Long-Term Socioeconomic Impact of Informal Care Provided to Patients with Pacemakers: Remote vs. Conventional Monitoring

 ,
, 
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Data Collection
2.4. Ethical Considerations
2.5. Statistical Analysis
3. Results
3.1. Main Characteristics of the Informal Caregivers
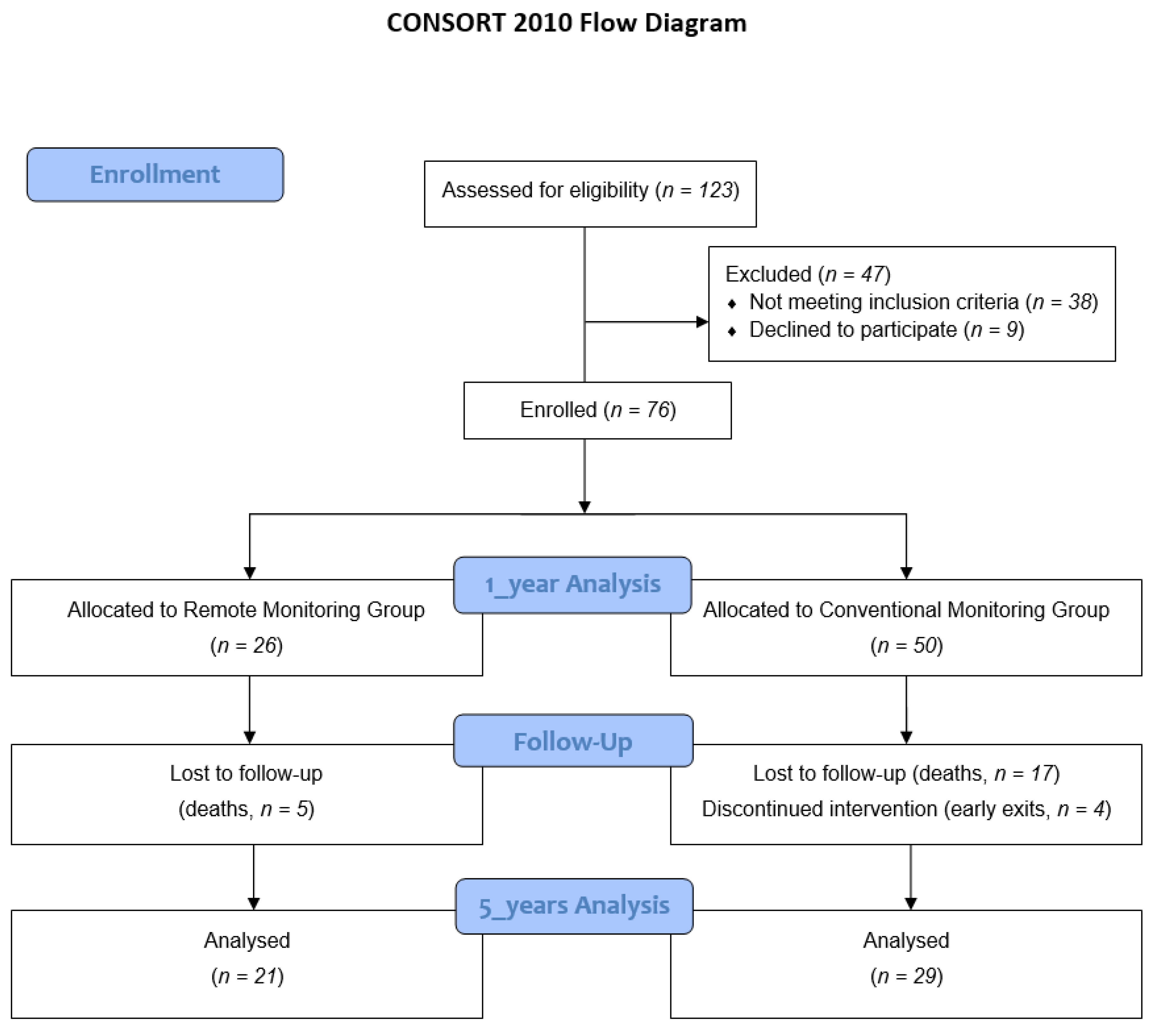
3.2. Attrition
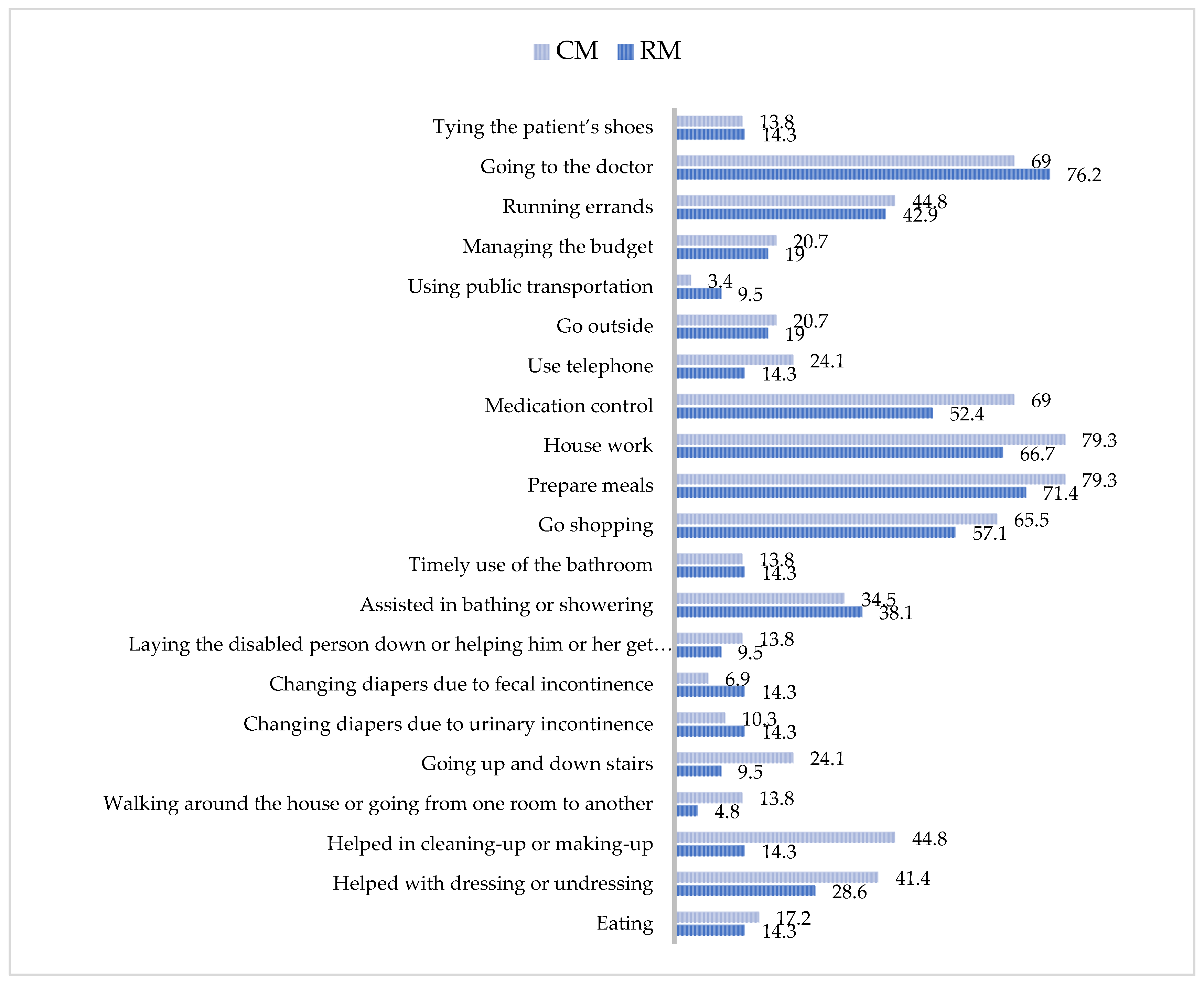
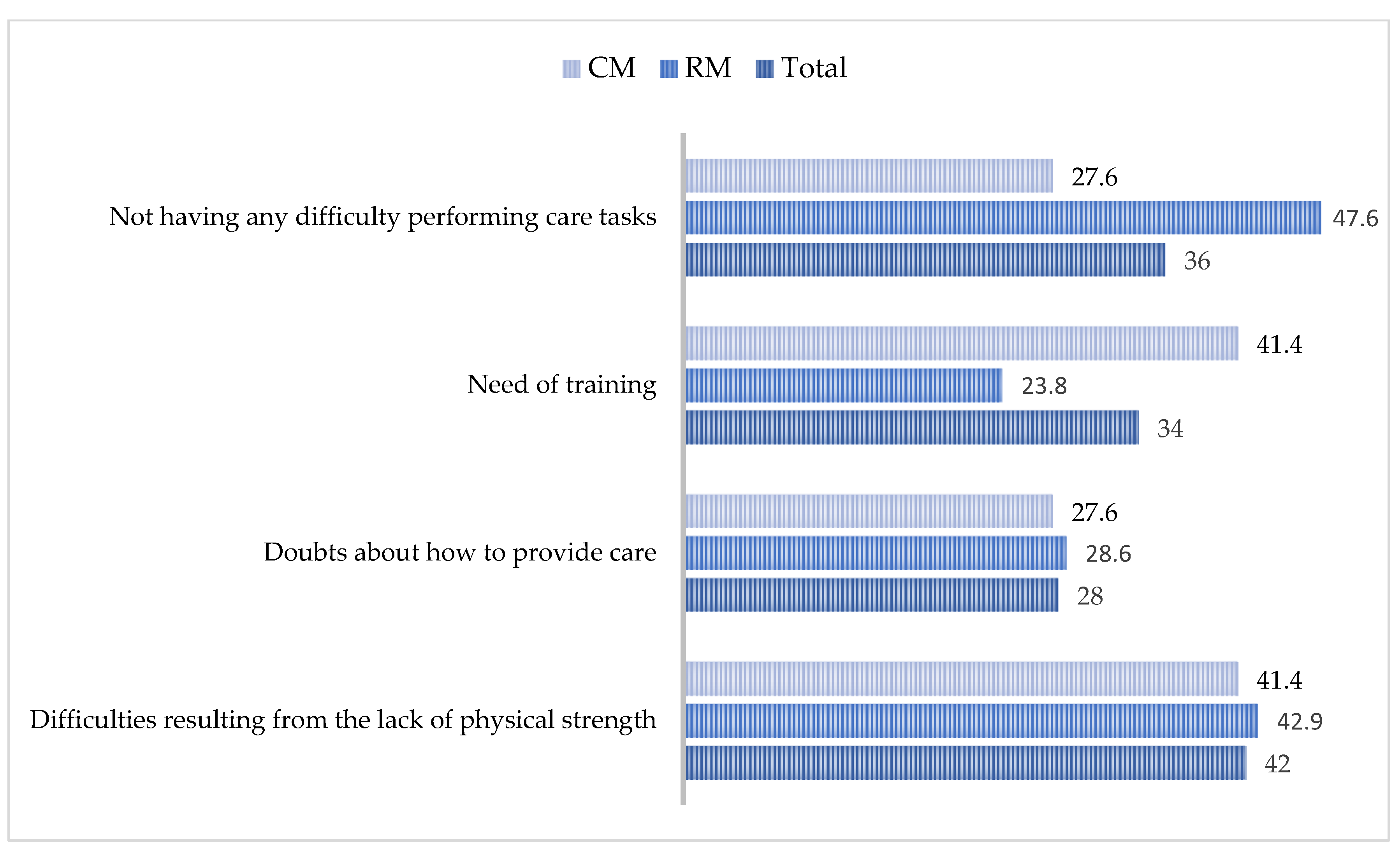
3.3. Workload and Activities Performed by the Informal Caregivers
3.4. Time and Costs of Informal Care
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Jiménez, M.P.; Pérez, O.C.; Carreño, D.L.; García, J.C.; Jiménez, M.P.; Pérez, O.C.; Carreño, D.L.; García, J.C. Spanish Pacemaker Registry. 15th Official Report of the Spanish Society of Cardiology Working Group on Cardiac Pacing (2017). Rev. Esp. Cardiol. 2018, 71, 1059–1068. [Google Scholar]
- Greenspon, A.J.; Patel, J.D.; Lau, E.; Ochoa, J.A.; Frisch, D.R.; Ho, R.T.; Pavri, B.B.; Kurtz, S.M. Trends in permanent pacemaker implantation in the United States from 1993 to 2009: Increasing complexity of patients and procedures. J. Am. Coll. Cardiol. 2012, 60, 1540–1545. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.H.; Lee, S.R.; Choi, E.K.; Jeong, J.; Park, H.D.; You, S.J.; Lee, S.S.; Oh, S. Temporal Trends of Cardiac Implantable Electronic Device Implantations: A Nationwide Population-based Study. Korean Circ. J. 2019, 49, 841–852. [Google Scholar] [CrossRef]
- Cardiac Rate Book, 2016: Cardiac Implants—Provincial Data. Available online: https://www.cihi.ca/en/cardiac-rate-book-2016-cardiac-implants-provincial-data (accessed on 13 June 2019).
- Raatikainen, M.J.P.; Arnar, D.O.; Merkely, B.; Nielsen, J.C.; Hindricks, G.; Heidbuchel, H.; Camm, J. A Decade of Information on the Use of Cardiac Implantable Electronic Devices and Interventional Electrophysiological Procedures in the European Society of Cardiology Countries: 2017 Report from the European Heart Rhythm Association. Europace 2017, 19 (Suppl. 2), ii1–ii90. [Google Scholar] [CrossRef]
- Lopez-Villegas, A.; Catalan-Matamoros, D.; Robles-Musso, E.; Peiro, S. Effectiveness of pacemaker tele-monitoring on quality of life, functional capacity, event detection and workload: The PONIENTE trial. Geriatr. Gerontol. Int. 2016, 16, 1188–1195. [Google Scholar] [CrossRef]
- Lopez-Villegas, A.; Catalan-Matamoros, D.; Lopez-Liria, R.; Enebakk, T.; Thunhaug, H.; Lappegård, K.T. Health-related quality of life on tele-monitoring for users with pacemakers 6 months after implant: The NORDLAND study, a randomized trial. BMC Geriatr. 2018, 18, 223. [Google Scholar] [CrossRef]
- López-Villegas, A.; Catalán-Matamoros, D.; Robles-Musso, E.; Peiró, S. Workload, time and costs of the informal cares in patients with tele-monitoring of pacemakers: The PONIENTE study. Clin Res Cardiol. 2016, 105, 307–313. [Google Scholar] [CrossRef]
- Klersy, C.; Boriani, G.; De Silvestri, A.; Mairesse, G.H.; Braunschweig, F.; Scotti, V.; Balduini, A.; Cowie, M.R.; Leyva, F. Health Economics Committee of the European Heart Rhythm Association Effect of telemonitoring of cardiac implantable electronic devices on healthcare utilization: A meta-analysis of randomized controlled trials in patients with heart failure. Eur. J. Heart Fail. 2016, 18, 195–204. [Google Scholar] [CrossRef]
- Health Quality Ontario. Remote Monitoring of Implantable Cardioverter-Defibrillators, Cardiac Resynchronization Therapy and Permanent Pacemakers: A Health Technology Assessment. Ont. Health Technol. Assess. Ser. 2018, 18, 1–199. [Google Scholar]
- Mairesse, G.H.; Braunschweig, F.; Klersy, K.; Cowie, M.R.; Leyva, F. Implementation and reimbursement of remote monitoring for cardiac implantable electronic devices in Europe: A survey from the health economics committee of the European Heart Rhythm Association. Europace. 2015, 17, 814–818. [Google Scholar] [CrossRef] [PubMed]
- López-Villegas, A.; Catalán-Matamoros, D.; Robles-Musso, E.; Peiró, S. Comparative Effectiveness of Remote Monitoring of People with Cardiac Pacemaker versus Conventional: Quality of Life at the 6 Months. Rev. Esp. Salud Publica 2015, 89, 149–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mabo, P.; Victor, F.; Bazin, P.; Ahres, S.; Babuty, D.; Da Costa, A.; Binet, D.; Daubert, J.-C. COMPAS Trial Investigators A randomized trial of long-term remote monitoring of pacemaker recipients (the COMPAS trial). Eur. Heart J. 2012, 33, 1105–1111. [Google Scholar] [CrossRef] [Green Version]
- Survey on Disability, Personal Autonomy and Dependency Situations 2008. Available online: https://www.ine.es/dyngs/INEbase/en/operacion.htm?c=Estadistica_C&cid=1254736176782&menu=resultados&secc=1254736194716&idp=1254735573175#!tabs-1254736194716 (accessed on 15 June 2020).
- Rudmik, L.; Drummond, M. Health economic evaluation: Important principles and methodology. Laryngoscope 2013, 123, 1341–1347. [Google Scholar] [CrossRef]
- van den Berg, B.; Spauwen, P. Measurement of informal care: An empirical study into the valid measurement of time spent on informal caregiving. Health Econ. 2006, 15, 447–460. [Google Scholar] [CrossRef] [Green Version]
- Labour and Social Economy Ministry. Available online: http://www.mitramiss.gob.es/es/portada/serviciohogar/preguntas-frecuentes/retribuciones/ (accessed on 15 June 2020).
- WMA—The World Medical Association—Declaration of Helsinki—Ethical Principles for Medical Research Involving Human Subjects. Available online: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/ (accessed on 15 June 2020).
- Ley 41/2002, de 14 de Noviembre, Básica Reguladora de la Autonomía del Paciente y de Derechos y Obligaciones en Materia de Información y Documentación Clínica. Available online: https://www.boe.es/buscar/act.php?id=BOE-A-2002-22188 (accessed on 15 June 2020).
- Ley Orgánica 3/2018, de 5 de Diciembre, de Protección de Datos Personales y Garantía de Los Derechos Digitales. Available online: https://www.boe.es/boe/dias/2018/12/06/pdfs/BOE-A-2018-16673.pdf (accessed on 15 June 2020).
- Grant, J.S.; Graven, L.J. Problems experienced by informal caregivers of individuals with heart failure: An integrative review. Int. J. Nurs. Stud. 2018, 80, 41–66. [Google Scholar] [CrossRef]
- Ni, P.W.; Mao, B.Q.; Yang, Y.; Li, J.J.; Liu, H.; Huang, Y.; Xie, T. Study on the relationship between uncertainty in illness and caregiving burden in family members of patients with chronic wounds. Zhonghua Shao Shang Za Zhi (Chin. J. Burns) 2019, 35, 379–383. [Google Scholar]
- Hamilton, H. The Lived Experience of African American Caregivers Caring for Adult African American Patients with Heart Failure. Home Healthc. Now 2016, 34, 196–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noonan, M.C.; Wingham, J.; Taylor, R.S. “Who Cares?” The experiences of caregivers of adults living with heart failure, chronic obstructive pulmonary disease and coronary artery disease: A mixed methods systematic review. BMJ Open 2018, 8, e020927. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malik, F.A.; Gysels, M.; Higginson, I.J. Living with breathlessness: A survey of caregivers of breathless patients with lung cancer or heart failure. Palliat. Med. 2013, 27, 647–656. [Google Scholar] [CrossRef] [PubMed]
- von Känel, R.; Mausbach, B.T.; Dimsdale, J.E.; Ziegler, M.G.; Mills, P.J.; Allison, M.A.; Patterson, T.L.; Ancoli-Israel, S.; Grant, I. Refining caregiver vulnerability for clinical practice: Determinants of self-rated health in spousal dementia caregivers. BMC Geriatr. 2019, 19, 18. [Google Scholar] [CrossRef]
- Strøm, A.; Andersen, K.L.; Korneliussen, K.; Fagermoen, M.S. Being “on the alert” and “a forced volunteer”: A qualitative study of the invisible care provided by the next of kin of patients with chronic heart failure. J. Multidiscip. Healthc. 2015, 8, 271–277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harkness, K.; Arthur, H.; McKelvie, R. The measurement of uncertainty in caregivers of patients with heart failure. J. Nurs. Meas. 2013, 21, 23–42. [Google Scholar] [CrossRef] [PubMed]
- Lilly, M.B.; Laporte, A.; Coyte, P.C. Labor market work and home care’s unpaid caregivers: A systematic review of labor force participation rates, predictors of labor market withdrawal, and hours of work. Milbank Q. 2007, 85, 641–690. [Google Scholar] [CrossRef] [Green Version]
- Sullivan, B.-J.; Marcuccilli, L.; Sloan, R.; Gradus-Pizlo, I.; Bakas, T.; Jung, M.; Pressler, S.J. Competence, Compassion, and Care of the Self: Family Caregiving Needs and Concerns in Heart Failure. J. Cardiovasc. Nurs. 2016, 31, 209–214. [Google Scholar] [CrossRef] [Green Version]
- Etemadifar, S.; Bahrami, M.; Shahriari, M.; Farsani, A.K. Family caregivers’ experiences of caring for patients with heart failure: A descriptive, exploratory qualitative study. J. Nurs. Res. JNR 2015, 23, 153–161. [Google Scholar] [CrossRef]
- Ricci, R.P.; Vicentini, A.; D’Onofrio, A.; Sagone, A.; Rovaris, G.; Padeletti, L.; Morichelli, L.; Fusco, A.; De Vivo, S.; Lombardi, L.; et al. Economic analysis of remote monitoring of cardiac implantable electronic devices: Results of the Health Economics Evaluation Registry for Remote Follow-up (TARIFF) study. Heart Rhythm 2017, 14, 50–57. [Google Scholar] [CrossRef] [Green Version]
- Neumann, A.; Mostardt, S.; Biermann, J.; Gelbrich, G.; Goehler, A.; Geisler, B.P.; Siebert, U.; Störk, S.; Ertl, G.; Angerrmann, C.E.; et al. Cost-effectiveness and cost-utility of a structured collaborative disease management in the Interdisciplinary Network for Heart Failure (INH) study. Clin. Res. Cardiol. 2015, 104, 304–309. [Google Scholar] [CrossRef]
- Herold, R.; Hoffmann, W.; van den Berg, N. Telemedical monitoring of patients with chronic heart failure has a positive effect on total health costs. BMC Health Serv. Res. 2018, 18, 271. [Google Scholar] [CrossRef] [Green Version]
- López-Villegas, A.; Catalán-Matamoros, D.; Martín-Saborido, C.; Villegas-Tripiana, I.; Robles-Musso, E. A Systematic Review of Economic Evaluations of Pacemaker Telemonitoring Systems. Rev. Espanola Cardiol. 2016, 69, 125–133. [Google Scholar] [CrossRef]
- Lopez-Villegas, A.; Catalan-Matamoros, D.; Robles-Musso, E.; Bautista-Mesa, R.; Peiro, S. Cost-utility analysis on telemonitoring of users with pacemakers: The PONIENTE study. J. Telemed. Telecare 2019, 25, 204–212. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Total n = 50 | Remote monitoring n = 21 | Conventional monitoring n = 29 | p | |||
|---|---|---|---|---|---|---|---|
| Age (mean, SD) | 63.14 | 14.9 | 62.9 | 15.14 | 63.32 | 14.99 | 0.92 |
| Sex (n %) | |||||||
| Male | 2 | 4 | 2 | 9.5 | 0 | 0 | 0.17 |
| Female | 48 | 96 | 19 | 90.5 | 29 | 100 | |
| Marital status (n, %) | |||||||
| Single | 10 | 20 | 5 | 23.8 | 5 | 17.2 | 0.77 |
| Married | 36 | 72 | 14 | 66.7 | 22 | 75.9 | |
| Widower | 4 | 8 | 2 | 9.5 | 2 | 6.9 | |
| Separated | 0 | 0 | 0 | 0 | 0 | 0 | |
| Divorced | 0 | 0 | 0 | 0 | 0 | 0 | |
| Type of caregiver (n, %) | |||||||
| Lives at the patient’s home-non-domestic worker | 35 | 70 | 17 | 81 | 18 | 62.1 | 0.49 |
| Lives at the patient’s home-domestic worker | 1 | 2 | 0 | 0 | 1 | 3.4 | |
| Does not live at the patient’s home-non-domestic worker | 11 | 22 | 3 | 14.3 | 8 | 27.6 | |
| Does not live at the patient’s home-domestic worker | 3 | 6 | 1 | 4.8 | 2 | 6.9 | |
| Health problems-general status (n, %) | |||||||
| Deterioration of health status | 11 | 22 | 5 | 23.8 | 6 | 20.7 | 0.53 |
| Fatigue | 8 | 16 | 4 | 19 | 4 | 13.8 | 0.45 |
| Depression | 2 | 4 | 1 | 4.8 | 1 | 3.4 | 0.67 |
| Treatment | 2 | 4 | 2 | 9.5 | 0 | 0 | 0.17 |
| Other health problems | 23 | 46 | 10 | 47.6 | 13 | 44.8 | 0.54 |
| Professional or economic problem (n, %) | |||||||
| Loss of employment | 2 | 4.1 | 0 | 0 | 2 | 7.1 | 0.32 |
| Reduction of working hours | 6 | 12.5 | 1 | 4.8 | 5 | 18.5 | 0.16 |
| Problems with working time | 4 | 8.2 | 1 | 4.8 | 3 | 10.7 | 0.42 |
| Cannot work out of the home | 7 | 14.3 | 2 | 9.5 | 5 | 17.9 | 0.35 |
| Economic problems | 3 | 6.1 | 1 | 4.8 | 2 | 7.1 | 0.61 |
| Loss of employment opportunities | 4 | 8.2 | 1 | 4.8 | 3 | 10.7 | 0.42 |
| Problems related to leisure, free time, or family life (n, %) | |||||||
| Reduction in leisure time | 23 | 46.9 | 7 | 33.3 | 16 | 57.1 | 0.09 |
| Reduction in holidays time | 13 | 26.5 | 4 | 19 | 9 | 32.1 | 0.24 |
| Time for providing care to other individuals | 8 | 16.3 | 1 | 4.8 | 7 | 25 | 0.62 |
| Time with friends | 4 | 8.2 | 1 | 4.8 | 3 | 10.7 | 0.42 |
| Time for self-care | 2 | 4.1 | 1 | 4.8 | 1 | 3.6 | 0.68 |
| Conflicts with the couple | 1 | 2 | 1 | 4.8 | 0 | 0 | 0.43 |
| Variables | Total n = 50 | Remote Monitoring n = 21 | Conventional Monitoring n = 29 | p | |||
|---|---|---|---|---|---|---|---|
| Hours per day (mean, SD) | 16.24 | 7.45 | 15.14 | 8.38 | 17.03 | 6.73 | 0.38 |
| Days per week (n, %) | |||||||
| <1 day | 1 | 2 | 1 | 4.8 | 0 | 0 | 0.55 |
| 1 day | 1 | 2 | 1 | 4.8 | 0 | 0 | |
| 2–3 days | 2 | 4 | 1 | 4.8 | 1 | 3.4 | |
| 4–5 days | 2 | 4 | 1 | 4.8 | 1 | 3.4 | |
| 6–7 days | 44 | 88 | 17 | 81 | 27 | 93.1 | |
| Hours per week (mean, SD) | 109.52 | 55.87 | 100.67 | 63.93 | 115.93 | 49.41 | 0.35 |
| Years (n %) | 0.85 | ||||||
| <1 | 7 | 14 | 4 | 19 | 3 | 10.3 | |
| From 1 to 2 | 10 | 20 | 5 | 23.8 | 5 | 17.2 | |
| From 2 to 4 | 14 | 28 | 5 | 23.8 | 9 | 31 | |
| From 4 to 8 | 16 | 32 | 6 | 28.6 | 10 | 35.5 | |
| >8 | 3 | 6 | 1 | 4.8 | 2 | 6.9 | |
| Informal costs (€) (mean, SD) | 185,044.99 | 94,394.59 | 170,086.40 | 108,009.37 | 195,877.08 | 15,504.03 | 0.35 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leal-Costa, C.; Lopez-Villegas, A.; Catalan-Matamoros, D.; Robles-Musso, E.; Lappegård, K.T.; Bautista-Mesa, R.J.; Peiró, S.; Lopez-Liria, R. Long-Term Socioeconomic Impact of Informal Care Provided to Patients with Pacemakers: Remote vs. Conventional Monitoring. Healthcare 2020, 8, 175. https://doi.org/10.3390/healthcare8020175
Leal-Costa C, Lopez-Villegas A, Catalan-Matamoros D, Robles-Musso E, Lappegård KT, Bautista-Mesa RJ, Peiró S, Lopez-Liria R. Long-Term Socioeconomic Impact of Informal Care Provided to Patients with Pacemakers: Remote vs. Conventional Monitoring. Healthcare. 2020; 8(2):175. https://doi.org/10.3390/healthcare8020175
Chicago/Turabian StyleLeal-Costa, Cesar, Antonio Lopez-Villegas, Daniel Catalan-Matamoros, Emilio Robles-Musso, Knut Tore Lappegård, Rafael Jesus Bautista-Mesa, Salvador Peiró, and Remedios Lopez-Liria. 2020. "Long-Term Socioeconomic Impact of Informal Care Provided to Patients with Pacemakers: Remote vs. Conventional Monitoring" Healthcare 8, no. 2: 175. https://doi.org/10.3390/healthcare8020175