1. Introduction
The health workforce is vital to the core functionality of a health system, yet it tends to be overlooked as a key element of upgrading health systems [
1]. Health worker shortage is an unfortunately rising phenomenon adversely affecting multiple health systems. There is minimal literature and knowledge on effective strategies on how to combat the hasty deterioration of human resource for health [
2], especially in developing countries. More than a decade ago in the World Health Organization (WHO) 2006 report Working Together for Health, 57 countries reported experiencing critical health workforce shortage [
3]. By 2018, according to the Global Health Observatory (GHO) by WHO, a global need for 17 million additional skilled health workers was reported [
4]. According to WHO, the African region is experiencing both the greatest burden of disease and the lowest density of health workers at 2.2 health workers per 1000 population of healthcare professionals [
5]. In the WHO 2006 report, 36 Member States, some of which are part of the East African Community (EAC), were and still are experiencing a critical shortage of human resource for health [
3]. Health workforce shortage crisis impedes the performance and quality of healthcare provided, contributing to sub-optimal functionality of health systems. Borghi and colleagues [
6] state that the ability of a health system to deliver quality healthcare among the current workforce is partly dependent on healthcare workers’ motivation.
Motivation is a determinant of behaviour characterised by the driving force one has to achieve a certain goal [
7]. In the context of health systems strengthening, motivation is one of the driving forces among health workers that can potentially contribute towards the progress of attaining the WHO health system goals, namely improved health level and equity, responsiveness to clients’ non-medical expectations, social and financial risk protection and improved efficiency [
8]. According to WHO, motivation is a worthy investment to effectively perform Primary Health Care (PHC) and health workforce strengthening [
8,
9,
10]. The significance of investing in health workforce motivation was affirmed in the Global Conference on Primary Health Care 2018 report [
9].
Assessing motivation is complex due to various determining factors, both external and internal in nature [
6,
11,
12]. The Hawthorne studies done between 1924 and 1932 by Elton Mayo and Fritz Roethlisberger reported a novel element: that employee motivation was not exclusively monetary-based as previously assumed by employer, employees, researchers and policymakers [
13]. Thus, the Hawthorne Effect, which is the overt observation of employee performance resulting in behavioural change such as higher performance [
13]. Following the discovery of the Hawthorne Effect, researchers began paying attention to non-monetary motivators [
13]. Researchers have found employees are motivated by intrinsic and extrinsic factors [
13].
Intrinsic motivation occurs when an individual is driven by interest and satisfaction doing the work itself [
14]. On the other hand, extrinsic motivation is when an individual is driven by the external consequences of performing a task [
14]. There are multiple theories on human motivation, with the most common being Maslow’s Hierarchy of Needs. Nonetheless, three theories, namely the Two-Factor theory by Herzberg, Cognitive Evaluation Theory by Porter and Lawler and Self-determination Theory by Ryan and Deci [
15], similarly view motivation from the perspective of intrinsic and extrinsic factors or motivators.
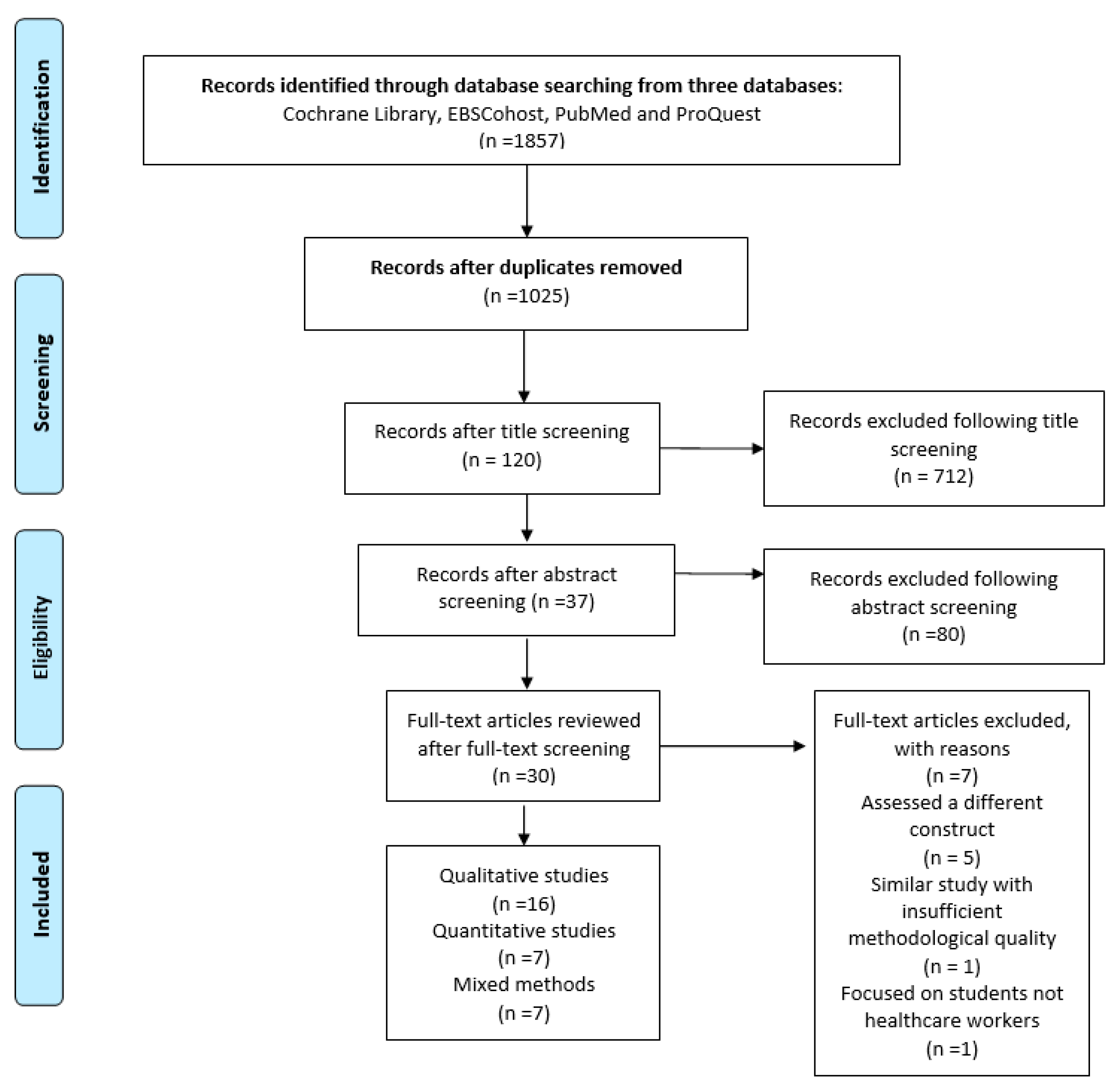
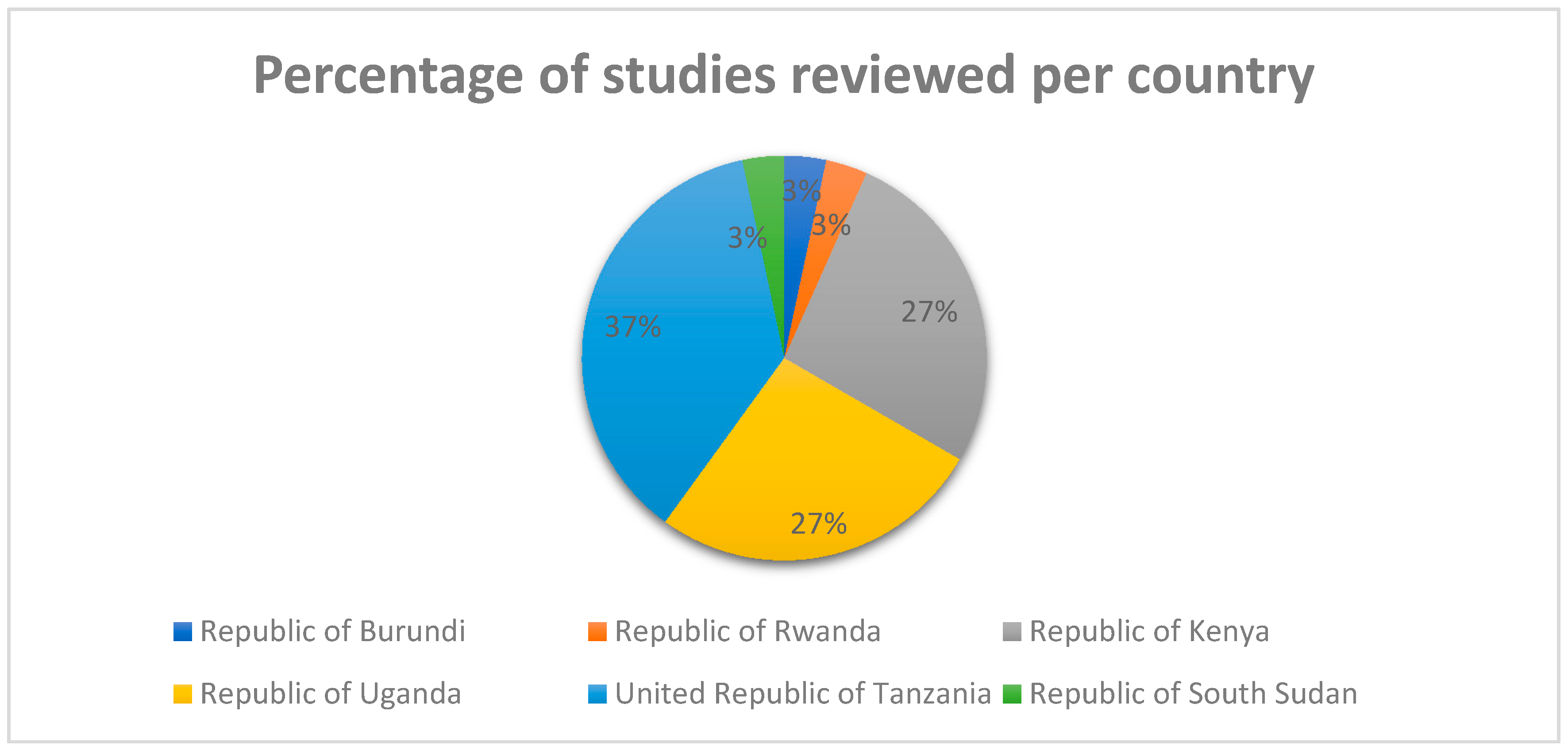
In this study, we aimed to do a systematic review, to consolidate the existing evidence on the determinants of motivation among healthcare workers in the East African Community (EAC). The EAC consists of six countries, namely the Republic of Burundi, Republic of Kenya, Republic of Rwanda, Republic of South Sudan, Republic of Uganda and United Republic of Tanzania, which are connected by a common integration agenda [
16]. The EAC countries are either low- or lower-middle-income developing countries, with most populations living in the rural areas. The EAC state health systems have been described as resource-limited settings [
17,
18,
19,
20], severely weakened [
21] and fragile [
22]. There are various studies that have been done about healthcare workers’ motivation. To date, there is no recent systematic review that has been done on determinants of healthcare workers’ motivation in the East African Community between 2009 and 2019. Using a narrative synthesis approach, we report on significant intrinsic and extrinsic determinants of motivation among healthcare workers in East Africa in the last 10 years (2009–2019).
This review answers the question, ‘What are the determinants of healthcare workers’ motivation in the East African Community between 2009 and 2019?’ The present review informs researchers what has been done in this area while simultaneously identifying the gaps in knowledge pertaining to this area of study. Healthcare workers will gain knowledge on the determinants of motivation among themselves and their colleagues within the health sector. Health policymakers and implementers will be able to use this information to create evidence-based policies to enhance healthcare workers’ motivation, thus progressively contributing to health systems strengthening among the countries within the East African Community.
4. Discussion
In this systematic review, we explored the determinants of healthcare workers’ motivation in the six East African Community (EAC) countries in the last decade (2009–2019). These countries are part of the Sub-Saharan Africa region, which has been described as having “severely weakened and under-resourced health systems” [
21]. Sub-Saharan Africa has one of the greatest health-related challenges, with approximately 25% of the worldwide burden of disease in this region coupled with the shortage crisis of skilled healthcare professionals [
3,
49]. As countries work towards achieving Universal Health Coverage (UHC) and the Sustainable Development Goal 3: Health for all at all ages (SDG3), we need to devise effective health system strategies on how to work with, attract and retain the present health workforce. One of the ways is to motivate to join and most significantly stay in the health system. It is evident that the numbers, training and quality of human resources for health varies from country to country [
1]; even with these similarities in determinants of healthcare workers’ motivation being discovered in this review among countries in the EAC. This review reports the individual, organizational/structural and societal determinants of healthcare workers’ motivation across the EAC states as reported by the health workforce.
Rudasingwa and colleagues stated that it is imperative that we integrate health workers’ definitions and perceptions of methods of enhancing quality of healthcare provision [
45] and health workforce strengthening [
10]. The motivating determinants of healthcare workers can also be viewed as facilitators of motivation, while the demotivating determinants can be viewed as barriers to their motivation. Both facilitators and barriers have been identified in this review at individual, organizational/structural and societal levels regarding the health workforce. Overall, motivating determinants were either individual-based while most demotivating determinants were organizational (health-facility-based) or structural (health-system-based). In our findings, while the individual determinants are mainly intrinsic in nature, the organizational and societal determinants are primarily extrinsic of the healthcare workers.
At the individual level, altruism is a prosocial behaviour that was the greatest motivating determinant among healthcare workers in the EAC. Altruism is a vital element of the medical discipline and has been described as a “core of competent health professionals’” [
51] (p. 374). Medical altruism is rooted in the Hippocratic Oath, taken by healthcare professionals in the United States [
51]. The desire to engage in prosocial behaviour involving saving lives, serving the community, sharing health-related knowledge and catalysing behavioural change within the community and public were some of the reasons for feeling a sense of responsibility to be altruistic [
11,
21,
30,
35,
36,
39,
42,
46]. According to the Theory-Based Model, altruism can be nurtured through education, practice and reinforcement [
51].
Medical altruism has been found to affect the professionalism depicted in healthy clinical and patient relationships, resulting in better patient health outcomes and adherence and satisfaction with the quality of healthcare provided [
47,
50,
51,
52]. In the United Kingdom, medical altruism is a vital element of health workforce planning, for example in the UK National Health Service [
52]. Examples of medical altruistic acts include working beyond contracted hours and providing additional information to their patients and their families, among other things [
52]. The discovery of altruism or medical altruism among healthcare workers means managers and policymakers should pay attention to more than just the numbers. Focusing on the numbers only (quantity) can result in depletion of health among healthcare workers and cause demoralization, which are barriers to motivation [
52].
In addition, a sense of usefulness within the community and in the health system after gaining knowledge and being able to use skills for the enhancement of healthy behaviour was echoed among respondents in various studies [
30,
34,
47]. Three demotivating determinants at the individual level included perceived fear of contracting illnesses [
42], being married [
32] and work conscientiousness following a supervision intervention [
37]. Health is a key concern among healthcare workers, particularly the risk and perceived fear of contracting illnesses’ [
42]. A study in India reported risk of poor personal health being a demotivating factor, due to its detrimental effects on their ability to do their work [
53]. As a result, health policymakers, managers and stakeholders ought to recognise the key role that feeling safe and protected through provision of protective gear plays and a safe working environment at large, have in reducing risk and fear of falling sick, thus increasing their motivation to work.
Work conscientiousness following a supervision intervention was found to decrease motivation among healthcare workers [
37]. A possible explanation is the role of the type of leadership or supervision instigating autonomous motivation or controlled motivation regulations. This means the supervision intervention may have reduced the work conscientiousness among healthcare workers due to highly controlled motivation regulations. A study done among 547 nurses in Canada reported nurses being motivated by autonomous motivation as opposed to controlled motivation [
54]. While autonomous motivation is self-regulated and intrinsic in nature, controlled motivation is the opposite and involves a lot of external control and complete lack of proactive independence in performing one’s work. Based on these finding, researchers encourage promotion of autonomous motivation over controlled motivation regulations to motivate and sustain healthcare workers [
54].
The societal level, consisting of the clients (patients), community and family, was reported to play a significant role in the motivation of healthcare workers. The society was reported as playing a significant a role in positive reinforcement of healthcare workers’ motivation through appreciating, admiring, respecting, and recognising the work they do [
11,
20,
30,
33,
34,
36,
40,
41]. The desire to instigate healthy behavioural change within the community and the public was a major determinant of motivation across the health workforce in the EAC at the societal level.
However, the lack of appreciation, lack of recognition, dissatisfaction, insecurity and inability to adequately support their family, community and clients constituted the main demotivating societal-level determinants. These barriers to motivation at the societal level created a sense of helplessness [
20] among healthcare professionals when receiving constant complaints or unexpected delays from the community or family of the clients occurred [
34,
43]. The presence of constantly escalating and irrational demands and expectations, such as the yearning for healthcare-related miracles of healthcare workers, instigated at times from the media, are barriers to medical altruism and motivation [
52]. Instead, encouragement of honest and open-minded dialogue between clinician and patients which may be challenging at times for both parties needs to occur, as opposed to dialogue rooted in dishonesties [
52]. Hence, it is paramount that we promote honesty, which could potentially result in an increased surge in medical altruism and motivation in healthcare workers. Health policymakers and stakeholders should recognise the integral role the community and society at large play in facilitating healthcare workers’ motivation as sources of reinforcement.
At the organizational and structural level, it is evident that greater attention to healthcare workers’ motivation is required [
40]. The top three motivating determinants at the organizational/structural level were training opportunities [
11,
17,
22,
29,
39,
41,
42,
48,
49], adequate monetary support suited for the living standards [
11,
17,
38,
39,
41,
49] and transformative leadership and supportive supervision [
31,
33,
34,
35,
37]. Similar to this review, a study in India reported that regular training was reported as a motivating factor in India [
53]. In Sweden, a study reported provision of remuneration as an important element of motivation, suggesting that monetary incentives be coupled with the quality of healthcare service delivery to patients [
55]. These findings show that health policymakers and managers should aim at creating both monetary and non-monetary motivational packages for the health workforce [
56].
Healthcare workers are motivated by transformative leaders who exhibit qualities such as idealised influence-behaviour, intellectual stimulation and inspirational motivation, not transactional or laissez-faire leaders [
31]. Similarly, a study in Sweden emphasised the role of positive management, including provision of clear direction, non-hierarchical collaboration, clear communication and systematic empowerment geared towards motivating the healthcare workers [
55]. In 2015, a study in Iran reported good and support manager and supervisors and having good working relations with co-workers being motivators of healthcare workers [
57]. This emphasises the importance of having a healthy organizational social environment to motivate healthcare workers, which can enhance by strengthening management capacities and cohesive organizational culture [
55,
57]. These strategies could potentially result in a more supportive organization environment and curb the organizational-related barriers to healthcare workers’ motivation reported in various studies.
Barriers to motivation reported in studies included lack of or inadequate monetary support, favouritism, critical shortage of skilled healthcare professionals leading to heavy workload, and unrealistic expectations from management and government. Likewise, in Iran, unfair treatment, lack of appreciation and poor management were reported as demotivating factors [
57], while in India heavy workload has been associated with job burnout [
53]. Accepting the informal payment from patients resulted in deterioration in the quality and access of healthcare service delivery and individually, feelings of being overwhelmed and guilty were experienced by healthcare workers [
48]. Therefore, it is essential to adequately compensate the health workforce to avoid compromising the universal access to healthcare, which is a right.
The health workforce shortage crisis has adverse effects on the health systems and highlights the significance of motivation in quality of healthcare delivery and health outcomes among the already present health workforce [
22,
48]. The perpetual health workforce shortage is caused by the higher trained cadres such as physicians and nurses moving from public to private sectors or rural to urban migration, or brain drain, thus leaving the lower cadre staff and few cadre staff with a heavier load, yet the majority of the training opportunities are offered to the higher cadre staff, not the auxiliary staff. In developing countries, optimising the lower-level cadres and auxiliary staff by increasing training opportunities [
1] to provide higher quality care from a knowledge- and skill-based stance will enhance health outcomes as a method of working around the shortage crisis.
Healthcare workers have suggested that increased support, receiving constructive feedback, fair treatment and teamwork that involves sharing the workload are strategies that will enhance their motivation to provide quality healthcare while creating a sense of belongingness [
11,
37]. Additionally, autonomy has been reported to be a motivating determinant among healthcare workers. A Brazilian study among female dentists reported that their motivation to choose dentistry was the relative flexibility of practising the profession and being considerate of the entire well-being of their patients [
58] whereas in Spain, doctors reported being intrinsically motivated and some financial controlling policies did weaken their intrinsic motivation [
59].
An Indian study reported non-financial motivators reportedly need more attention in order to increase motivation among healthcare workers [
53]. The findings of the studies in Spain [
59] and India [
48] are like the ones reported in this review. As much as both financial motivators are essential, non-motivators are equally important. Hence, redesigning flexible policies facilitating financial and non-financial motivation determinants among healthcare workers within health facilities and health sector at large need to be innovated and implemented.
Allowing the barriers to healthcare workers’ motivation to prevail results in their demotivation. Healthcare workers’ demotivation has an adverse ripple effect, from the reduced quality of care provided to poor patient outcomes, poor health outcomes and low performance at healthcare-worker, health-facility and health-system levels. Kok and colleagues stated that motivation is a critical determinant of performance [
37] and thus is paramount in the functionality of health systems.
Even in resource-limited settings, it is essential to note that money cannot solve all the hardships in the health system [
1], as much as it is a key facilitator. Therefore, non-monetary determinants of motivation identified can be used to create contextually relevant strategies to enhance the quality of healthcare services provision and strengthen health systems. Improvements and changes at the individual, organizational and societal levels are required based on the determinants of motivation and demotivation by the healthcare workers in the EAC health systems. This is vital to enhance the quality of care provided, health workforce strengthening [
10], health system strengthening [
8], achievement of Universal Health Coverage (UHC) [
60] and the success if Sustainable Development Goal 3 (SDG:3) on health for all at all ages [
61].
In the following recommendation section, stating the limitations of studies, possible considerations and solutions are geared towards enhancing health workforce motivation in the East African Community.
4.1. Limitations in Studies Reviewed
Limitations reported in the various studies include limited sample size [
18,
37,
46] and sample error related to the non-randomised techniques used to recruit participants such as convivence and purposive sampling [
31,
38,
40,
49]. Researchers stated that the limited sample size and related factors could potentially result in various biases, namely selection bias, social desirability bias, courtesy bias and response bias [
29,
30,
31,
36,
39,
40,
49]. Due to limited or small sample size, researchers were aware of the limitations surrounding the possibility of the findings not being statistically generalizable to all healthcare workers [
18,
19,
20,
29,
42,
48,
49]. However, due to similarities in the determinants reported among healthcare workers in multiple settings in the studies reviewed, the results should still be considered when creating informed strategies. Additionally cited limitations that may have affected the findings included the timing of the study [
39,
40], financial constraints [
36] and use of a single measure [
31].
4.2. Research Gaps and Recommendations for Further Research
Based on the limitations and gaps cited in the literature reviewed, researchers recommended possible solutions. Researchers recommend future studies should use large sample sizes [
22,
34], preferably more heterogeneous samples, including all cadres—both support and professional healthcare workers [
38]. For a broader picture, two studies recommended interviewing the healthcare workers who have left to know what would have motivated them to stay [
34,
41]. The need for more observational studies was identified due to the primarily subjective nature of most studies in this topic, as the majority were qualitative studies [
36]. More quantitative studies using varied psychometrically tested measures in multiple settings, especially in rural areas, are needed [
19,
20,
29,
30,
31]. The reason being tha the majority of the East African populations in all the six countries reside in the rural areas and are in more need of healthcare.
Future studies should consider doing more correlational or causal studies on the relationship between the level of motivation and demographic factors [
41], perceived performance [
19] and effect of interventions on motivation [
32,
37]. More randomised studies are also needed to increase the possibility of generalisability of results; however, researchers also emphasis realistic, comprehensive approaches need to be taken when doing research and creating policies on this topic [
22]. Additional studies in private health facilities would be essential for comprehensive and insightful analysis of determinants of healthcare workers’ motivation [
29]. This is because the national health system includes both private and public healthcare facilities and workers.
A critical shortage of healthcare workers has been cited as a major challenge in the EAC, resulting in adverse ripple effects in the national health systems. Therefore, it is vital that we health policymakers, managers and ministries of health begin to recognise the importance of the already-present healthcare workers. Optimisation of the present health workforce will help improve the quality of healthcare delivery and strengthen health systems. Holistic programs [
62] and context-specific training and supportive supervision of healthcare workers, especially the ones in lower cadres, are essential for the above to be achieved. The reason being that, in majority of Sub-Saharan health systems, lower-cadre and auxiliary healthcare workers are the majority compared to higher-cadre staff and are more likely to stay in the health system [
1]. Therefore, as proven in this review, the desire for lower-cadre and auxiliary staff to be trained is high. The Ministries of Health in all the EAC member states should recognise this as an opportunity to work around the shortage of healthcare workers. Through empowering, training, rewarding and better remunerating the lower cadre staff for the work they already do due to the shortage, their motivation to remain in the health system and provide higher quality healthcare will prevail [
11].
More studies regarding healthcare workers’ motivation in the EAC are needed to bridge knowledge gaps, some of which have been identified in this review. More literature has the potential of resulting in creation of tactically significant policies. Health-sector authorities should consider the inclusion of healthcare workers as stakeholders, decision-makers and policymakers in the strategic development and implementation initiatives [
56]. This could result in more effective and relevant strategies, monitoring and evaluating of trends among healthcare workers [
56]. These policies can facilitate health policymakers and implementers in the six EAC member states in decision-making processes regarding healthcare workers’ motivation and inform health-workforce-strengthening strategies.





{kind=link}
{kind=link}