Maternal Health and Green Spaces in China: A Longitudinal Analysis of MMR Based on Spatial Panel Model


Abstract
:1. Introduction
2. Materials and Methods
2.1. Variables and Data Source
2.2. Methods
3. Results
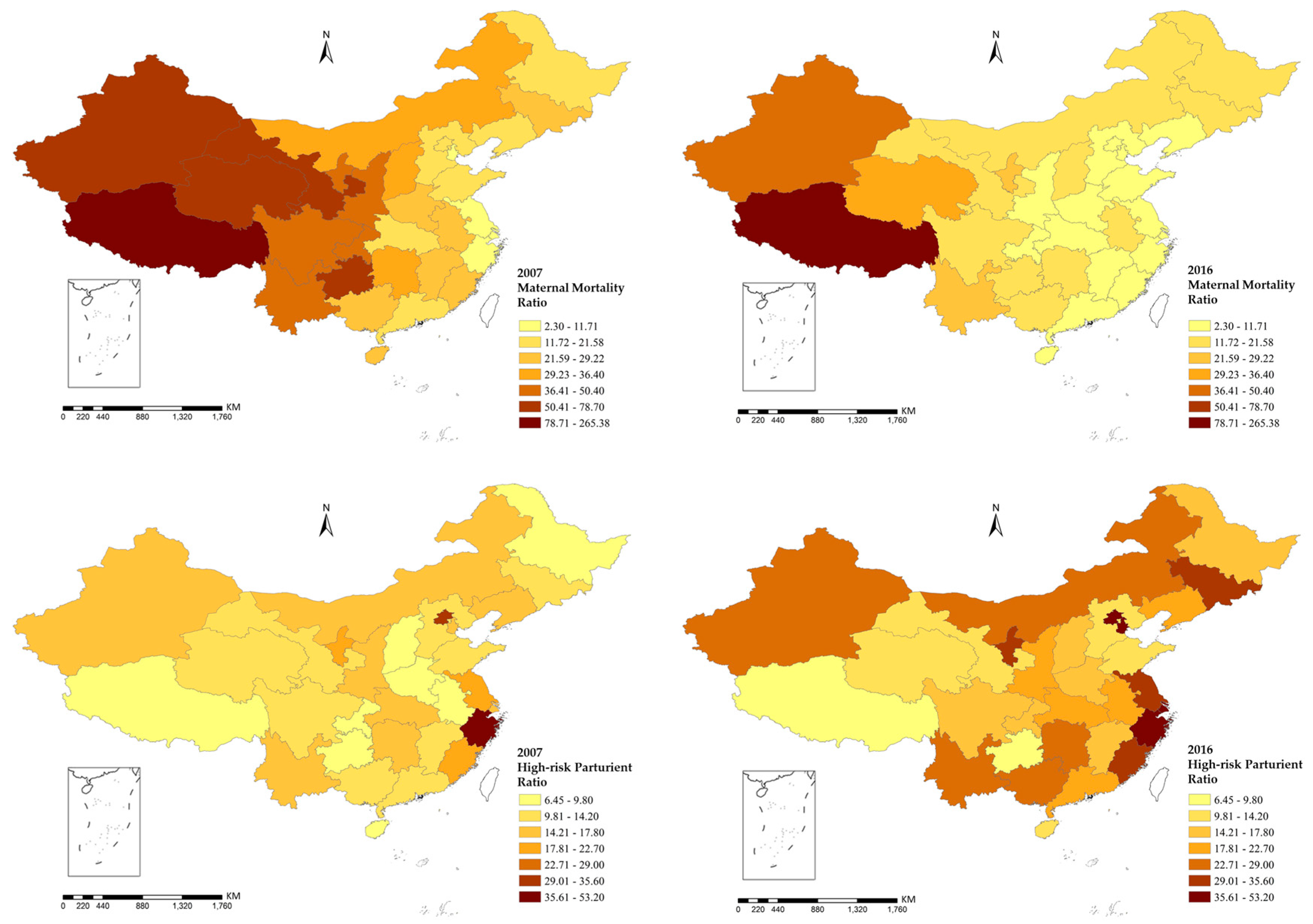
3.1. Description Analysis
3.2. Global Moran’s I Statistics
3.3. Panel Data Model
3.4. Spatial Panel Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Beaglehole, R.; Bonita, R. Global public health: A scorecard. Lancet 2008, 372, 1988–1996. [Google Scholar] [CrossRef]
- Singh, K.; Story, W.T.; Moran, A.C. Assessing the continuum of care pathway for maternal health in South Asia and sub-Saharan Africa. Matern. Child Health J. 2016, 20, 281–289. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.; Creanga, A.A.; Gillespie, D.G.; Tsui, A.O. Economic status, education and empowerment: Implications for maternal health service utilization in developing countries. PLoS ONE 2010, 5, e11190. [Google Scholar] [CrossRef] [PubMed]
- Feng, X.L.; Zhu, J.; Zhang, L.; Song, L.; Hipgrave, D.; Guo, S.; Ronsmans, C.; Guo, Y.; Yang, Q. Socio-economic disparities in maternal mortality in China between 1996 and 2006. BJOG Int. J. Obstet. Gynecol. 2010, 117, 1527–1536. [Google Scholar] [CrossRef]
- Liang, J.; Li, X.; Kang, C.; Wang, Y.; Kulikoff, X.R.; Coates, M.M.; Ng, M.; Luo, S.; Mu, Y.; Wang, X.; et al. Maternal mortality ratios in 2852 Chinese counties, 1996–2015, and achievement of Millennium Development Goal 5 in China: A subnational analysis of the Global Burden of Disease Study 2016. Lancet 2019, 393, 241–252. [Google Scholar] [CrossRef]
- Huang, Y.; Shallcross, D.; Pi, L.; Tian, F.; Pan, J.; Ronsmans, C. Ethnicity and maternal and child health outcomes and service coverage in western China: A systematic review and meta-analysis. Lancet Glob. Health 2018, 6, e39–e56. [Google Scholar] [CrossRef]
- Liang, J.; Zhu, J.; Dai, L.; Li, X.; Li, M.; Wang, Y. Maternal mortality in China, 1996–2005. Int. J. Obstet. Gynecol. 2010, 110, 93–96. [Google Scholar] [CrossRef]
- Li, Y.; Zhang, Y.; Fang, S.; Liu, S.; Liu, X.; Li, M.; Liang, H.; Fu, H. Analysis of inequality in maternal and child health outcomes and mortality from 2000 to 2013 in China. Int. J. Equity Health 2017, 16, 66. [Google Scholar] [CrossRef]
- Dadvand, P.; Wright, J.; Martinez, D.; Basagaña, X.; Mceachan, R.R.; Cirach, M.; Gidlow, C.J.; De, H.K.; Gražulevičienė, R.; Nieuwenhuijsen, M.J. Inequality, green spaces, and pregnant women: Roles of ethnicity and individual and neighbourhood socioeconomic status. Environ. Int. 2014, 71, 101–108. [Google Scholar] [CrossRef]
- Morellofrosch, R.; Shenassa, E.D. The environmental “riskscape” and social inequality: Implicationsfor explaining maternal and child health disparities. Environ. Health Perspect. 2006, 114, 1150–1153. [Google Scholar] [CrossRef]
- Timmermans, S.; Bonsel, G.J.; Steegers-Theunissen, R.P.M.; Mackenbach, J.P.; Steyerberg, E.W.; Raat, H.; Verbrugh, H.A.; Tiemeier, H.W.; Hofman, A.; Birnie, E.; et al. Individual accumulation of heterogeneous risks explains perinatal inequalities within deprived neighbourhoods. Eur. J. Epidemiol. 2011, 26, 165–180. [Google Scholar] [CrossRef] [PubMed]
- Izugbara, C.O.; Ngilangwa, D.P. Women, poverty and adverse maternal outcomes in Nairobi, Kenya. BMC Women’s Health 2010, 10, 33. [Google Scholar] [CrossRef] [PubMed]
- Dadvand, P.; Nazelle, A.D.; Figueras, F.; Basagaña, X.; Su, J.; Amoly, E.; Jerrett, M.; Vrijheid, M.; Sunyer, J.; Nieuwenhuijsen, M.J. Green space, health inequality and pregnancy. Environ. Int. 2012, 40, 110–115. [Google Scholar] [CrossRef] [PubMed]
- James, P.; Banay, R.F.; Hart, J.E.; Laden, F. A review of the health benefits of greenness. Curr. Epidemiol. Rep. 2015, 2, 131–142. [Google Scholar] [CrossRef]
- Both, M.I.; Overvest, M.A.; Wildhagen, M.F.; Golding, J.; Wildschut, H.I.J. The association of daily physical activity and birth outcome: A population-based cohort study. Eur. J. Epidemiol. 2010, 25, 421–429. [Google Scholar] [CrossRef]
- Hegaard, H.K.; Pedersen, B.K.; Birgitte Bruun, N.; Peter, D. Leisure time physical activity during pregnancy and impact on gestational diabetes mellitus, pre-eclampsia, preterm delivery and birth weight: A review. Acta Obstet. Gynecol. Scand. 2011, 86, 1290–1296. [Google Scholar] [CrossRef]
- Hjortebjerg, D.; Andersen, A.M.N.; Ketzel, M.; Pedersen, M.; Raaschou-Nielsen, O.; Sørensen, M. Associations between maternal exposure to air pollution and traffic noise and newborn’s size at birth: A cohort study. Environ. Int. 2016, 95, 1–7. [Google Scholar] [CrossRef]
- Kingsley, S.L.; Eliot, M.N.; Whitsel, E.A.; Huang, Y.-T.; Kelsey, K.T.; Marsit, C.J.; Wellenius, G.A. Maternal residential proximity to major roadways, birth weight, and placental DNA methylation. Environ. Int. 2016, 92–93, 43–49. [Google Scholar] [CrossRef]
- Rondó, P.H.C.; Ferreira, R.F.; Nogueira, F.; Ribeiro, M.C.N.; Lobert, H.; Artes, R. Maternal psychological stress and distress as predictors of low birth weight, prematurity and intrauterine growth retardation. Eur. J. Clin. Nutr. 2003, 57, 266–272. [Google Scholar] [CrossRef]
- Grote, N.K.; Bridge, J.A.; Gavin, A.R.; Melville, J.L.; Satish, I.; Katon, W.J. A meta-analysis of depression during pregnancy and the risk of preterm birth, low birth weight, and intrauterine growth restriction. Arch. Gen. Psychiatry 2010, 67, 1012. [Google Scholar] [CrossRef]
- Gill, S.E.; Handley, J.F.; Ennos, A.R.; Pauleit, S. Adapting cities for climate change: The role of the green infrastructure. Built Environ. 2007, 33, 115–133. [Google Scholar] [CrossRef]
- Scotland, H. Guide to HIA of Greenspace (Greenspace, Scotland). Available online: http://cloud.snappages.com/803c0945dd99f78b94cef59b278fec5244df7b24/HIA%20of%20greenspace%20a%20guide%20-%20GS%20HS%20SNH%20IOM%20Scotland%20-%202008.pdf (accessed on 28 November 2019).
- Lawton, E.; Brymer, E.; Clough, P.; Denovan, A. The relationship between the physical activity environment, nature relatedness, anxiety, and the psychological well-being benefits of regular exercisers. Front. Psychol. 2017, 8, 1058. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.C.; Maheswaran, R. The health benefits of urban green spaces: A review of the evidence. J. Public Health 2011, 33, 212–222. [Google Scholar] [CrossRef] [PubMed]
- Maas, J.; van Dillen, S.M.; Verheij, R.A.; Groenewegen, P.P. Social contacts as a possible mechanism behind the relation between green space and health. Health Place 2009, 15, 586–595. [Google Scholar] [CrossRef]
- Maas, J.; Verheij, R.A.; de Vries, S.; Spreeuwenberg, P.; Schellevis, F.G.; Groenewegen, P.P. Morbidity is related to a green living environment. J. Epidemiol. Community Health 2009, 63, 967–973. [Google Scholar] [CrossRef]
- Nowak, D.J.; Crane, D.E.; Stevens, J.C. Air pollution removal by urban trees and shrubs in the United States. Urban For. Urban Green. 2006, 4, 115–123. [Google Scholar] [CrossRef]
- Whitford, V.; Ennos, A.R.; Handley, J.F. “City form and natural process”—Indicators for the ecological performance of urban areas and their application to Merseyside, UK. Landsc. Urban Plan. 2001, 57, 91–103. [Google Scholar] [CrossRef]
- Martine, V.; David, M.; Sandra, M.; Payam, D.; Anna, S.; Judith, R.; Mark, N. Ambient air pollution and risk of congenital anomalies: A systematic review and meta-analysis. Environ. Health Perspect. 2011, 119, 598–606. [Google Scholar]
- Sapkota, A.; Chelikowsky, A.P.; Nachman, K.E.; Cohen, A.J.; Ritz, B. Exposure to particulate matter and adverse birth outcomes: A comprehensive review and meta-analysis. Air Qual. Atmos. Health 2012, 5, 369–381. [Google Scholar] [CrossRef]
- Rupa, B.; Brian, M.; Bart, O. High ambient temperature and the risk of preterm delivery. Am. J. Epidemiol. 2010, 172, 1108. [Google Scholar]
- Wolch, J.R.; Byrne, J.; Newell, J.P. Urban green space, public health, and environmental justice: The challenge of making cities ‘just green enough’. Landsc. Urban Plan. 2014, 125, 234–244. [Google Scholar] [CrossRef]
- Banay, R.F.; Bezold, C.P.; James, P.; Hart, J.E.; Laden, F. Residential greenness: Current perspectives on its impact on maternal health and pregnancy outcomes. Int. J. Women’s Health 2017, 9, 133–144. [Google Scholar] [CrossRef]
- Payam, D.; Jordi, S.; Xavier, B.A.; Ferran, B.; Aitana, L.; Ana, F.S.; Marisa, E.; Raquel, G.E.; Mendez, M.A.; Nieuwenhuijsen, M.J. Surrounding greenness and pregnancy outcomes in four Spanish birth cohorts. Environ. Health Perspect. 2012, 120, 1481–1487. [Google Scholar]
- Casey, J.A.; James, P.; Rudolph, K.E.; Wu, C.D.; Schwartz, B.S. Greenness and birth outcomes in a range of Pennsylvania communities. Int. J. Environ. Res. Public Health 2016, 13, 311. [Google Scholar] [CrossRef]
- China Health Statistics Yearbook, 2007–2016. Available online: http://data.cnki.net/yearbook/Single/N2019030282 (accessed on 15 June 2018).
- China Statistics Yearbook, 2007–2016. Available online: http://data.cnki.net/yearbook/Single/N2019110002 (accessed on 15 June 2018).
- Liu, L.; Zhong, Y.; Ao, S.; Wu, H. Exploring the relevance of green space and epidemic diseases based on panel data in China from 2007 to 2016. Int. J. Environ. Res. Public Health 2019, 16, 2551. [Google Scholar] [CrossRef] [Green Version]
- Véronique, F.; Carine, R.; Campbell, O.M.R.; Graham, W.J.; Anne, M.; Jo, B.; Marjorie, K.; David, O. Maternal health in poor countries: The broader context and a call for action. Lancet 2006, 368, 1535–1541. [Google Scholar]
- Tunçalp, Ö.; Souza, J.P.; Hindin, M.J.; Santos, C.A.; Oliveira, T.H.; Vogel, J.P.; Togoobaatar, G.; Ha, D.Q.; Say, L.; Gülmezoglu, A.M.; et al. Education and severe maternal outcomes in developing countries: A multicountry cross-sectional survey. BJOG Int. J. Obstet. Gynecol. 2014, 121, 57–65. [Google Scholar] [CrossRef] [Green Version]
- Marmot, M. Social determinants of health inequalities. Lancet 2012, 51, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Levy, L.; Herzog, A.N. Effects of population density and crowding on health on health and social adapation in the Netherlands. J. Health Soc. Behav. 1974, 15, 228–240. [Google Scholar] [CrossRef]
- Gage, A.J. Barriers to the utilization of maternal health care in rural Mali. Soc. Sci. Med. 2007, 65, 1666–1682. [Google Scholar] [CrossRef]
- Cao, Q.; Liang, Y.; Niu, X. China’s air quality and respiratory disease mortality based on the spatial panel model. Int. J. Environ. Res. Public Health 2017, 14, 1081. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hystad, P.; Davies, H.W.; Frank, L.; Van Loon, J.; Gehring, U.; Tamburic, L.; Brauer, M. Residential greenness and birth outcomes: Evaluating the influence of spatially correlated built-environment factors. Environ. Health Perspect. 2014, 122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grazuleviciene, R.; Danileviciute, A.; Dedele, A.; Vencloviene, J.; Andrusaityte, S.; Uždanaviciute, I.; Nieuwenhuijsen, M.J. Surrounding greenness, proximity to city parks and pregnancy outcomes in Kaunas cohort study. Int. J. Hyg. Environ. Health 2015, 218, 358–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davey, G. Happiness and quality of life in the people’s republic of China. In Happiness across Cultures; Springer: Dordrecht, The Netherlands, 2012. [Google Scholar] [CrossRef]
- Harpham, T. Urbanization and mental health in developing countries: A research role for social scientists, public health professionals and social psychiatrists. Soc. Sci. Med. 1994, 39, 233–245. [Google Scholar] [CrossRef]
- Moore, M.; Gould, P.; Keary, B.S. Global urbanization and impact on health. Int. J. Hyg. Environ. Health 2003, 206, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Fuller, R.A.; Gaston, K.J. The scaling of green space coverage in European cities. Biol. Lett. 2009, 5, 352. [Google Scholar] [CrossRef] [Green Version]
- Smith, M.P.; Guarnizo, L.E. Global mobility, shifting borders and urban citizenship. J. Econ. Soc. Geogr. 2010, 100, 610–622. [Google Scholar] [CrossRef]
- Bowler, D.E.; Buyung-Ali, L.M.; Knight, T.M.; Pullin, A.S. A systematic review of evidence for the added benefits to health of exposure to natural environments. BMC Public Health 2010, 10, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Maas, J.; Verheij, R.A.; Groenewegen, P.P.; de Vries, S.; Spreeuwenberg, P. Green space, urbanity, and health: How strong is the relation? J. Epidemiol. Community Health 2006, 60, 587–592. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | |
|---|---|---|---|---|---|---|---|---|---|---|
| MMR (1 death/100,000 livebirth) | ||||||||||
| Min. | 7.86 | 6.57 | 5.20 | 3.60 | 1.20 | 1.40 | 1.90 | 1.90 | 1.90 | 2.30 |
| Mean | 39.87 | 32.11 | 28.84 | 25.81 | 22.15 | 20.66 | 19.78 | 17.72 | 17.72 | 16.32 |
| Max. | 265.38 | 233.96 | 232.20 | 174.80 | 180.70 | 176.10 | 154.50 | 108.90 | 108.90 | 100.90 |
| HPR (1 death/100,000 livebirth) | ||||||||||
| Min. | 6.45 | 6.47 | 6.50 | 7.20 | 5.90 | 7.60 | 8.70 | 8.50 | 8.50 | 8.70 |
| Mean | 14.28 | 16.20 | 17.26 | 18.17 | 18.61 | 19.43 | 20.77 | 22.39 | 22.39 | 24.68 |
| Max. | 38.30 | 41.19 | 41.90 | 42.60 | 42.50 | 44.00 | 46.40 | 46.90 | 46.90 | 53.20 |
| Area of Green Space (100 km2) | ||||||||||
| Min. | 0.20 | 0.20 | 0.22 | 0.21 | 0.29 | 0.34 | 0.36 | 0.42 | 0.53 | 0.62 |
| Mean | 5.56 | 5.69 | 6.43 | 6.89 | 7.24 | 7.64 | 7.83 | 8.15 | 8.61 | 8.99 |
| Max. | 27.47 | 37.70 | 40.16 | 42.04 | 41.06 | 40.17 | 41.20 | 42.19 | 43.84 | 45.27 |
| Area of Public Green Space (100 km2) | ||||||||||
| Min. | 0.02 | 0.03 | 0.04 | 0.03 | 0.05 | 0.05 | 0.06 | 0.07 | 0.09 | 0.09 |
| Mean | 1.09 | 1.18 | 1.30 | 1.42 | 1.56 | 1.67 | 1.77 | 1.86 | 1.98 | 2.11 |
| Max. | 4.76 | 5.02 | 5.32 | 5.85 | 6.80 | 7.40 | 7.89 | 8.32 | 8.96 | 9.75 |
| Green Space Coverage Ratio (%) | ||||||||||
| Min. | 24.10 | 25.10 | 27.30 | 16.00 | 24.10 | 30.00 | 18.10 | 30.80 | 29.80 | 31.10 |
| Mean | 34.18 | 35.32 | 36.70 | 36.33 | 37.75 | 38.46 | 38.13 | 39.34 | 39.11 | 39.17 |
| Max. | 42.80 | 42.60 | 47.70 | 46.60 | 46.80 | 46.20 | 47.10 | 49.10 | 48.40 | 48.40 |
| Urbanization rate (%) | ||||||||||
| Min. | 0.21 | 0.22 | 0.22 | 0.23 | 0.23 | 0.23 | 0.24 | 0.26 | 0.28 | 0.30 |
| Mean | 0.47 | 0.48 | 0.49 | 0.51 | 0.52 | 0.53 | 0.54 | 0.56 | 0.57 | 0.58 |
| Max. | 0.89 | 0.89 | 0.89 | 0.89 | 0.89 | 0.89 | 0.90 | 0.90 | 0.88 | 0.88 |
| Health worker (10,000 persons) | ||||||||||
| Min. | 1.02 | 1.17 | 1.60 | 1.67 | 2.22 | 2.16 | 2.47 | 2.65 | 2.91 | 2.92 |
| Mean | 19.06 | 19.90 | 25.10 | 26.44 | 27.76 | 29.38 | 31.55 | 32.98 | 34.46 | 36.01 |
| Max. | 45.21 | 47.98 | 60.21 | 64.59 | 68.96 | 73.89 | 81.93 | 83.85 | 85.57 | 87.41 |
| Year | Maternal Mortality Ratio (MMR) | High-Risk Parturient Ratio (HPR) | ||||
|---|---|---|---|---|---|---|
| Moran’s I | p | Z | Moran’s I | p | Z | |
| 2007 | 0.162 | <0.001 | 3.552 | −0.064 | 0.678 | −0.415 |
| 2010 | 0.130 | <0.001 | 3.166 | 0.027 | 0.939 | 0.007 |
| 2013 | 0.122 | <0.001 | 3.23 | 0.012 | 0.56 | 0.584 |
| 2016 | 0.114 | <0.001 | 3.209 | 0.032 | 0.402 | 0.838 |
| Variables | Pooled OLS | Fixed Effects | Random Effects |
|---|---|---|---|
| HPR | −0.145 | 0.828 *** | 0.516 ** |
| Mediworker | −5.689 | −37.711 *** | −10.38 |
| GDP | 9.020 * | 0.929 | 0.373 |
| PopDen | −5.603 ** | 5.733 | 0.384 |
| GS | 16.021 * | −16.624 * | −4.442 |
| Public GS | −42.580 *** | −60.312 *** | −46.133 *** |
| Gscoverage | −0.774 * | −0.418 * | −0.747 *** |
| Urban R | −66.523 ** | 184.193 *** | −2.629 |
| R2 | 0.618 | 0.579 | 0.502 |
| Adjusted R2 | 0.608 | 0.52 | 0.489 |
| F Statistic | 60.984 *** (df = 8; 301) | 46.595 *** (df = 8; 271) | 303.620 *** |
| Variables | SDM | SLM | SEM | |||
|---|---|---|---|---|---|---|
| Coef. | p | Coef. | p | Coef. | p | |
| HPR | 0.087381 | 0.645 | 0.82245 | <0.001 *** | 0.82801 | <0.001 *** |
| Mediworker | −10.8043 | 0.024 * | −37.9481 | <0.001 *** | −37.4303 | <0.001 *** |
| GDP | −1.91947 | 0.201 | 0.886 | 0.697 | 0.9084 | 0.68903 |
| PopDen | −2.6407 | 0.333 | 5.71223 | 0.179 | 5.66942 | 0.18136 |
| GS | −2.75892 | 0.688 | −16.841 | <0.05 * | −16.891 | <0.05 * |
| Public GS | −10.1467 | 0.362 | −60.0729 | <0.001 *** | −60.4161 | <0.001 *** |
| Gscoverage | −0.26285 | 0.021 * | −0.42238 | <0.05 * | −0.42398 | <0.05 * |
| Urban R | −73.6624 | 0.004 ** | 183.3074 | <0.001 *** | 184.0643 | <0.001 *** |
| 0.955045 | <0.001 *** | |||||
| 0.065648 | 0.3925 | −0.016712 | 0.8125 | |||
| λ | −0.016370 | 0.8378 | ||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jin, P.; Gao, Y.; Liu, L.; Peng, Z.; Wu, H. Maternal Health and Green Spaces in China: A Longitudinal Analysis of MMR Based on Spatial Panel Model. Healthcare 2019, 7, 154. https://doi.org/10.3390/healthcare7040154
Jin P, Gao Y, Liu L, Peng Z, Wu H. Maternal Health and Green Spaces in China: A Longitudinal Analysis of MMR Based on Spatial Panel Model. Healthcare. 2019; 7(4):154. https://doi.org/10.3390/healthcare7040154
Chicago/Turabian StyleJin, Ping, Yushu Gao, Lingbo Liu, Zhenghong Peng, and Hao Wu. 2019. "Maternal Health and Green Spaces in China: A Longitudinal Analysis of MMR Based on Spatial Panel Model" Healthcare 7, no. 4: 154. https://doi.org/10.3390/healthcare7040154