Virtual Reality-Based Cognitive–Motor Rehabilitation in Older Adults with Mild Cognitive Impairment: A Randomized Controlled Study on Motivation and Cognitive Function



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Ethics
2.3. Sample Size Estimation
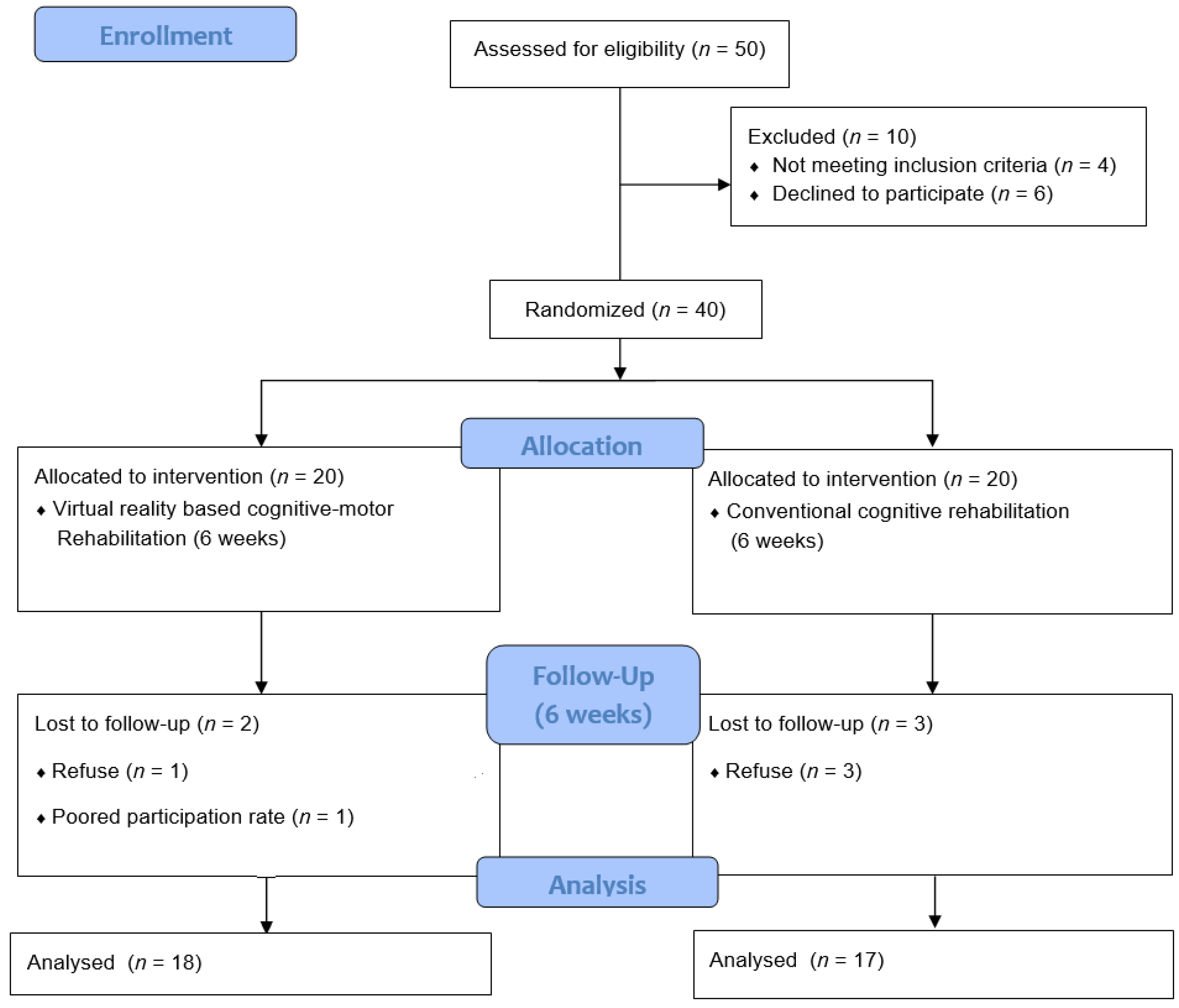
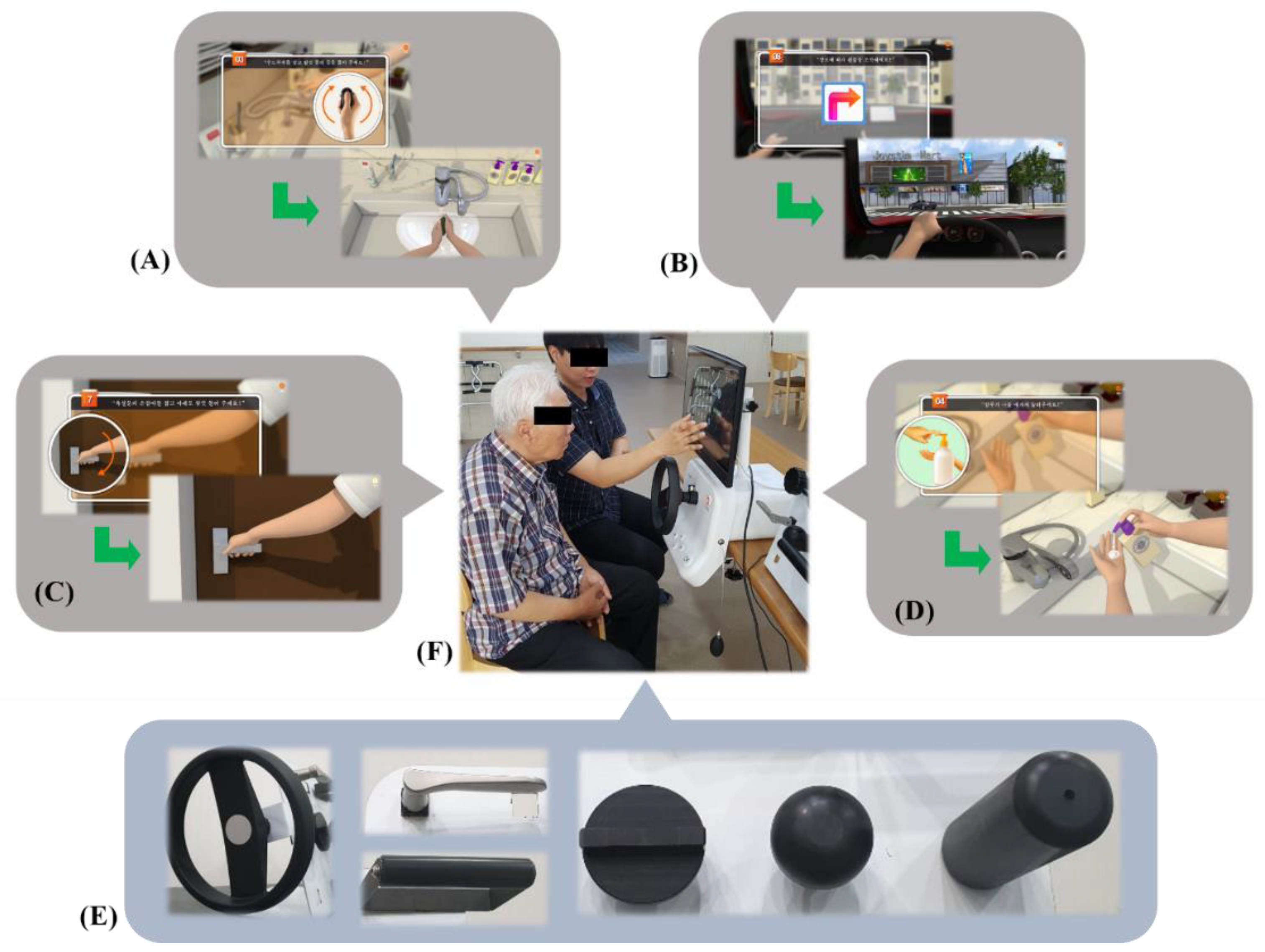
2.4. Study Design and Procedures
2.5. Outcome Measurement
2.6. Statistical Analysis
3. Results
3.1. Subjects’ Characteristics
3.2. Cognitive Function Evaluation
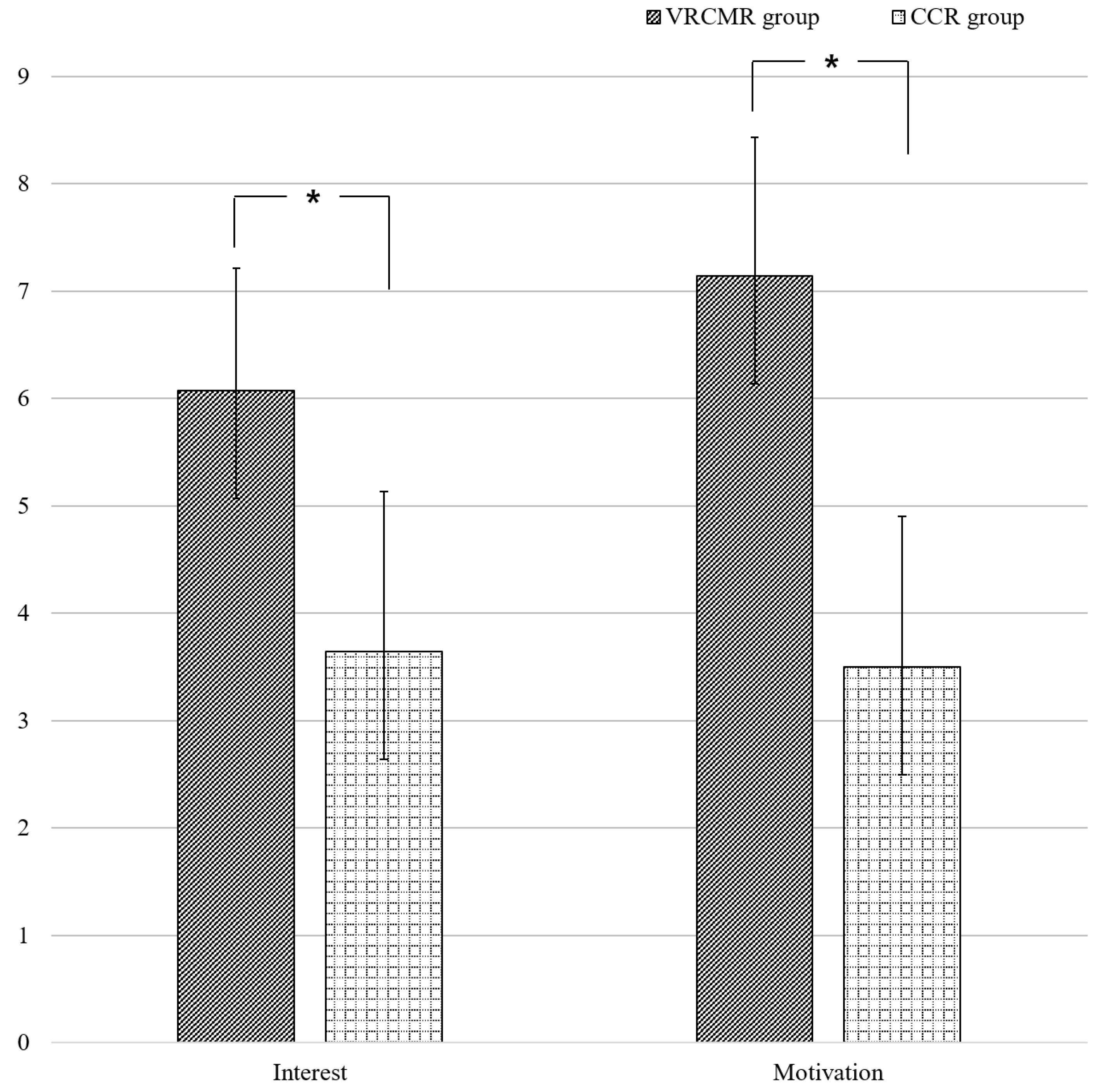
3.3. Interest and Motivation Evaluation Using NRSS
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Livingston, G.; Sommerlad, A.; Orgeta, V.; Costafreda, S.G.; Huntley, J.; Ames, D.; Ballard, C.; Banerjee, S.; Burns, A.; Cohen-Mansfield, J.; et al. Dementia prevention, intervention, and care. Lancet 2017, 390, 2673–2734. [Google Scholar] [CrossRef] [Green Version]
- Luck, T.; Luppa, M.; Briel, S.; Riedel-Heller, S.G. Incidence of mild cognitive impairment: A systematic review. Dement. Geriatr. Cogn. Disord. 2010, 29, 164–175. [Google Scholar] [CrossRef]
- Bruscoli, M.; Lovestone, S.I. Is MCI really just early dementia? A systematic review of conversion studies. Int. Psychogeriatr. 2004, 16, 129–140. [Google Scholar] [CrossRef] [PubMed]
- Petersen, R.C.; Doody, R.; Kurz, A.; Mohs, R.C.; Morris, J.C.; Rabins, P.V.; Ritchie, K.; Rossor, M.; Thal, L.; Winblad, B. Current concepts in mild cognitive impairment. Arch. Neurol. 2001, 58, 1985–1992. [Google Scholar] [CrossRef]
- Johnson, D.K.; Storandt, M.; Morris, J.C.; Galvin, J.E. Longitudinal study of the transition from healthy aging to Alzheimer disease. Arch. Neurol. 2009, 66, 1254–1259. [Google Scholar] [CrossRef] [Green Version]
- Murman, D.L. The Impact of Age on Cognition. Semin. Hear. 2015, 36, 111–121. [Google Scholar] [CrossRef] [PubMed]
- Artero, S.; Ancelin, M.L.; Portet, F.; Dupuy, A.; Berr, C.; Dartigues, J.F.; Tzourio, C.; Rouaud, O.; Poncent, M.; Pasquier, F.; et al. Risk profiles for mild cognitive impairment and progression to dementia are gender specific. J. Neurol. Neurosurg. Psychiatry 2008, 79, 979–984. [Google Scholar] [CrossRef] [Green Version]
- Bahar-Fuchs, A.; Clare, L.; Woods, B. Cognitive training and cognitive rehabilitation for persons with mild to moderate dementia of the Alzheimer’s or vascular type: A review. Alzheimers Res. Ther. 2013, 5, 35. [Google Scholar] [CrossRef]
- Kueider, A.M.; Parisi, J.M.; Gross, A.L.; Rebok, G.W. Computerized cognitive training with older adults: A systematic review. PLoS ONE 2012, 7, 40588. [Google Scholar] [CrossRef] [Green Version]
- Fan, F.; Zou, Y.; Tan, Y.; Hong, L.E.; Tan, S. Computerized cognitive remediation therapy effects on resting state brain activity and cognition in schizophrenia. Sci. Rep. 2017, 6, 4758. [Google Scholar] [CrossRef]
- Bernini, S.; Alloni, A.; Panzarasa, S.; Picascia, M.; Quaglini, S.; Tassorelli, C.; Sinforiani, E. A computer-based cognitive training in Mild Cognitive Impairment in Parkinson’s Disease. NeuroRehabilitation 2019, 44, 555–567. [Google Scholar] [CrossRef] [PubMed]
- Lee, G.J.; Bang, H.J.; Lee, K.M.; Kong, H.H.; Seo, H.S.; Oh, M.; Bang, M. A comparison of the effects between 2 computerized cognitive training programs, Bettercog and COMCOG, on elderly patients with MCI and mild dementia: A single-blind randomized controlled study. Medicine 2018, 97, 13007. [Google Scholar] [CrossRef] [PubMed]
- Ten Brinke, L.F.; Best, J.R.; Chan, J.L.; Ghag, C.; Erickson, K.I.; Handy, T.C.; Liu-Ambrose, T. The Effects of Computerized Cognitive Training with and without Physical Exercise on Cognitive Function in Older Adults: An 8-week Randomized Controlled Trial. J. Gerontol. 2019, 75, 755–763. [Google Scholar] [CrossRef] [PubMed]
- Liao, Y.Y.; Tseng, H.Y.; Lin, Y.J.; Wang, C.J.; Hsu, W.C. Using virtual reality-based training to improve cognitive function, instrumental activities of daily living and neural efficiency in older adults with mild cognitive impairment: A randomized controlled trial. Eur. J. Phys. Rehabil. Med. 2019, 56, 47. [Google Scholar] [CrossRef]
- Zając-Lamparska, L.; Wiłkość-Dębczyńska, M.; Wojciechowski, A.; Podhorecka, M.; Polak-Szabela, A.; Warchoł, Ł.; Kedziora-Kornatowska, K.; Araszkiewicz, A.; Izedebski, P. Effects of virtual reality-based cognitive training in older adults living without and with mild dementia: A pretest-posttest design pilot study. BMC Res. Notes 2019, 12, 776. [Google Scholar] [CrossRef]
- Doniger, G.M.; Beeri, M.S.; Bahar-Fuchs, A.; Gottlieb, A.; Tkachov, A.; Kenan, H.; Livny, A.; Bahat, Y.; Sharon, H.; Ben-Gal, O.; et al. Virtual reality-based cognitive-motor training for middle-aged adults at high Alzheimer’s disease risk: A randomized controlled trial. Alzheimers Dement. 2018, 4, 118–129. [Google Scholar] [CrossRef]
- Park, J.H.; Liao, Y.; Kim, D.R.; Song, S.; Lim, J.H.; Park, H.; Lee, Y.; Park, K.W. Feasibility and Tolerability of a Culture-Based Virtual Reality (VR) Training Program in Patients with Mild Cognitive Impairment: A Randomized Controlled Pilot Study. Int. J. Environ. Res. Public Health 2020, 17, 3030. [Google Scholar] [CrossRef]
- Yang, S.; Chun, M.H.; Son, Y.R. Effect of virtual reality on cognitive dysfunction in patients with brain tumor. Ann. Rehabil. Med. 2014, 38, 726–733. [Google Scholar] [CrossRef] [Green Version]
- Subramanian, S.; Dahl, Y.; Skjæret Maroni, N.; Vereijken, B.; Svanæs, D. Assessing Motivational Differences Between Young and Older Adults When Playing an Exergame. Games Health J. 2020, 9, 24–30. [Google Scholar] [CrossRef]
- Amjad, I.; Toor, H.; Niazi, I.K.; Pervaiz, S.; Jochumsen, M.; Shafique, M.; Haavik, H.; Ahmed, T. Xbox 360 Kinect Cognitive Games Improve Slowness, Complexity of EEG, and Cognitive Functions in Subjects with Mild Cognitive Impairment: A Randomized Control Trial. Games Health J. 2019, 8, 144–152. [Google Scholar] [CrossRef]
- Lee, J.Y.; Lee, D.W.; Cho, S.J.; Na, D.L.; Jeon, H.J.; Kim, S.K.; Lee, Y.R.; Youn, J.H.; Kwon, M.; Lee, J.H.; et al. Brief screening for mild cognitive impairment in elderly outpatient clinic: Validation of the Korean version of the Montreal Cognitive Assessment. J. Geriatr. Psychiatry Neurol. 2008, 21, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Llinas-Regla, J.; Vilalta-Franch, J.; Lopez-Pousa, S.; Calvo-Perxas, L.; Torrents Rodas, D.; Garre-Olmo, J. The Trail Making Test. Assessment 2017, 24, 183–196. [Google Scholar] [CrossRef] [PubMed]
- Tamez, E.; Myerson, J.; Morris, L.; White, D.A.; Baum, C.; Connor, L.T. Assessing executive abilities following acute stroke with the trail making test and digit span. Behav. Neurol. 2011, 24, 177–185. [Google Scholar] [CrossRef]
- Kothari, M.; Svensson, P.; Jensen, J.; Holm, T.D.; Nielsen, M.S.; Mosegaard, T.; Nielsen, J.F.; Ghovanloo, M.; Baad-Hansen, L. Tongue-controlled computer game: A new approach for rehabilitation of tongue motor function. Arch. Phys. Med. Rehabil. 2014, 95, 524–530. [Google Scholar] [CrossRef]
- Fransson, P.A.; Patel, M.; Jensen, H.; Lundberg, M.; Tjernström, F.; Magnusson, M.; Ekvall Hansson, E. Postural instability in an immersive Virtual Reality adapts with repetition and includes directional and gender specific effects. Sci. Rep. 2019, 28, 3168. [Google Scholar] [CrossRef] [Green Version]
- Culpepper, L.; Lam, R.W.; McIntyre, R.S. Cognitive Impairment in Patients with Depression: Awareness, Assessment, and Management. J. Clin. Psychiatry 2017, 78, 1383–1394. [Google Scholar] [CrossRef]
- Kim, B.R.; Chun, M.H.; Kim, L.S.; Park, J.Y. Effect of virtual reality on cognition in stroke patients. Ann. Rehabil. Med. 2011, 35, 450–459. [Google Scholar] [CrossRef] [Green Version]
- Kim, M.Y.; Lee, K.S.; Choi, J.S.; Kim, H.B.; Park, C.I. Effectiveness of cognitive training based on virtual reality for the elderly. Ann. Rehabil. Med. 2005, 29, 424–433. [Google Scholar]
- Calabrò, R.S.; Russo, M.; Naro, A.; De Luca, R.; Leo, A.; Tomasello, P.; Molonia, F.; Dattola, V.; Bramanti, A.; Bramanti, P. Robotic gait training in multiple sclerosis rehabilitation: Can virtual reality make the difference? Findings from a randomized controlled trial. J. Neurol. Sci. 2017, 377, 25–30. [Google Scholar] [CrossRef] [PubMed]
- You, S.H.; Jang, S.H.; Kim, Y.H.; Hallett, M.; Ahn, S.H.; Kwon, Y.H.; Kim, J.H.; Lee, M.Y. Virtual reality-induced cortical reorganization and associated locomotor recovery in chronic stroke: An experimenter-blind randomized study. Stroke 2005, 36, 1166–1171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oh, Y.B.; Kim, G.W.; Han, K.S.; Won, Y.H.; Park, S.H.; Seo, J.H.; Ko, M.H. Efficacy of Virtual Reality Combined With Real Instrument Training for Patients With Stroke: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2019, 100, 1400–1408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mandolesi, L.; Polverino, A.; Montuori, S.; Foti, F.; Ferraioli, G.; Sorrentino, P.; Sorrentino, G. Effects of Physical Exercise on Cognitive Functioning and Wellbeing: Biological and Psychological Benefits. Front. Psychol. 2018, 9, 509. [Google Scholar] [CrossRef] [PubMed]
- Luger, A.; Deuster, P.A.; Kyle, S.B.; Gallucci, W.T.; Montgomery, L.C.; Gold, P.W.; Loriaux, D.L.; Chrousos, G.P. Acute hypothalamic-pituitary-adrenal responses to the stress of treadmill exercise. Physiologic adaptations to physical training. N. Engl. J. Med. 1987, 316, 1309–1315. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| VRCMR Group (n = 18) | CCR Group (n = 17) | |
|---|---|---|
| Number of subject | 18 | 17 |
| Gender (man/woman) | 10:8 | 7:10 |
| Age (year) | 75.8 ± 8.5 | 77.2 ± 7.2 |
| Educational level | ||
| Uneducated | 2 | 1 |
| Elementary school | 13 | 13 |
| Middle School | 2 | 2 |
| High school | 1 | 1 |
| University | 0 | 0 |
| VRCMR Group (n = 18) | CCR Group (n = 17) | Between Groups p-Values | |||||
|---|---|---|---|---|---|---|---|
| Before Intervention | After Intervention | p-Value | Before Intervention | After Intervention | p-Value | ||
| MoCA Trail Making Test | 17.7 ± 3.4 | 20.9 ± 3.4 | <0.001* | 17.8 ± 2.4 | 18.3 ± 3.0 | 0.047 * | 0.045 † |
| TMT—A | 72.2 ± 4.4 | 65.1 ± 4.4 | <0.001* | 69.6 ± 4.3 | 68.6 ± 4.6 | 0.079 | 0.039 † |
| TMT—B Digit Span Test | 152.3 ± 9.1 | 144.4 ± 7.7 | <0.001* | 154. ± 10.9 | 152.3 ± 11.2 | 0.060 | 0.040 † |
| DST—forward | 3.1 ± 0.8 | 4.7 ± 0.8 | <0.001* | 3.2 ± 0.8 | 3.7 ± 0.9 | 0.029 * | 0.011 † |
| DST—backward | 2.0 ± 0.7 | 2.6 ± 0.7 | <0.001* | 2.0 ± 0.5 | 2.4 ± 0.6 | 0.008 * | 0.424 |
| VRCMR Group | CCR Group | p-Value | Cohen’s d | |
|---|---|---|---|---|
| Δ Montreal Cognitive Assessment | 3.21 ± 0.89 | 0.50 ± 0.85 | <0.001 † | 0.8 |
| Trail Making Test | ||||
| Δ Trail Making Test-A | −7.14 ± 1.70 | −1.00 ± 1.96 | <0.001 † | 0.135 |
| Δ Trail Making Test–B | −7.93 ± 6.67 | −2.14 ± 3.90 | 0.009 † | 0.6 |
| Digit Span Test | ||||
| Δ Digit Span Test-forward | 1.57 ± 0.75 | 0.50 ± 0.76 | <0.001 † | 1.19 |
| Δ Digit Span Test-backward | 0.57 ± 0.51 | 0.43 ± 0.51 | 0.468 | 0.2 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, J.-S.; Jung, Y.-J.; Lee, G. Virtual Reality-Based Cognitive–Motor Rehabilitation in Older Adults with Mild Cognitive Impairment: A Randomized Controlled Study on Motivation and Cognitive Function. Healthcare 2020, 8, 335. https://doi.org/10.3390/healthcare8030335
Park J-S, Jung Y-J, Lee G. Virtual Reality-Based Cognitive–Motor Rehabilitation in Older Adults with Mild Cognitive Impairment: A Randomized Controlled Study on Motivation and Cognitive Function. Healthcare. 2020; 8(3):335. https://doi.org/10.3390/healthcare8030335
Chicago/Turabian StylePark, Ji-Su, Young-Jin Jung, and Gihyoun Lee. 2020. "Virtual Reality-Based Cognitive–Motor Rehabilitation in Older Adults with Mild Cognitive Impairment: A Randomized Controlled Study on Motivation and Cognitive Function" Healthcare 8, no. 3: 335. https://doi.org/10.3390/healthcare8030335