Electroacupuncture and Manual Acupuncture Increase Joint Flexibility but Reduce Muscle Strength


Abstract
:1. Introduction
2. Material and Methods
2.1. Participants
2.2. Study Design
2.3. Procedures
2.4. Measurements
2.5. Physical Examination
2.6. Treatments
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kiew Kit, W. Complete Book of Chinese Medicine: A Holistic Approach to Physical, Emotional and Mental Health; Cosmos Internet (Publishing Division): Kedah, Malaysia, 2002; pp. 1–12. [Google Scholar]
- De Carvalho, A.O.; Cabral, L.; Rubini, E. Acupuncture improves flexibility: Acute effect of acupuncture before a static stretch of hip adductors. Med. Acupunct. 2011, 23, 27–33. [Google Scholar] [CrossRef]
- Wilke, J.; Niederer, D.; Hübscher, M.; Rothmayr, J.; Ivkovic, D.; Rickert, M.; Banzer, W. Short-term effects of acupuncture and stretching on myofascial trigger point pain of the neck: A blinded, placebo-controlled RCT. Complement. Ther. Med. 2014, 22, 835–841. [Google Scholar] [CrossRef] [PubMed]
- Tung-wu, L.; Wei, I.P.; Yen-hung, L.; Wei-chun, H.; Ting-ming, W.; Chu-fen, C.; Jaung-geng, L. Immediate effects of acupuncture on gait patterns in patients with knee osteoarthritis. Chin. Med. 2010, 123, 165. [Google Scholar]
- Hübscher, M.; Vogt, L.; Ziebart, T.; Banzer, W. Immediate effects of acupuncture on strength performance: A randomized, controlled crossover trial. Eur. J. Appl. Physiol. 2010, 110, 353–358. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.P.; Zhou, S.; Ao, M.; Zhao, M.L.; Zhang, L.Q.; Cao, L.J. Unilateral intramuscular needling can improve ankle dorsiflexor strength and muscle activation in both legs. J. Exerc. Sci. Fit. 2015, 13, 86–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zanin, M.S.; Ronchi, J.M.; de Castro Silva, T.; Fuzaro, A.C.; de Araujo, J.E. Electromyographic and strength analyses of activation patterns of the wrist flexor muscles after acupuncture. J. Acupunct. Meridian Stud. 2014, 7, 231–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takakura, N.; Yajima, H. Analgesic effect of acupuncture needle penetration: A double-blind crossover study. Open Med. 2009, 3, e54–e61. [Google Scholar]
- Kagitani, F.; Uchida, S.; Hotta, H. Afferent nerve fibers and acupuncture. Auton Neurosci. 2010, 157, 2–8. [Google Scholar] [CrossRef]
- Schuldt, H. The application of nosodes in electroacupuncture according to Voll. Am. J. Acupunct. 1981, 9, 161–164. [Google Scholar]
- Wang, T.Q.; Li, Y.T.; Wang, L.Q.; Shi, G.X.; Tu, J.F.; Yang, J.W.; Hou, Y.Q.; Lin, L.L.; Sun, N.; Zhao, J.J.; et al. Electroacupuncture versus manual acupuncture for knee osteoarthritis: A randomized controlled pilot trial. Acupunct. Med. 2020, 38, 291–300. [Google Scholar] [CrossRef]
- Plaster, R.; Vieira, W.B.; Alencar, F.A.D.; Nakano, E.Y.; Liebano, R.E. Immediate effects of electroacupuncture and manual acupuncture on pain, mobility and muscle strength in patients with knee osteoarthritis: A randomised controlled trial. Acupunct. Med. 2014, 32, 236–241. [Google Scholar] [CrossRef] [PubMed]
- Payton, S.; Bailey, S.D. The effect of manual acupuncture and electroacupuncture on lower limb muscle strength. J. Acupunct. Tuina Sci. 2017, 15, 47–53. [Google Scholar] [CrossRef]
- Tsui, P.; Leung, M.C. Comparison of the effectiveness between manual acupuncture and electro-acupuncture on patients with tennis elbow. Acupunct. Electrother. Res. 2002, 27, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Comachio, J.; Oliveira, C.C.; Silva, I.F.; Magalhaes, M.O.; Marques, A.P. Effectiveness of manual and electrical acupuncture for chronic non-specific low back pain: A randomized controlled trial. Assessment 2020, 26, 27. [Google Scholar] [CrossRef]
- Schliessbach, J.; van der Klift, E.; Arendt-Nielsen, L.; Curatolo, M.; Streitberger, K. The effect of brief electrical and manual acupuncture stimulation on mechanical experimental pain. Pain Med. 2011, 12, 268–275. [Google Scholar] [CrossRef] [Green Version]
- Valenza, M.C.; Torres-Sánchez, I.; Cabrera-Martos, I.; Valenza-Demet, G.; Cano-Cappellacci, M. Acute effects of contract-relax stretching vs. TENS in young subjects with anterior knee pain: A randomized controlled trial. J. Strength Cond. Res. 2016, 30, 2271–2278. [Google Scholar] [CrossRef] [Green Version]
- Gabler, C.M.; Lepley, A.S.; Uhl, T.L.; Mattacola, C.G. Comparison of transcutaneous electrical nerve stimulation and cryotherapy for increasing quadriceps activation in patients with knee Pathologies. J. Sport Rehabil. 2016, 25, 294–300. [Google Scholar] [CrossRef] [Green Version]
- Binkley, J.M.; Stratford, P.W.; Lott, S.A.; Riddle, D.L. The Lower Extremity Functional Scale (LEFS): Scale development, measurement properties, and clinical application. Phys. Ther. 1999, 79, 371–383. [Google Scholar]
- Starkey, C.; Brown, S.D. Examination of Orthopedic & Athletic Injuries; FA Davis: Philadelphia, PA, USA, 2015; pp. 421–467. [Google Scholar]
- Uchio, Y.; Ochi, M.; Fujihara, A.; Adachi, N.; Iwasa, J.; Sakai, Y. Cryotherapy influences joint laxity and position sense of the healthy knee joint. Arch. Phys. Med. Rehabil. 2003, 84, 131–135. [Google Scholar] [CrossRef]
- Sierpina, V.S.; Frenkel, M.A. Acupuncture: A clinical review. South Med. J. 2005, 98, 330–337. [Google Scholar] [CrossRef] [Green Version]
- Cameron, D.M.; Bohannon, R.W.; Owen, S.V. Influence of hip position on measurements of the straight leg raise test. J. Orthop. Sports Phys. Ther. 1994, 19, 168–172. [Google Scholar] [CrossRef] [Green Version]
- Harvey, D. Assessment of the flexibility of elite athletes using the modified Thomas test. Br. J. Sports Med. 1998, 32, 68–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacPherson, H.; Altman, D.G.; Hammerschlag, R.; Youping, L.; Taixiang, W.; White, A.; Moher, D. Revised Standards for Reporting Interventions Evidence-based Clinical Chinese Medicine—Volume 3 in Clinical Trials of Acupuncture (STRICTA): Extending the CONSORT statement. J. Evid. Based Med. 2010, 3, 155. [Google Scholar] [CrossRef] [Green Version]
- Huffman, D.H.; Pietrosimone, B.G.; Grindstaff, T.L.; Hart, J.M.; Saliba, S.A.; Ingersoll, C.D. Effects of menthol-based counterirritant on quadriceps motoneuron-pool excitability. J. Sport Rehabil. 2010, 19, 30–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cha, W.S.; Oh, J.H.; Park, H.J.; Ahn, S.W.; Hong, S.Y.; Kim, N.I. Historical difference between traditional Korean medicine and traditional Chinese medicine. Neurol. Res. 2007, 29, 5–9. [Google Scholar] [CrossRef] [PubMed]
- Pietrosimone, B.G.; Hart, J.M.; Saliba, S.A.; Hertel, J.; Ingersoll, C.D. Immediate effects of transcutaneous electrical nerve stimulation and focal knee joint cooling on quadriceps activation. Med. Sci. Sports Exerc. 2009, 41, 1175. [Google Scholar] [CrossRef] [PubMed]
- Karner, M.; Brazkiewicz, F.; Remppis, A.; Fischer, J.; Gerlach, O.; Stremmel, W.; Subramanian, S.V.; Greten, H.J. Objectifying specific and nonspecific effects of acupuncture: A double-blinded randomised trial in osteoarthritis of the knee. Evid. Based Complement. Altern. Med. 2013, 2013, 427265. [Google Scholar] [CrossRef]
- De la Pena, E.; Sala, S.; Rovira, J.C.; Schmidt, R.F.; Belmonte, C. Elastoviscous substances with analgesic effects on joint pain reduce stretch-activated ion channel activity in vitro. Pain 2002, 99, 501–508. [Google Scholar] [CrossRef]
- Coutaux, A. Non-pharmacological treatments for pain relief: TENS and acupuncture. Jt. Bone Spine 2017, 84, 657–661. [Google Scholar] [CrossRef] [PubMed]
- Chu, J. The local mechanism of acupuncture. Zhonghua Yi Xue Za Zhi 2002, 65, 299–302. [Google Scholar]
- Sandberg, M.; Lundeberg, T.; Lindberg, L.G.; Gerdle, B. Effects of acupuncture on skin and muscle blood flow in healthy subjects. Eur. J. Aappl. Physiol. 2003, 90, 114–119. [Google Scholar] [CrossRef]
- Cagnie, B.; Dewitte, V.; Barbe, T.; Timmermans, F.; Delrue, N.; Meeus, M. Physiologic effects of dry needling. Curr. Pain Headache Rep. 2013, 17, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Langevin, H.M.; Churchill, D.L.; Cipolla, M.J. Mechanical signaling through connective tissue: A mechanism for the therapeutic effect of acupuncture. FASEB J. 2001, 15, 2275–2282. [Google Scholar] [CrossRef] [PubMed]
- Li, N.C.; Li, M.Y.; Chen, B.; Guo, Y. A new perspective of acupuncture: The interaction among three networks leads to neutralization. Evid. Based Complement. Alternat. Med. 2019, 2019, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Costa, L.A.; de Araujo, J.E. The immediate effects of local and adjacent acupuncture on the tibialis anterior muscle: A human study. Chin. Med. 2008, 3, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, L.P.; Zhou, S.; Lu, Z.; Tian, Q.; Li, X.; Cao, L.J.; Yu, J.H.; Wang, H. Bilateral effect of unilateral electroacupuncture on muscle strength. J. Altern. Complement. Med. 2007, 13, 539–546. [Google Scholar] [CrossRef] [Green Version]
- Park, J.; Ty Hopkins, J. Immediate effects of acupuncture and cryotherapy on quadriceps motoneuron pool excitability: Randomised trial using anterior knee infusion model. Acupunct. Med. 2012, 30, 195–202. [Google Scholar] [CrossRef]
- Giordano, J. The neurobiology of nociceptive and anti-nociceptive systems. Pain Physician 2005, 8, 277–290. [Google Scholar]
- Guo, J.T.; Dai, Q.P.; Qiu, M.L.; Chen, Y.Q. Clinical observation on the influence of electroacupuncture on the proprioception of patients with osteoarthritis. Chin. J. Rehabil. Med. 2008, 23, 1114–1116. [Google Scholar]
- Zhu, Y.; Qiu, M.; Ding, Y.; Qiang, Y.; Qin, B.Y. Effects of electroacupuncture on the proprioception of athletes with functional ankle instability. Zhongquo Zhen Jiu 2012, 32, 503–506. [Google Scholar] [CrossRef]
- Goddard, G.; Karibe, H.; McNeill, C.; Villafuerte, E. Acupuncture and sham acupuncture reduce muscle pain in myofascial pain patients. J. Orofac. Pain 2002, 16, 71–76. [Google Scholar] [PubMed]
- Assefi, N.P.; Sherman, K.J.; Jacobsen, C.; Goldberg, J.; Smith, W.R.; Buchwald, D. A randomized clinical trial of acupuncture compared with sham acupuncture in fibromyalgia. Ann. Intern. Med. 2005, 143, 10–19. [Google Scholar] [CrossRef]
- Chen, H.; Yang, M.; Ning, Z.; Lam, W.L.; Zhao, Y.K.; Yeung, W.F.; Ng, B.F.; Ziea, E.T.; Lao, L. A guideline for randomized controlled trials of acupuncture. Am. J. Chin. Med. 2019, 47, 1–18. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Acupoint Options & Participants Number | Acupoints (# of Needles) | Targeted Muscles | Anatomy Trains (Meridian) |
|---|---|---|---|
| A (Control: 1; Electro: 2, Manual: 1) | SP9, SP10, and SP11 (3) | SP9 (popliteus and soleus), SP10 (vastus medius), and SP11 (adductor longus, magnus) | Deep front line (Spleen meridian) |
| B (Control: 0; Electro: 1, Manual: 0) | ST31, ST34, and ST36 (3) | ST31 (rectus femoris), ST34 (vastus lateralis), and ST36 (tibialis anterior and extensor digitorum longus) | Superficial front line (Stomach meridian) |
| C (Control: 2; Electro: 4, Manual: 0) | GB30, GB31, and GB34 (3) | GB30 (piriformis, gluteus medius, and gluteus minimus), GB31 (iliotibial band and vastus lateralis), and GB34 (peroneus longus and extensor digitorum longus) | Lateral line (Gallbladder meridian) |
| A + B (Control: 3; Electro: 1, Manual: 1) | SP9, SP10, SP11, ST31, ST34, and ST36 (6) | SP9 (popliteus and soleus), SP10 (vastus medius), SP11 (adductor longus, magnus), ST31 (rectus femoris), ST34 (vastus lateralis), and ST36 (tibialis anterior and extensor digitorum longus) | Deep front line (Spleen meridian) and Superficial front line (Stomach meridian) |
| A + C (Control: 3; Electro: 6, Manual: 5) | SP9, SP10, SP11, GB30, GB31, and GB34 (6) | SP9 (popliteus and soleus), SP10 (vastus medius), SP 11 (adductor longus, magnus), GB30 (piriformis, gluteus medius, and gluteus minimus), GB31 (iliotibial band and vastus lateralis), and GB34 (peroneus longus and extensor digitorum longus) | Deep front line (Spleen meridian) and Lateral line (Gallbladder meridian) |
| B + C (Control: 1; Electro: 1, Manual: 1) | ST31, ST34, ST36, GB30, GB31, and GB34 (6) | ST31 (rectus femoris), ST34 (vastus lateralis), ST36 (tibialis anterior and extensor digitorum longus), GB30 (piriformis, gluteus medius, and gluteus minimus), GB31 (iliotibial band and vastus lateralis), and GB34 (peroneus longus and extensor digitorum longus) | Superficial front line (Stomach meridian) and Lateral line (Gallbladder meridian) |
| A + B+C (Control: 3; Electro: 3, Manual: 6) | SP9, SP10, SP11, ST31, ST34, ST36, GB30, GB31, and GB34 (9) | SP9 (popliteus and soleus), SP10 (vastus medius), SP11 (adductor longus, magnus), ST31 (rectus femoris), ST34 (vastus lateralis), ST36 (tibialis anterior and extensor digitorum longus), GB30 (piriformis, gluteus medius, and gluteus minimus), GB31 (iliotibial band and vastus lateralis), and GB34 (peroneus longus and extensor digitorum longus) | Deep front line (Spleen meridian), Superficial front line (Stomach meridian), and Lateral line (Gallbladder meridian) |
| Total (Control: 13; Electroacupuncture: 18; Manual acupuncture: 14) | |||
| Item | Detail |
|---|---|
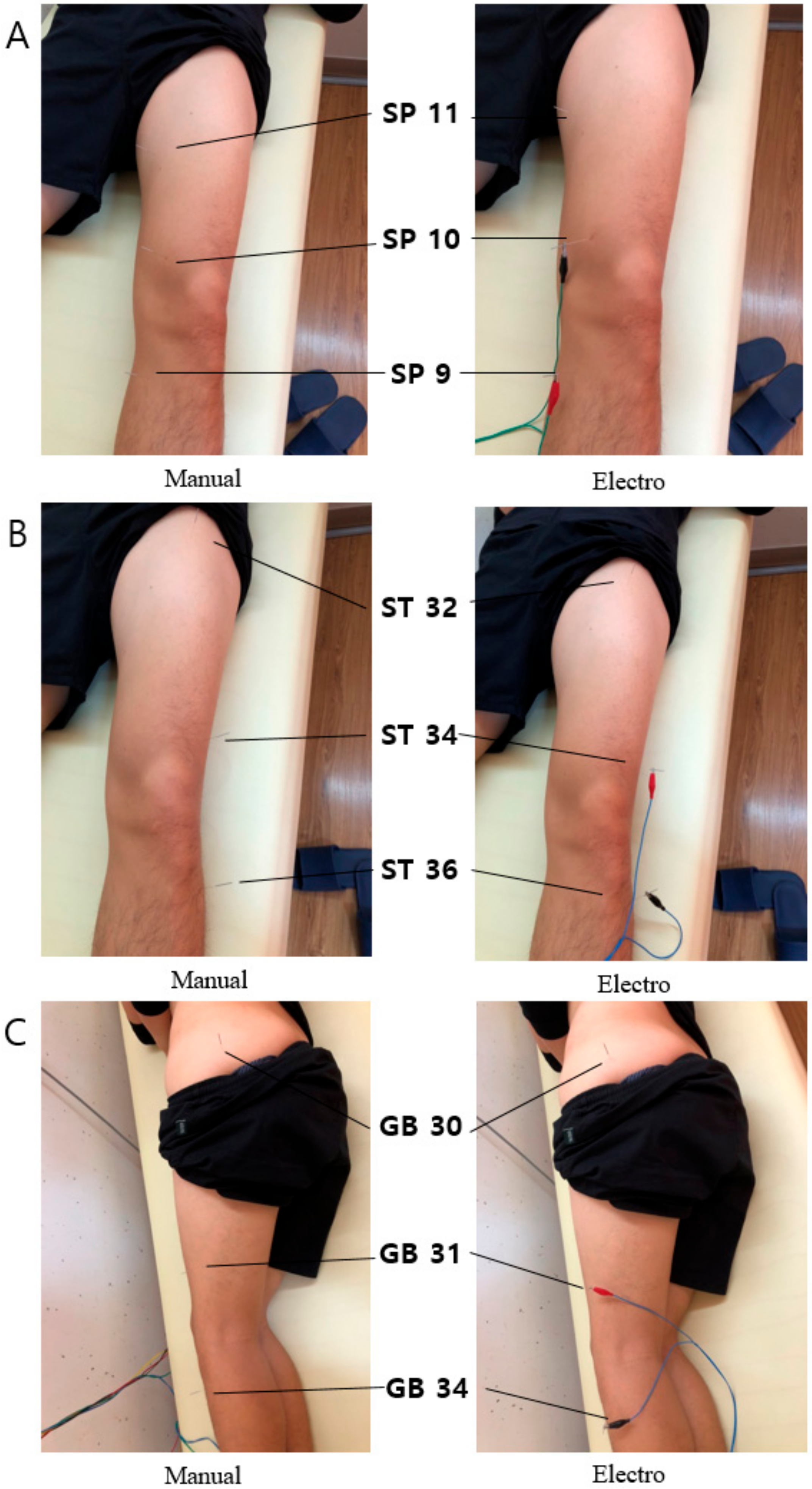
| 1. Acupuncture rationale | (1a) Style of acupuncture: We selected the acupoints based on traditional Korean medicine (TKM) meridian theory [27] to improve the hip joint ROM and hip flexor tightness, and to treat gluteus medius weakness. (1b) Reasoning for treatment provided, based on physical examination: Acupoints were chosen for individual participants by physical examination (straight leg raise test, modified Thomas test, gluteal medius manual muscle test). |
| 2. Details of needling | (2a) Number of needle inserts per subject: Three acupoints were inserted in case of positive in one physical examination. (2b) Names of points used (unilateral): Acupoints used were unilateral SP9, SP10 and SP11 points in case of positive in straight leg raise test (less than the normal ROM 70°), ST31, ST34, and ST36 points in case of positive in modified Thomas test, GB30, GB31, and GB34 points in case of positive in gluteal medius manual muscle test. (2c) Depth of insertion, based on a specified unit of measurement, or on a particular tissue level: In acupuncture treatment, the depth of needle insertion was about 5–30 mm. (2d) Manual acupuncture: It was performed for 15 min, the needle was rotated in either clockwise or counterclockwise direction to make the participant feel a de qi sensation. (2e) Electroacupuncture: It was performed for 15 min and electrically stimulation for 480 s (170 Hz, phase duration 55 μs within tolerable strength) using electro-stimulator (STN-110; StraTek Inc. Anyang, Korea). (2f) Needle type: The needles used for acupuncture were disposable stainless-steel needles (0.30 × 40 mm; Dong Bang Acupuncture., Seongnam, Korea). |
| 3. Treatment regimen | (3a) Electroacupoints: Three acupoints were inserted in case of positive in one physical examination, two acupoints were stimulated just below and above the knee joint (SP9-SP10, ST34-ST36, and GB31-GB34). (3b) Electroacupuncture stimulation: It was delivered at an intensity that the participant could notice but felt comfortable with. |
| 4. Practitioner background | (4a) Description of participating acupuncturist (qualification or professional affiliation, years in acupuncture practice, other relevant experience): Korean medical doctor administered the acupuncture treatment. He obtained license of traditional Korean Medicine and had used acupuncture in his practices for 13 years. |
| 5. Control or comparator interventions | (5a) Precise description of the control group: There is no sham acupuncture in control group, subjects were in supine position for 15 min. |
| Unit: ° | Control | Electroacupuncture | Manual Acupuncture |
|---|---|---|---|
| Baseline | 67.4 (4.1) | 68.0 (4.5) | 62.1 (2.7) |
| 0-min | 68.6 (4.1) | 71.9 (4.6) * | 67.3 (3.3) * |
| 20-min | 67.8 (3.7) | 72.9 (4.1) * | 67.6 (3.4) * |
| 40-min | 68.1 (3.7) | 72.4 (4.6) * | 67.5 (3.0) * |
| Replications at 15° | Replications at 45° | |||||
|---|---|---|---|---|---|---|
| Control | Electroacupuncture | Manual Acupuncture | Control | Electroacupuncture | Manual Acupuncture | |
| Baseline | 31.2 (4.2) | 13.0 (2.7) | 12.8 (3.7) | 8.4 (2.1) | 6.6 (1.9) | 8.5 (3.0) |
| 0-min | 12.2 (3.8) | 8.4 (2.0) | 12.5 (3.5) | 7.6 (2.2) | 6.7 (1.8) | 7.6 (3.2) |
| 20-min | 13.3 (4.7) | 9.6 (2.3) | 11.7 (3.1) | 6.2 (2.3) | 6.5 (1.2) | 6.2 (1.3) |
| 40-min | 13.6 (4.4) | 8.7 (2.0) | 12.0 (3.9) | 7.0 (2.6) | 6.7 (1.6) | 7.0 (2.1) |
| Strength (N·m/kg) | Activation (Central Activation Ratio) | |||||
|---|---|---|---|---|---|---|
| Control | Electroacupuncture | Manual Acupuncture | Control | Electroacupuncture | Manual Acupuncture | |
| Baseline | 3.9 (0.4) | 3.7 (0.3) | 3.4 (0.3) | 0.95 (0.02) | 0.95 (0.02) | 0.97 (0.01) |
| 0-min | 3.7 (0.4) | 3.4 †(0.3) | 3.3 (0.3) | 0.95 (0.02) | 0.95 (0.02) | 0.96 (0.02) |
| 20-min | 3.7 (0.5) | 3.5 (0.5) | 3.3 (0.3) | 0.94 (0.02) | 0.95 (0.02) | 0.96 (0.02) |
| 40-min | 3.6 (0.5) | 3.5 ‡ (0.5) | 3.1 § (0.3) | 0.94 (0.02) | 0.95 (0.02) | 0.96 (0.01) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, D.; Jang, S.; Park, J. Electroacupuncture and Manual Acupuncture Increase Joint Flexibility but Reduce Muscle Strength. Healthcare 2020, 8, 414. https://doi.org/10.3390/healthcare8040414
Kim D, Jang S, Park J. Electroacupuncture and Manual Acupuncture Increase Joint Flexibility but Reduce Muscle Strength. Healthcare. 2020; 8(4):414. https://doi.org/10.3390/healthcare8040414
Chicago/Turabian StyleKim, Daeho, Sein Jang, and Jihong Park. 2020. "Electroacupuncture and Manual Acupuncture Increase Joint Flexibility but Reduce Muscle Strength" Healthcare 8, no. 4: 414. https://doi.org/10.3390/healthcare8040414