Maximum and Minimum Phonatory Glottal Area before and after Treatment for Vocal Nodules

 ,
,  ,
, 

Abstract
:1. Introduction
2. Methods
2.1. Patient Sources
2.2. Voice Analysis
2.3. Subjective Assessment
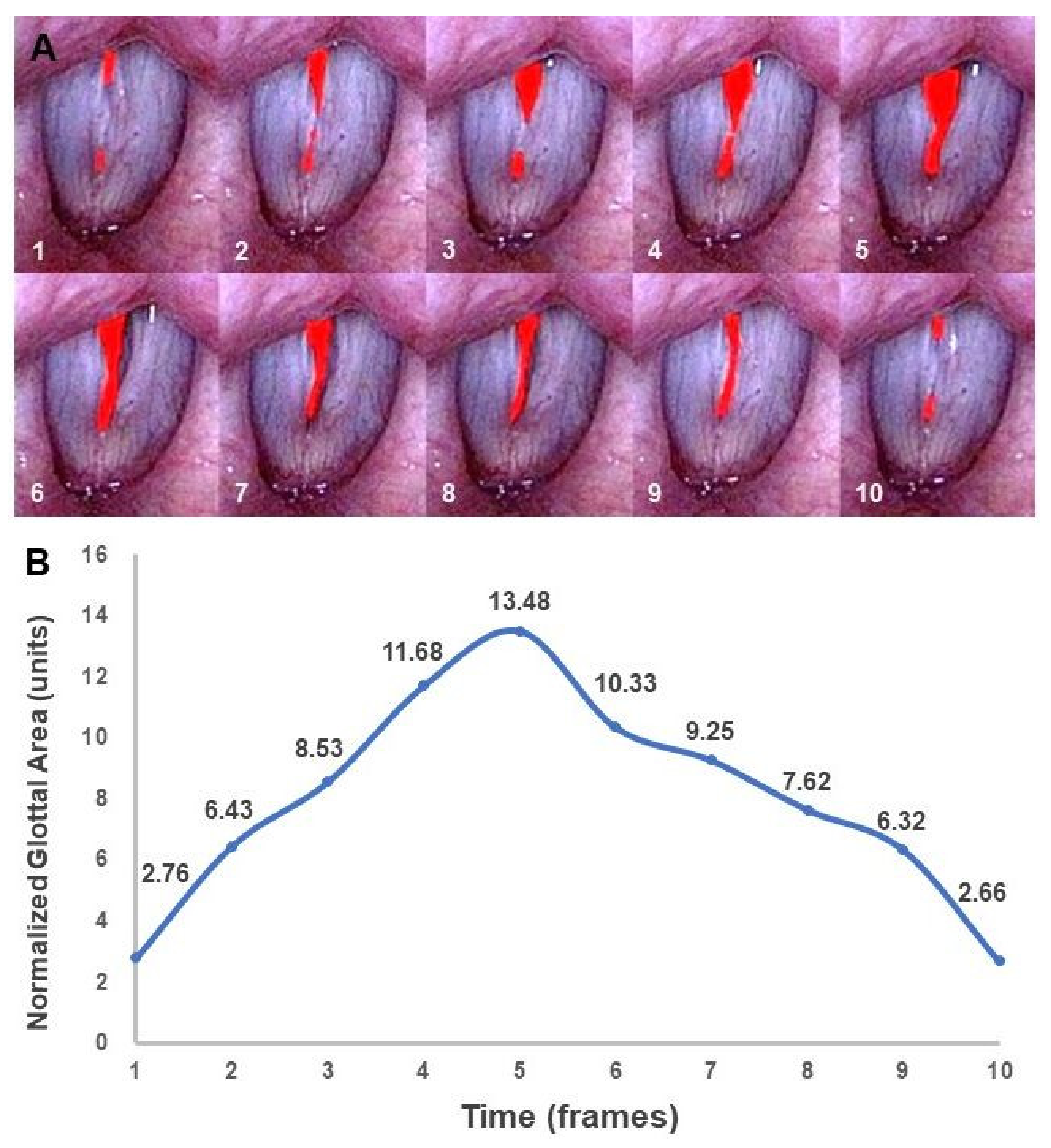
2.4. GA Measurement
2.5. Statistical Analysis
3. Results
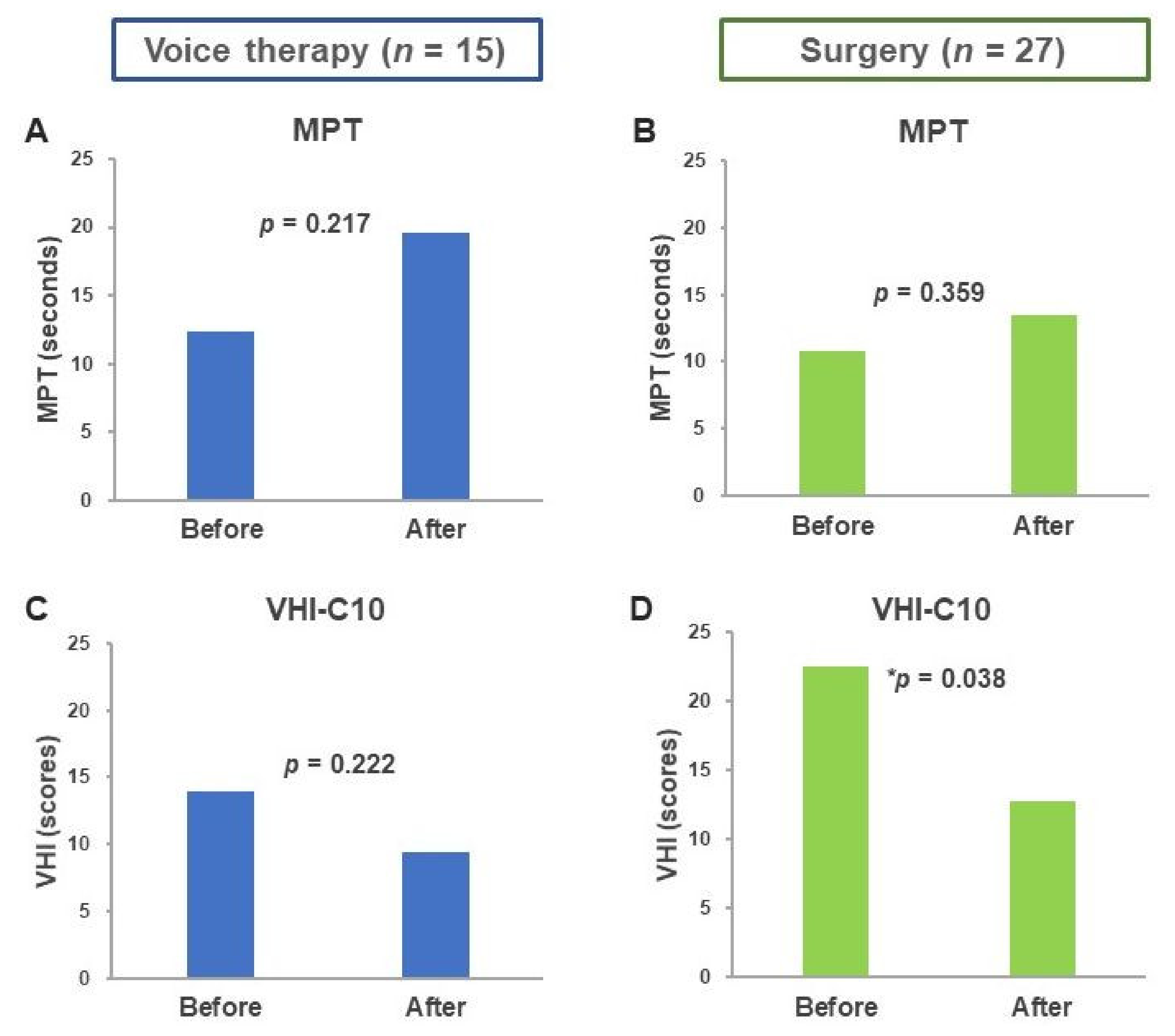
3.1. Objective Voice Parameters
3.2. VHI-C10 Scores before and after Treatment
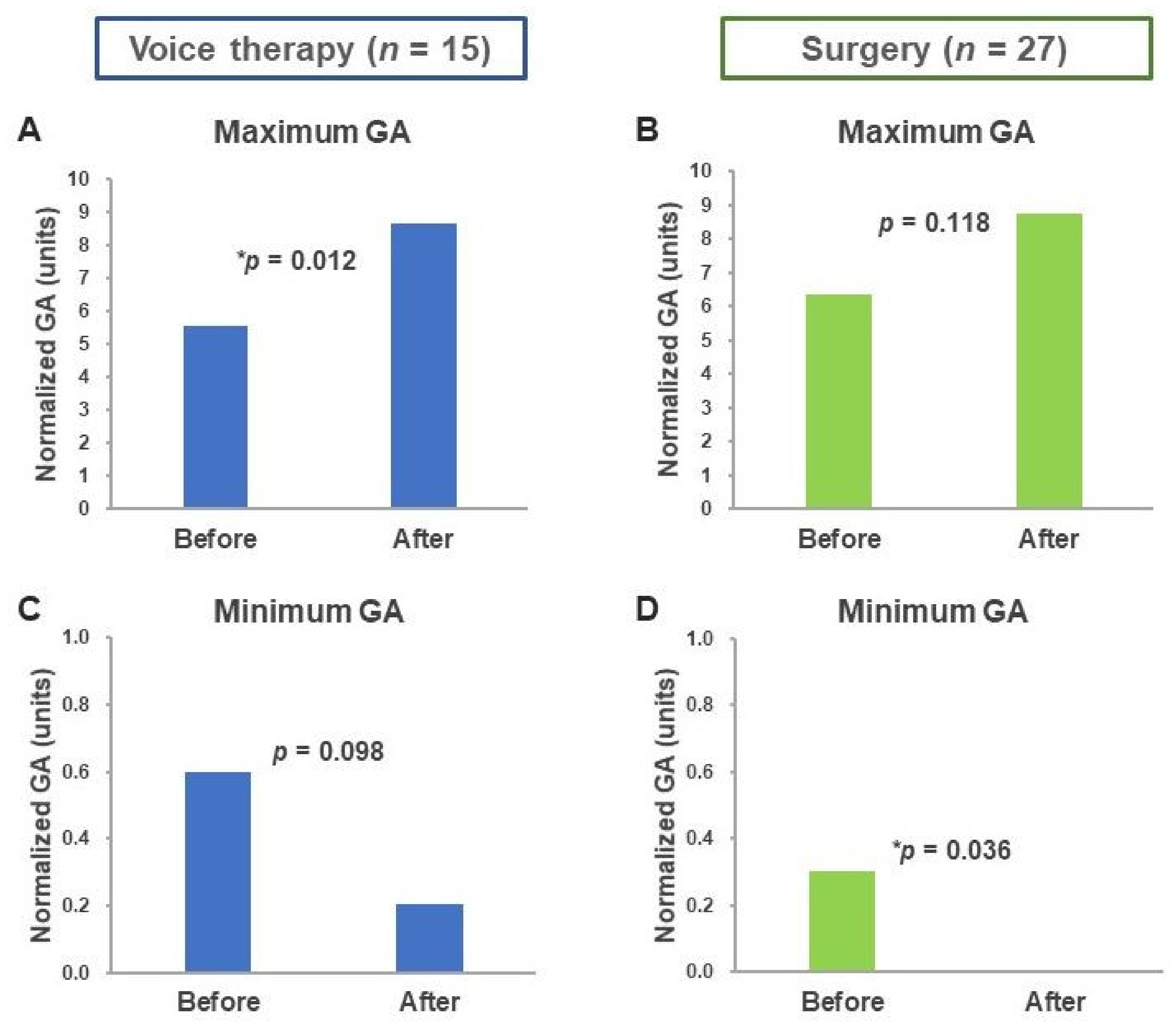
3.3. Maximum and Minimum Glottal Area
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
References
- Wallis, L.; Jackson-Menaldi, C.; Holland, W.; Giraldo, A. Vocal fold nodule vs. vocal fold polyp: Answer from surgical pathologist and voice pathologist point of view. J. Voice 2004, 18, 125–129. [Google Scholar] [CrossRef] [PubMed]
- Leonard, R. Voice therapy and vocal nodules in adults. Curr. Opin. Otolaryngol. Head Neck Surg. 2009, 17, 453–457. [Google Scholar] [CrossRef] [PubMed]
- McHugh-Munier, C.; Scherer, K.R.; Lehmann, W.; Scherer, U. Coping strategies, personality, and voice quality in patients with vocal fold nodules and polyps. J. Voice 1997, 11, 452–461. [Google Scholar] [CrossRef] [Green Version]
- Song, B.H.; Merchant, M.; Schloegel, L. Voice Outcomes of Adults Diagnosed with Pediatric Vocal Fold Nodules and Impact of Speech Therapy. Otolaryngol. Head Neck Surg. 2017, 157, 824–829. [Google Scholar] [CrossRef]
- Tsai, M.-S.; Yang, Y.-H.; Liu, C.-Y.; Lin, M.-H.; Chang, G.-H.; Tsai, Y.-T.; Li, H.-Y.; Tsai, Y.-H.; Hsu, C.-M. Unilateral vocal fold paralysis and risk of pneumonia: A nationwide population-based cohort study. Otolaryngol. Head Neck Surg. 2018, 158, 896–903. [Google Scholar] [CrossRef]
- Patel, R.R.; Dubrovskiy, D.; Dollinger, M. Measurement of glottal cycle characteristics between children and adults: Physiological variations. J. Voice 2014, 28, 476–486. [Google Scholar] [CrossRef] [Green Version]
- Powell, M.E.; Deliyski, D.D.; Hillman, R.E.; Zeitels, S.M.; Burns, J.A.; Mehta, D.D. Comparison of Videostroboscopy to Stroboscopy Derived From High-Speed Videoendoscopy for Evaluating Patients With Vocal Fold Mass Lesions. Am. J. Speech Lang. Pathol. 2016, 25, 576–589. [Google Scholar] [CrossRef]
- Harden, J. Comparison of glottal area changes as measured from ultrahigh-speed photographs and photoelectric glottographs. J. Speech Hear Res. 1975, 18, 728–738. [Google Scholar] [CrossRef]
- Selamtzis, A.; Ternstrom, S.; Richter, B.; Burk, F.; Koberlein, M.; Echternach, M. A comparison of electroglottographic and glottal area waveforms for phonation type differentiation in male professional singers. J. Acoust. Soc. Am. 2018, 144, 3275. [Google Scholar] [CrossRef]
- Chen, G.; Kreiman, J.; Gerratt, B.R.; Neubauer, J.; Shue, Y.-L.; Alwan, A. Development of a glottal area index that integrates glottal gap size and open quotient. J. Acoust. Soc. Am. 2013, 133, 1656–1666. [Google Scholar] [CrossRef] [Green Version]
- Timcke, R.; von Leden, H.; Moore, P. Laryngeal vibrations: Measurements of the glottic wave: Part I. The normal vibratory cycle. AMA Arch. Otolaryngol. 1958, 68, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Woo, P. Quantification of videostrobolaryngoscopic findings—Measurements of the normal glottal cycle. Laryngoscope 1996, 106, 1–27. [Google Scholar] [CrossRef] [PubMed]
- Gora, S.; Yavin, N.; Elad, D.; Wolf, M.; Primov-Fever, A. Computerized analysis of vocal folds vibration from laryngeal videostroboscopy. J. Voice 2016, 30, 478–484. [Google Scholar] [CrossRef] [PubMed]
- Schlegel, P.; Kniesburges, S.; Dürr, S.; Schützenberger, A.; Döllinger, M. Machine learning based identification of relevant parameters for functional voice disorders derived from endoscopic high-speed recordings. Sci. Rep. 2020, 10, 1–14. [Google Scholar] [CrossRef]
- Echternach, M.; Raschka, J.; Kuranova, L.; Köberlein, M.; Richter, B.; Döllinger, M.; Kainz, M.-A. Immediate effects of water resistance therapy on patients with vocal fold mass lesions. Eur. Arch. Oto-Rhino-Laryngol. 2020, 277, 1995–2003. [Google Scholar] [CrossRef] [Green Version]
- Powell, M.E.; Deliyski, D.D.; Zeitels, S.M.; Burns, J.A.; Hillman, R.E.; Gerlach, T.T.; Mehta, D.D. Efficacy of videostroboscopy and high-speed videoendoscopy to obtain functional outcomes from perioperative ratings in patients with vocal fold mass lesions. J. Voice 2019. In Press. [Google Scholar] [CrossRef]
- Ghasemzadeh, H.; Deliyski, D.D.; Ford, D.S.; Kobler, J.B.; Hillman, R.E.; Mehta, D.D. Method for vertical calibration of laser-projection transnasal fiberoptic high-speed videoendoscopy. J. Voice 2019. [Google Scholar] [CrossRef]
- Niebudek-Bogusz, E.; Kopczynski, B.; Strumillo, P.; Morawska, J.; Wiktorowicz, J.; Sliwinska-Kowalska, M. Quantitative assessment of videolaryngostroboscopic images in patients with glottic pathologies. Logop. Phoniatr. Vocology 2017, 42, 73–83. [Google Scholar] [CrossRef]
- Murphy, P.J. Spectral characterization of jitter, shimmer, and additive noise in synthetically generated voice signals. J. Acoust. Soc. Am. 2000, 107, 978–988. [Google Scholar] [CrossRef]
- Wertzner, H.F.; Schreiber, S.; Amaro, L. Analysis of fundamental frequency, jitter, shimmer and vocal intensity in children with phonological disorders. Braz. J. Otorhinolaryngol. 2005, 71, 582–588. [Google Scholar] [CrossRef] [Green Version]
- Jotz, G.P.; Cervantes, O.; Abrahão, M.; Settanni, F.A.P.; de Angelis, E.C. Noise-to-harmonics ratio as an acoustic measure of voice disorders in boys. J. Voice 2002, 16, 28–31. [Google Scholar] [CrossRef]
- Tsai, M.S.; Yang, M.Y.; Chang, G.H.; Tsai, Y.T.; Lin, M.H.; Hsu, C.M. Autologous thyroid cartilage graft implantation in medialization laryngoplasty: A modified approach for treating unilateral vocal fold paralysis. Sci. Rep. 2017, 7, 4790. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lam, P.K.; Chan, K.M.; Ho, W.K.; Kwong, E.; Yiu, E.M.; Wei, W.I. Cross-cultural adaptation and validation of the Chinese Voice Handicap Index-10. Laryngoscope 2006, 116, 1192–1198. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.; Han, D.; Li, H.; Hu, R.; Zhang, L. Application of the Mandarin Chinese version of the Voice Handicap Index. J. Voice 2010, 24, 702–707. [Google Scholar] [CrossRef] [PubMed]
- Omori, K.; Slavit, D.H.; Kacker, A.; Blaugrund, S.M. Quantitative videostroboscopic measurement of glottal gap and vocal function: An analysis of thyroplasty type I. Ann. Otol. Rhinol. Laryngol. 1996, 105, 280–285. [Google Scholar] [CrossRef]
- Noordzij, J.P.; Woo, P. Glottal area waveform analysis of benign vocal fold lesions before and after surgery. Ann. Otol. Rhinol. Laryngol. 2000, 109, 441–446. [Google Scholar] [CrossRef]
- Yamauchi, A.; Yokonishi, H.; Imagawa, H.; Sakakibara, K.; Nito, T.; Tayama, N.; Yamasoba, T. Age- and gender-related difference of vocal fold vibration and glottal configuration in normal speakers: Analysis with glottal area waveform. J. Voice 2014, 28, 525–531. [Google Scholar] [CrossRef]
- Teixeira, J.P.; Gonçalves, A. Algorithm for jitter and shimmer measurement in pathologic voices. Procedia Comput. Sci. 2016, 100, 271–279. [Google Scholar] [CrossRef] [Green Version]
- Remacle, M.; Friedrich, G.; Dikkers, F.G.; de Jong, F. Phonosurgery of the vocal folds: A classification proposal. Eur. Arch. Oto-Rhino-Laryngol. 2003, 260, 1–6. [Google Scholar] [CrossRef]
- Salturk, Z.; Ozdemir, E.; Sari, H.; Keten, S.; Kumral, T.L.; Berkiten, G.; Tutar, B.; Uyar, Y. Assessment of Resonant Voice Therapy in the Treatment of Vocal Fold Nodules. J. Voice 2018. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total Patients (n = 42) | p Value | |
|---|---|---|---|
| Treatment | Voice therapy (n = 15) | Surgery (n = 27) | |
| Sex (Male/Female) | 5/10 | 12/15 | 0.482 |
| Mean age year (range) | 52.28 (25–75) | 48.0 (23–67) | 0.324 |
| MPT (sec) | 12.37 ± 5.47 | 10.77 ± 4.85 | 0.666 |
| Jitter | 2.38 ± 2.16 | 3.10 ± 2.85 | 0.418 |
| Shimmer | 0.55 ± 0.41 | 0.58 ± 0.3 | 0.785 |
| NHR | 0.20 ± 0.14 | 0.18 ±0.09 | 0.624 |
| VHI-C10 | 14.00 ± 8.44 | 22.53 ± 7.17 | 0.01 * |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, C.-M.; Yang, M.-Y.; Fang, T.-J.; Wu, C.-Y.; Tsai, Y.-T.; Chang, G.-H.; Tsai, M.-S. Maximum and Minimum Phonatory Glottal Area before and after Treatment for Vocal Nodules. Healthcare 2020, 8, 326. https://doi.org/10.3390/healthcare8030326
Hsu C-M, Yang M-Y, Fang T-J, Wu C-Y, Tsai Y-T, Chang G-H, Tsai M-S. Maximum and Minimum Phonatory Glottal Area before and after Treatment for Vocal Nodules. Healthcare. 2020; 8(3):326. https://doi.org/10.3390/healthcare8030326
Chicago/Turabian StyleHsu, Cheng-Ming, Ming-Yu Yang, Tuan-Jen Fang, Ching-Yuan Wu, Yao-Te Tsai, Geng-He Chang, and Ming-Shao Tsai. 2020. "Maximum and Minimum Phonatory Glottal Area before and after Treatment for Vocal Nodules" Healthcare 8, no. 3: 326. https://doi.org/10.3390/healthcare8030326