Sleep Deprivation from the Perspective of a Patient Hospitalized in the Intensive Care Unit—Qualitative Study

 , , and
, , and
Abstract
:1. Introduction
Background
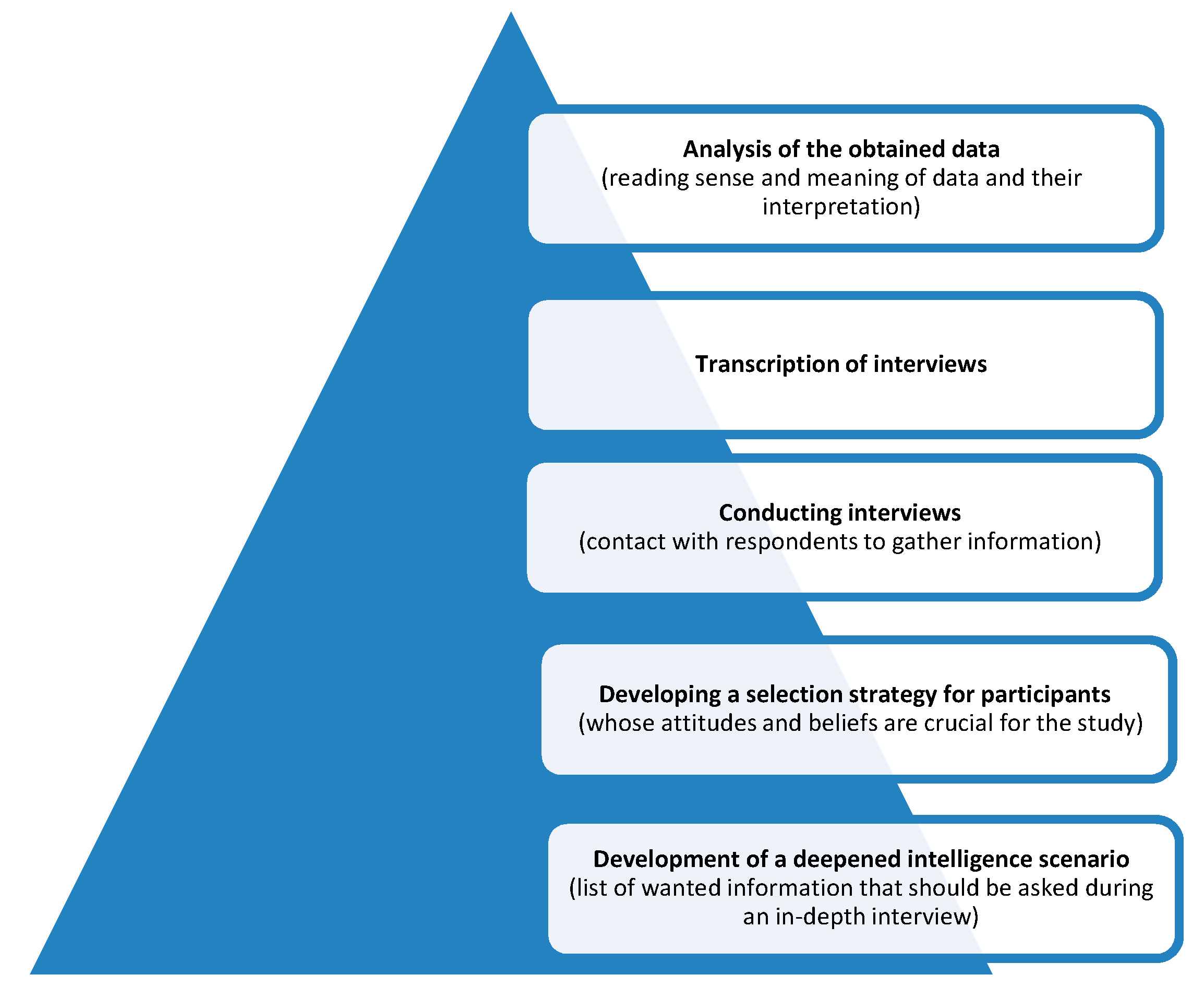
2. Methods
2.1. Sample and Recruitment
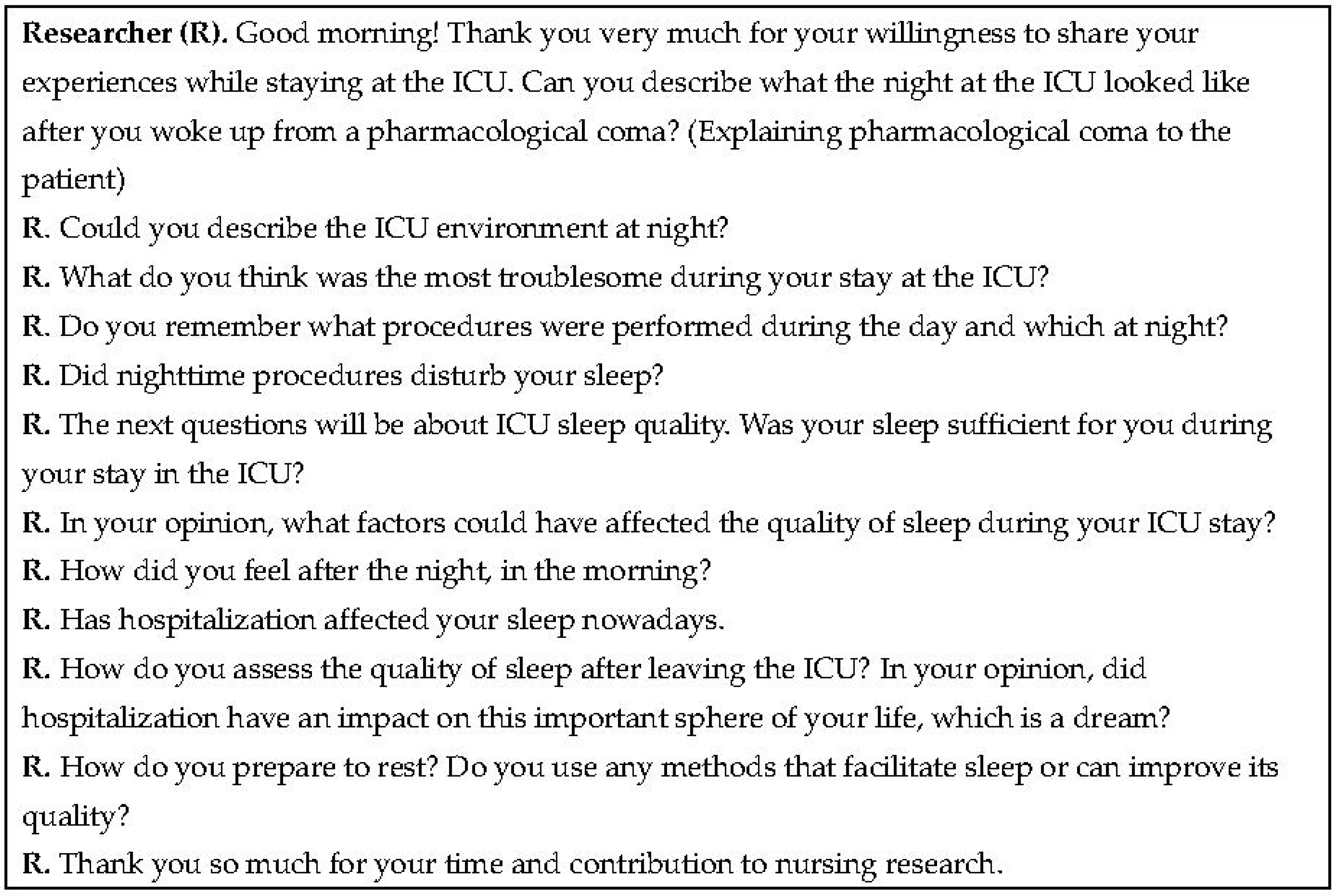
2.2. Questionnaire Development
2.3. Data Collection
2.4. Data Analysis
3. Results
3.1. Anxiety
“Stress wasn’t as much of a nuisance as the anger and fear that I might not return to my full former condition. This also had a huge impact on my sleep, because deep down I kept thinking that things would never be the same again, and such thoughts came to me when I was asleep.”(P1)
“There was one time when I was woken up from my coma, and I had that feeling of suffocation and I found it hard to sleep. I was afraid to fall asleep for fear that I wouldn’t wake up again. I panicked… I had to be given oxygen although I didn’t really need it.”(P2)
“I don’t know if the fear of surgery was worse or anxiety or if everything is good when I woke up after the surgery. I had this endotracheal tube and I couldn’t ask anyone. After a while, the nurse said that she was already after the surgery, but I did not know this place and these people. Maybe if I had seen this room before, it would have been better for me.”(P9)
“After waking up, I couldn’t bear to lie down. I felt thirsty, I wanted to roll on the bed, but no one understood what I was saying. Night? I thought it lasted forever. All in all, it was only during the visit that I saw the watch and I knew it was morning. There all the time I was unsure what time it is.”(P8)
3.2. Noise
“Noise did nothing but disturb; those loud conversations between nurses, stamping, pushing things. (…) I don’t think that made it easier for me to fall asleep, but made it all the more difficult. (….) And there were those situations when at five o’clock in the morning (although they wake patients up probably at 8 for the morning hygiene routines) the nurse would give me my medications, but two or three of them would get together by the isolation room and they would talk by my bed, wake me up and so on; this was what would wake me up—their conversations.”(P1)
“The worst thing about staying at the ICU was that you never know what noise will wake you up. Sometimes it was so that for 3 h it was quite quiet, and immediately began to turn on the pumps, you could hear metal baskets. Sometimes you sleep there an hour, sometimes 10 min and sometimes not at all. You never know what the night will bring.”(P8)
3.3. Light
“The exhausting light: natural light during the day, and artificial light at night. At some point I asked my family for sunglasses (…) so when I could sleep during the day because there was only slight noise in the background but I was disturbed by the light, I would lie wearing them and fall asleep. The nurses laughed at me, but they always helped me to put them on, because my paralysis stopped me from doing so.”(P4)
“During the evening, nurses tried especially to dim the light in the room but all of a sudden, at 8:00 p.m., there was a round and they turned all the lights on in the room as they had to read all the records. I felt dizzy as though I’d been woken by a brutal force. And it was always like that whenever they intervened during the night; when something was going on with other patients, they always turned the light on in the entire room. It was awful.”(P1)
3.4. Medical Staff
“I felt like I was the bed number. Everyone was saying to each other, Have you looked at seven? There was a pump to change. But when the nurses came to bed I felt like I was finally getting my name back. Then I felt safe and important at the same time. I could fall asleep safely.”(P18)
“Well… what was most annoying for me was when nurses or doctors intervened with other patients who were around me; I always automatically woke up when something was going on in my room.”(P19)
“There was a patient next to me who had to have cardioversion several times during the night, and all that commotion was stressful for me, so I obviously couldn’t sleep either.”(P3)
3.5. There’s No Place like Home
“Then I remember that the nurse answered my daughter’s phone and said I was still asleep and I had a respirator. And I wanted to say everything was OK, but I couldn’t. Then I was worried all the time if my family knew I was doing well.”(P10)
“(…) I didn’t feel regenerated at all, I felt more exhausted each day. I had no appetite, my meals were irregular, I felt like I was on medication all the time and I didn’t feel regenerated even after a night’s sleep. Regardless of whether I slept during the night or not, I didn’t feel regenerated.”(P1)
“I didn’t have nightmares to do with the ICU or the accident. When I returned home, I slept very well to regenerate.”(P3)
“I already sleep well—I sleep poorly when I feel pain in my leg stub—after an active day.”(P4)
“(…) It seems to me that it’s a question of every patient requiring different things individually. I think that when one patient needs peace, another will sleep well.”(P5)
4. Discussion
5. Conclusions
6. Implications for Nursing and Health Policy
7. Limitations
Author Contributions
Funding
Conflicts of Interest
Ethical Approval
References
- Matthews, E.E. Sleep Disturbances and Fatigue in Critically ILL Patients. AACN Adv. Crit. Care 2011, 22, 204–224. [Google Scholar] [CrossRef] [PubMed]
- Kowalska, A. Mózg, a Sen. In Neurokogintywistyka w Patol. i Zdrowiu, 2011–2013; Pomorski Uniwersytet Medyczny w Szczexinie: Szczecin, Poland, 2013; pp. 80–83. [Google Scholar]
- Kawalec, A.; Pawlas, K. Enviromental factors affecting sleep and respecting sleep hygiene. Probl. Hig. Epidemiol. 2013, 94, 1–5. [Google Scholar]
- Sterniczuk, R.; Rusak, B.; Rockwood, K. Sleep Disturbance in Older ICU Patients. Clin. Interv. Aging 2014, 9, 969–977. [Google Scholar] [CrossRef] [Green Version]
- Kamdar, B.B.; Needham, D.M.; Collop, N.A. Sleep Deprivation in Critical Illness: Its Role in Physical and Psychological Recovery. J. Intensive Care Med. 2012, 27, 97–111. [Google Scholar] [CrossRef]
- Bonnet, M.; Kryger, M.; Roth, T.; Dement, W. Acute Sleep Deprivation. In Principles and Practice of Sleep Medicine, 5th ed.; Elsevier Saunders: St. Louis, MO, USA, 2011; pp. 54–66. [Google Scholar]
- Hellström, A.; Willman, A. Promoting Sleep by Nursing Interventions in Health Care Settings: A Systematic Review. Worldviews Evid. Based Nurs. 2011, 8, 128–142. [Google Scholar] [CrossRef] [PubMed]
- Beltrami, F.G.; Nguyen, X.-L.; Pichereau, C.; Maury, E.; Fleury, B.; Fagondes, S. Sleep in the Intensive Care Unit. J. Bras. Pneumol. 2015, 41, 539–546. [Google Scholar] [CrossRef] [PubMed]
- Kamdar, B.B.; Martin, J.L.; Needham, D.M.; Ong, M.K. Promoting Sleep to Improve Delirium in the ICU. Crit. Care Med. 2016, 44, 2290–2291. [Google Scholar] [CrossRef] [Green Version]
- Freedman, N.S.; Kotzer, N.; Schwab, R.J. Patient Perception of Sleep Quality and Etiology of Sleep Disruption in the Intensive Care Unit. Am. J. Respir. Crit. Care Med. 1999, 159, 1155–1162. [Google Scholar] [CrossRef]
- Elliott, R.; McKinley, S.; Cistulli, P.; Fien, M. Characterisation of Sleep in Intensive Care Using 24-hour Polysomnography: An Observational Study. Crit. Care 2013, 17, 46. [Google Scholar] [CrossRef] [Green Version]
- Broughton, R.; Baron, R. Sleep Patterns in the Intensive Care Unit and on the Ward after Acute Myocardial Infarction. Electroencephalogr. Clin. Neurophysiol. 1978, 45, 348–360. [Google Scholar] [CrossRef]
- Nelson, J.E.; Meier, D.E.; Oei, E.J.; Nierman, D.M.; Senzel, R.S.; Manfredi, P.L.; Davis, S.M.; Morrison, R.S. Self-Reported Symptom Experience of Critically Ill Cancer Patients Receiving Intensive Care. Crit. Care Med. 2001, 29, 277–282. [Google Scholar] [CrossRef] [PubMed]
- Simini, B. Patients’ Perceptions of Intensive Care. Lancet 1999, 354, 571–572. [Google Scholar] [CrossRef]
- Nicolás, A.; Aizpitarte, E.; Iruarrizaga, A.; Vázquez, M.; Margall, A.; Asiain, C. Perception of Night-Time Sleep by Surgical Patients in an Intensive Care Unit. Nurs. Crit. Care 2008, 13, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Van Der Zalm, J.E.; Bergum, V. Hermeneutic-Phenomenology: Providing Living Knowledge for Nursing Practice. J. Adv. Nurs. 2000. [Google Scholar] [CrossRef]
- Pietkiewicz, I.; Smith, J.A. A practical guide to using Interpretative Phenomenological Analysis in qualitative research psychology. Psychol. J. 2014, 20, 7–14. [Google Scholar] [CrossRef]
- Dahlberg, K.; Drew, N. A Lifeworld Paradigm for Nursing Research. J. Holist. Nurs. 1997, 15, 303–317. [Google Scholar] [CrossRef]
- van Manen, M. Researching Lived Experience: Human Science for an Action Sensitive Pedagogy; SUNY: New York, NY, USA, 1990; pp. 89–93. [Google Scholar]
- Tembo, A.C.; Parker, V.; Higgins, I. The Experience of Sleep Deprivation in Intensive Care Patients: Findings from a Larger Hermeneutic Phenomenological Study. Intensive Crit. Care Nurs. 2013, 29, 310–316. [Google Scholar] [CrossRef] [PubMed]
- Bihari, S.; Doug McEvoy, R.; Matheson, E.; Kim, S.; Woodman, R.J.; Bersten, A.D. Factors Affecting Sleep Quality of Patients in Intensive Care Unit. J. Clin. Sleep Med. 2012, 8, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Telias, I.; Wilcox, M.E. Sleep and Circadian Rhythm in Critical Illness. Crit. Care 2019, 23, 83. [Google Scholar] [CrossRef] [Green Version]
- Stewart, J.A.; Green, C.; Stewart, J.; Tiruvoipati, R. Factors Influencing Quality of Sleep among Non-Mechanically Ventilated Patients in the Intensive Care Unit. Aust. Crit. Care 2017. [Google Scholar] [CrossRef]
- Ehlers, V.J.; Watson, H.; Moleki, M.M. Factors Contributing to Sleep Deprivation in a Multidisciplinary Intensive Care Unit in South Africa. Curationis 2013, 36, 8. [Google Scholar] [CrossRef] [PubMed]
- McKinley, S.; Aitken, L.M.; Alison, J.A.; King, M.; Leslie, G.; Burmeister, E.; Elliott, D. Sleep and other Factors Associated with Mental Health and Psychological Distress after Intensive Care for Critical Illness. Intensive Care Med. 2012, 38, 627–633. [Google Scholar] [CrossRef] [PubMed]
- Devlin, J.W.; Skrobik, Y.; Gélinas, C.; Needham, D.M.; Slooter, A.J.C.; Pandharipande, P.P.; Watson, P.L.; Weinhouse, G.L.; Nunnally, M.E.; Rochwerg, B.; et al. Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU. Crit. Care Med. 2018, 46, e825–e873. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| No. Patient | Age | Sex | The Reason for Hospitalization | Time of Stay in ICU (Days) | Has the Patient Had Tracheostomy | Was the Patient in the General/Isolated Room |
|---|---|---|---|---|---|---|
| P1 | 23 | Male | multifocal injury | 14 | no | general room |
| P2 | 36 | Female | multifocal injury, transport accident | 88 | yes | isolated room |
| P3 | 28 | Female | multifocal injury, transport accident | 28 | yes | general room |
| P4 | 33 | Male | multifocal injury | 56 | yes | isolated room |
| P5 | 34 | Male | cervical spine injury | 32 | yes | general room |
| P6 | 42 | Male | cardiac surgery—by pass | 12 | no | general room |
| P7 | 55 | Female | cardiac surgery—aortic dissection | 45 | yes | isolated room |
| P8 | 61 | Male | cardiac surgery—aortic valve plastic surgery | 16 | no | general room |
| P9 | 47 | Female | cardiac surgery—aortic valve plastic surgery | 14 | no | general room |
| P10 | 49 | Female | cardiac surgery—aortic dissection | 18 | no | general room |
| P11 | 27 | Male | cardiac surgery—aortic valve plastic surgery | 7 | no | general room |
| P12 | 39 | Male | cardiac surgery—mitral valve replacement | 9 | no | general room |
| P13 | 53 | Male | cardiac surgery—aortic dissection | 7 | Yes | general room |
| P14 | 46 | Female | cardiac surgery—by pass | 42 | yes | isolated room |
| P15 | 50 | Male | cardiac surgery—aortic dissection | 75 | yes | isolated room |
| P16 | 74 | Male | respiratory failure | 112 | no | general room |
| P17 | 90 | male | respiratory failure | 7 | no | general room |
| P18 | 71 | female | respiratory failure | 126 | yes | isolated room |
| P19 | 78 | Male | cardiac surgery—aortic dissection | 21 | no | general room |
| P20 | 89 | female | respiratory failure | 7 | no | general room |
| P21 | 29 | Male | multifocal injury | 21 | no | isolated room |
| P22 | 32 | male | cervical spine injury | 14 | no | general room |
| P23 | 58 | male | multifocal injury | 18 | no | general room |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lewandowska, K.; Mędrzycka-Dąbrowska, W.; Pilch, D.; Wach, K.; Fortunato, A.; Krupa, S.; Ozga, D. Sleep Deprivation from the Perspective of a Patient Hospitalized in the Intensive Care Unit—Qualitative Study. Healthcare 2020, 8, 351. https://doi.org/10.3390/healthcare8030351
Lewandowska K, Mędrzycka-Dąbrowska W, Pilch D, Wach K, Fortunato A, Krupa S, Ozga D. Sleep Deprivation from the Perspective of a Patient Hospitalized in the Intensive Care Unit—Qualitative Study. Healthcare. 2020; 8(3):351. https://doi.org/10.3390/healthcare8030351
Chicago/Turabian StyleLewandowska, Katarzyna, Wioletta Mędrzycka-Dąbrowska, Dorota Pilch, Krystyna Wach, Antonietta Fortunato, Sabina Krupa, and Dorota Ozga. 2020. "Sleep Deprivation from the Perspective of a Patient Hospitalized in the Intensive Care Unit—Qualitative Study" Healthcare 8, no. 3: 351. https://doi.org/10.3390/healthcare8030351