
| Marital Status | Married | 39.25 ± 5.56 | 0.777 b | 39.01 ± 6.59 | 0.960 b | 20.13 ± 7.55 | 0.218 b | 19.76 ± 7.67 | 0.651 b | 24.83 ± 5.85 | 0.603 b | 24.25 ± 5.84 | 0.168 b | 26.32 ± 8.66 | 0.689 b | 26.07 ± 9.36 | 0.414 b |
| Single | 38.97 ± 7.55 | 39.10 ± 6.73 | 19.57 ± 7.33 | 19.38 ± 8.27 | 23.74 ± 6.24 | 23.71 ± 6.91 | 25.46 ± 10.00 | 28.14 ± 9.32 | |||||||||
| Widowed/Divorced | 39.58 ± 7.42 | 38.61 ± 7.23 | 18.24 ± 7.82 | 21.26 ± 8.24 | 24.82 ± 6.19 | 26.65 ± 6.83 | 25.29 ± 10.18 | 28.09 ± 7.74 | |||||||||
| Contract | Permanent | 39.45 ± 6.57 | 0.742 a | 38.32 ± 6.91 | 0.043 a,* | 19.01 ± 7.46 | 0.186 a | 20.01 ± 7.74 | 0.718 a | 23.96 ± 5.97 | 0.049 a,* | 24.41 ± 6.04 | 0.928 a | 24.34 ± 9.01 | 0.004 a,** | 26.18 ± 9.34 | 0.571 a |
| Temporary | 39.69 ± 6.00 | 40.10 ± 6.03 | 20.19 ± 7.70 | 19.63 ± 7.80 | 25.34 ± 5.91 | 24.48.611 | 27.42 ± 9.08 | 26.88 ± 9.04 | |||||||||
| Profession | Nurse | 39.77 ± 6.32 | 0.261 b | 39.82 ± 5.61 | 0.001 b,** | 19.82 ± 7.62 | 0.359 b | 18.99 ± 6.80 | 0.005 b,** | 24.64 ± 5.84 | 0.324 b | 23.99 ± 5.63 | 0.001 b,** | 26.51 ± 9.01 | 0.048 b,* | 26.19 ± 8.54 | 0.005 b,** |
| Doctor | 38.16 ± 6.54 | 36.32 ± 8.12 | 20.16 ± 7.31 | 22.52 ± 9.31 | 25.77 ± 6.47 | 26.51 ± 6.63 | 26.28 ± 9.47 | 28.62 ± 10.66 | |||||||||
| Health technician | 40.14 ± 5.45 | 41.11 ± 6.84 | 17.97 ± 7.83 | 18.11 ± 7.70 | 23.78 ± 6.06 | 20.83 ± 5.22 | 22.47 ± 9.19 | 20.83 ± 6.82 | |||||||||
| Work shift | Dayshift rotating | 40.34 ± 5.47 | 0.661 b | 39.00 ± 1.00 | 0.999 b | 17.23 ± 7.28 | 0.113 b | 16.33 ± 4.04 | 0.775 b | 22.60 ± 4.75 | 0.023 b,* | 24.33 ± 1.16 | 0.470 b | 23.57 ± 9.06 | 0.170 b | 24.00 ± 3.00 | 0.620 b |
| Nights rotating | 39.67 ± 6.46 | 39.00 ± 6.69 | 20.16 ± 7.64 | 20.51 ± 7.19 | 25.07 ± 6.11 | 24.78 ± 6.42 | 25.99 ± 8.88 | 27.12 ± 8.85 | |||||||||
| Constant day shift | 39.05 ± 6.26 | 38.97 ± 6.64 | 19.86 ± 7.57 | 19.54 ± 8.14 | 24.86 ± 5.97 | 24.21 ± 5.89 | 27.32 ± 9.80 | 26.06 ± 9.52 | |||||||||
| Constant night shift | 39.17 ± 7.39 | 21.67 ± 7.37 | 28.83 ± 7.20 | 27.17 ± 6.80 | |||||||||||||
| Variables | All professionals | PC Professionals | HC Professionals | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 1 | 2 | 3 | 4 | 1 | 2 | 3 | 4 | |
| 1. CS | −0.403 ** | −0.563 ** | −0.454 ** | -434 ** | −0.568 ** | −0.499 ** | −0.375 ** | −0.563 | −0.413 | |||
| 2. CF | 0.720 ** | 0.712 ** | 0.714 ** | 0.687 ** | 0.726 ** | 0.733 ** | ||||||
| 3. BO | 0.620 ** | 0.633 ** | 0.611 ** | |||||||||
| 4. PSS-14 | - | |||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ortega-Galán, Á.M.; Ruiz-Fernández, M.D.; Lirola, M.-J.; Ramos-Pichardo, J.D.; Ibáñez-Masero, O.; Cabrera-Troya, J.; Salinas-Pérez, V.; Gómez-Beltrán, P.A.; Fernández-Martínez, E. Professional Quality of Life and Perceived Stress in Health Professionals before COVID-19 in Spain: Primary and Hospital Care. Healthcare 2020, 8, 484. https://doi.org/10.3390/healthcare8040484
Ortega-Galán ÁM, Ruiz-Fernández MD, Lirola M-J, Ramos-Pichardo JD, Ibáñez-Masero O, Cabrera-Troya J, Salinas-Pérez V, Gómez-Beltrán PA, Fernández-Martínez E. Professional Quality of Life and Perceived Stress in Health Professionals before COVID-19 in Spain: Primary and Hospital Care. Healthcare. 2020; 8(4):484. https://doi.org/10.3390/healthcare8040484
Chicago/Turabian StyleOrtega-Galán, Ángela María, María Dolores Ruiz-Fernández, María-Jesús Lirola, Juan Diego Ramos-Pichardo, Olivia Ibáñez-Masero, José Cabrera-Troya, Virginia Salinas-Pérez, Piedras Alba Gómez-Beltrán, and Elia Fernández-Martínez. 2020. "Professional Quality of Life and Perceived Stress in Health Professionals before COVID-19 in Spain: Primary and Hospital Care" Healthcare 8, no. 4: 484. https://doi.org/10.3390/healthcare8040484