Assessment of the Impact of Deformable Registration of Diagnostic MRI to Planning CT on GTV Delineation for Radiotherapy for Oropharyngeal Carcinoma in Routine Clinical Practice


Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Image Acquisition
2.2.1. MRI
2.2.2. CT
2.3. Deformable MRI–CT Image Registration
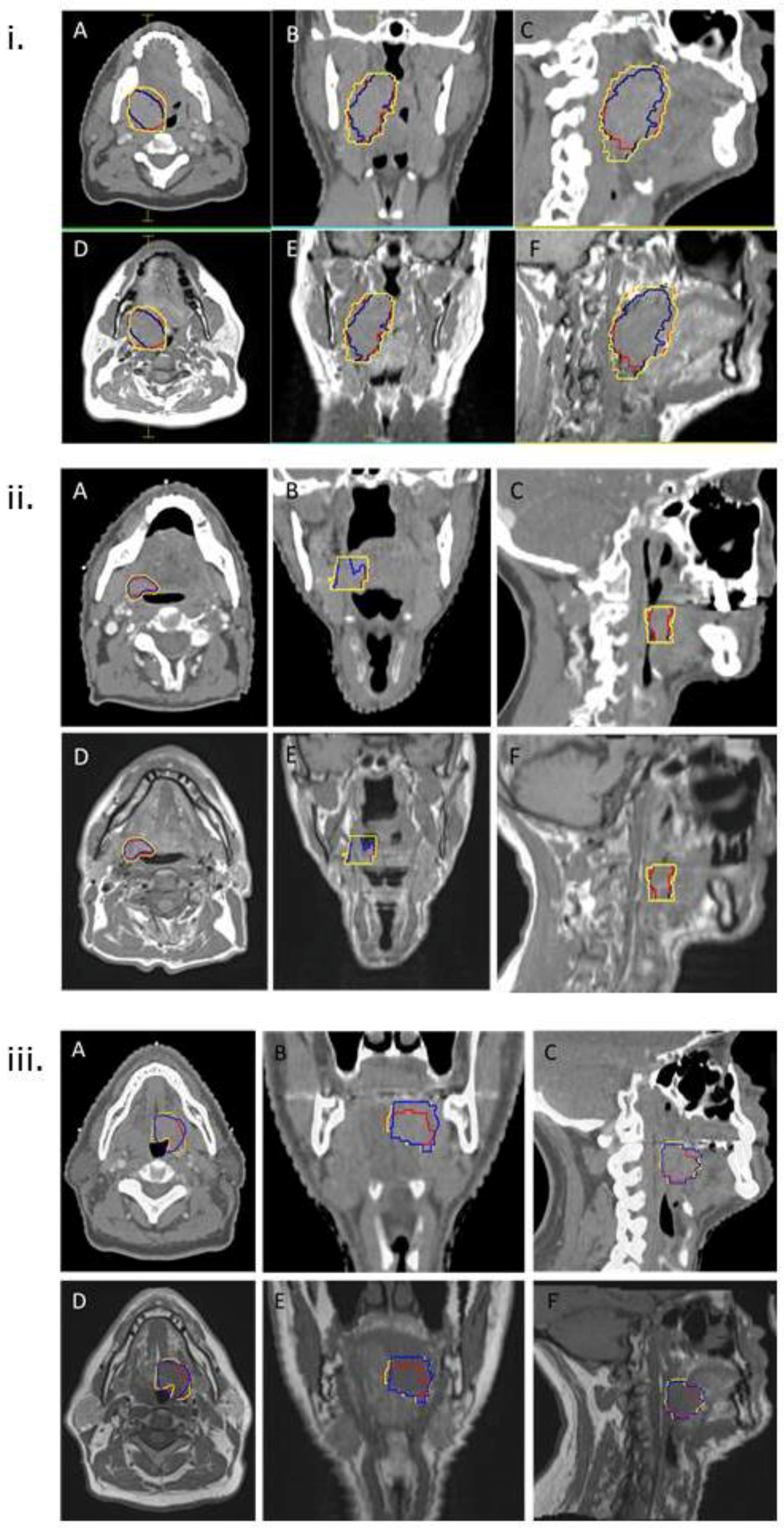
2.4. GTV Delineation
2.5. Analysis of GTVs
2.5.1. Conformity Index (CI)
2.5.2. Mean Distance to Conformity (MDC)
2.5.3. Dice Similarity Coefficient (DSC)
2.5.4. Centre of Gravity Distance (CGD)
2.5.5. Volumetric Analysis
2.6. Statistical Analysis
3. Results
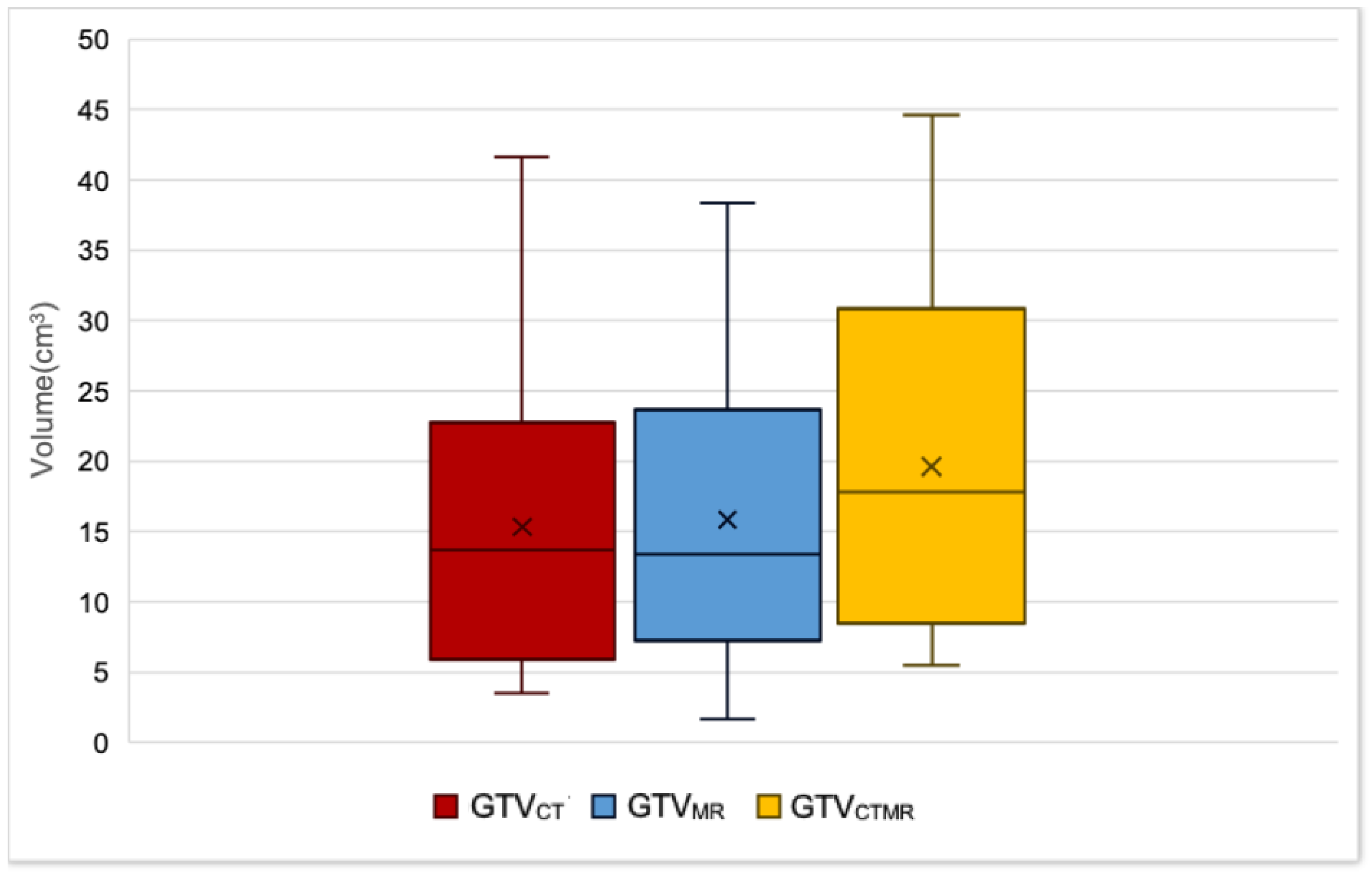
3.1. Comparison of GTV Volumes
3.2. Comparison of Positional Metrics
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Eisbruch, A.; Marsh, L.H.; Dawson, L.A.; Bradford, C.R.; Teknos, T.N.; Chepeha, D.B.; Worden, F.P.; Urba, S.; Lin, A.; Schipper, M.J.; et al. Recurrences near base of skull after IMRT for head-and-neck cancer: Implications for target delineation in high neck and for parotid gland sparing. Int. J. Radiat. Oncol. Biol. Phys. 2004, 59, 28–42. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.M.; Farwell, D.G.; Luu, Q.; Chen, L.M.; Vijayakumar, S.; Purdy, J.A. Marginal misses after postoperative intensity-modulated radiotherapy for head and neck cancer. Int. J. Radiat. Oncol. Biol. Phys. 2011, 80, 1423–1429. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.M.; Chin, R.; Beron, P.; Yoshizaki, T.; Mikaeilian, A.G.; Cao, M. Inadequate target volume delineation and local-regional recurrence after intensity-modulated radiotherapy for human papillomavirus-positive oropharynx cancer. Radiother. Oncol. 2017, 123, 412–418. [Google Scholar] [CrossRef] [PubMed]
- Njeh, C.F. Tumor delineation: The weakest link in the search for accuracy in radiotherapy. J. Med. Phys. 2008, 33, 136–140. [Google Scholar] [CrossRef] [PubMed]
- Weiss, E.; Hess, C.F. The impact of gross tumor volume (GTV) and clinical target volume (CTV) definition on the total accuracy in radiotherapy theoretical aspects and practical experiences. Strahlenther. Onkol. 2003, 179, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Rasch, C.; Steenbakkers, R.; van Herk, M. Target definition in prostate, head, and neck. Semin. Radiat. Oncol. 2005, 15, 136–145. [Google Scholar] [CrossRef] [PubMed]
- Grégoire, V.; Evans, M.; Le, Q.T.; Bourhis, J.; Budach, V.; Chen, A.; Eisbruch, A.; Feng, M.; Giralt, J.; Gupta, T.; et al. Delineation of the primary tumour Clinical Target Volumes (CTV-p) in laryngeal, hypopharyngeal, oropharyngeal and oral cavity squamous cell carcinoma: AIRO, CACA, DAHANCA, EORTC, GEORCC, GORTEC, HKNPCSG, HNCIG, IAG-KHT, LPRHHT, NCIC CTG, NCRI, NRG Oncology, PHNS, SBRT, SOMERA, SRO, SSHNO, TROG consensus guidelines. Radiother. Oncol. 2018, 126, 3–24. [Google Scholar] [PubMed]
- Battista, J.J.; Rider, W.D.; Van Dyk, J. Computed tomography for radiotherapy planning. Int. J. Radiat. Oncol. Biol. Phys. 1980, 6, 99–107. [Google Scholar] [CrossRef]
- Ahmed, M.; Schmidt, M.; Sohaib, A.; Kong, C.; Burke, K.; Richardson, C.; Usher, M.; Brennan, S.; Riddell, A.; Davies, M.; et al. The value of magnetic resonance imaging in target volume delineation of base of tongue tumours—A study using flexible surface coils. Radiother. Oncol. 2010, 94, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Bird, D.; Scarsbrook, A.F.; Sykes, J.; Ramasamy, S.; Subesinghe, M.; Carey, B.; Wilson, D.J.; Roberts, N.; McDermott, G.; Karakaya, E.; et al. Multimodality imaging with CT, MR and FDG-PET for radiotherapy target volume delineation in oropharyngeal squamous cell carcinoma. BMC Cancer 2015, 15, 844. [Google Scholar] [CrossRef] [PubMed]
- Chuter, R.; Prestwich, R.; Bird, D.; Scarsbrook, A.; Sykes, J.; Wilson, D.; Speight, R. The use of deformable image registration to integrate diagnostic MRI into the radiotherapy planning pathway for head and neck cancer. Radiother. Oncol. 2017, 122, 229–235. [Google Scholar] [CrossRef] [PubMed]
- Prestwich, R.J.; Sykes, J.; Carey, B.; Sen, M.; Dyker, K.E.; Scarsbrook, A.F. Improving target definition for head and neck radiotherapy: A place for magnetic resonance imaging and 18-fluoride fluorodeoxyglucose positron emission tomography? Clin. Oncol. 2012, 24, 577–589. [Google Scholar] [CrossRef] [PubMed]
- Webster, G.J.; Kilgallon, J.E.; Ho, K.F.; Rowbottom, C.G.; Slevin, N.J.; Mackay, R.I. A novel imaging technique for fusion of high-quality immobilised MR images of the head and neck with CT scans for radiotherapy target delineation. Br. J. Radiol. 2009, 82, 497–503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmed, M.; Hansen, V.N.; Harrington, K.J.; Nutting, C.M. Reducing the risk of xerostomia and mandibular osteoradionecrosis: The potential benefits of intensity modulated radiotherapy in advanced oral cavity carcinoma. Med. Dosim. 2009, 34, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Brunt, J.N. Computed tomography-magnetic resonance image registration in radiotherapy treatment planning. Clin. Oncol. 2010, 22, 688–697. [Google Scholar] [CrossRef] [PubMed]
- Hanvey, S.; McJury, M.; Tho, L.M.; Glegg, M.; Thomson, M.; Grose, D.; James, A.; Rizwanullah, M.; Paterson, C.; Foster, J. The influence of MRI scan position on patients with oropharyngeal cancer undergoing radical radiotherapy. Radiat. Oncol. 2013, 8, 129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jena, R.; Kirkby, N.F.; Burton, K.E.; Hoole, A.C.; Tan, L.T.; Burnet, N.G. A novel algorithm for the morphometric assessment of radiotherapy treatment planning volumes. Br. J. Radiol. 2010, 83, 44–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dice, L.R. Measures of the amount of ecologic association between species. Ecology 1945, 26, 297–302. [Google Scholar] [CrossRef]
- Prestwich, R.J.; Subesinghe, M.; Gilbert, A.; Chowdhury, F.U.; Sen, M.; Scarsbrook, A.F. Delayed response assessment with FDG-PET-CT following (chemo) radiotherapy for locally advanced head and neck squamous cell carcinoma. Clin. Radiol. 2012, 67, 966–975. [Google Scholar] [CrossRef] [PubMed]
- Cooper, J.S.; Mukherji, S.K.; Toledano, A.Y.; Beldon, C.; Schmalfuss, I.M.; Amdur, R.; Sailer, S.; Loevner, L.A.; Kousouboris, P.; Ang, K.K.; et al. An evaluation of the variability of tumor-shape definition derived by experienced observers from CT images of supraglottic carcinomas (ACRIN protocol 6658). Int. J. Radiat. Oncol. Biol. Phys. 2007, 67, 972–975. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dirix, P.; Haustermans, K.; Vandecaveye, V. The value of magnetic resonance imaging for radiotherapy planning. Semin. Radiat. Oncol. 2014, 24, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Daisne, J.F.; Duprez, T.; Weynand, B.; Lonneux, M.; Hamoir, M.; Reychler, H.; Grégoire, V. Tumor volume in pharyngolaryngeal squamous cell carcinoma: Comparison at CT, MR imaging, and FDG PET and validation with surgical specimen. Radiology 2004, 233, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Geets, X.; Tomsej, M.; Lee, J.A.; Duprez, T.; Coche, E.; Cosnard, G.; Lonneux, M.; Grégoire, V. Adaptive biological image-guided IMRT with anatomic and functional imaging in pharyngo-laryngeal tumors: Impact on target volume delineation and dose distribution using helical tomotherapy. Radiother. Oncol. 2007, 85, 105–115. [Google Scholar] [CrossRef] [PubMed]
- Seitz, O.; Chambron-Pinho, N.; Middendorp, M.; Sader, R.; Mack, M.; Vogl, T.J.; Bisdas, S. 18F-Fluorodeoxyglucose-PET/CT to evaluate tumor, nodal disease, and gross tumor volume of oropharyngeal and oral cavity cancer: Comparison with MR imaging and validation with surgical specimen. Neuroradiology 2009, 51, 677–686. [Google Scholar] [CrossRef] [PubMed]
- Rasch, C.; Keus, R.; Pameijer, F.A.; Koops, W.; Muller, S.; Touw, A.; Bartelink, H.; Lebesque, J.V. The potential impact of CT-MRI matching on tumor volume delineation in advanced head and neck cancer. Int. J. Radiat. Oncol. Biol. Phys. 1997, 39, 841–848. [Google Scholar] [CrossRef] [Green Version]
- Chung, N.N.; Ting, L.L.; Hsu, W.C.; Lui, L.T.; Wang, P.M. Impact of magnetic resonance imaging versus CT on nasopharyngeal carcinoma: Primary tumor target delineation for radiotherapy. Head Neck 2004, 26, 241–246. [Google Scholar] [CrossRef] [PubMed]
- Caldas-Magalhaes, J.; Kasperts, N.; Kooij, N.; van den Berg, C.A.; Terhaard, C.H.; Raaijmakers, C.P.; Philippens, M.E. Validation of imaging with pathology in laryngeal cancer: Accuracy of the registration methodology. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, e289–e298. [Google Scholar] [CrossRef] [PubMed]
- Emami, B.; Sethi, A.; Petruzzelli, G.J. Influence of MRI on target volume delineation and IMRT planning in nasopharyngeal carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2003, 57, 481–488. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Patient Number | Sex | Age (Years) | Subsite | T-Stage | N-Stage | Grade | p16 Status | GTVCT (cm3) | GTVMR (cm3) | GTVCTMR (cm3) |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | M | 52 | Tonsil | 3 | 2b | 3 | positive | 39.1 | 32.5 | 44.6 |
| 2 | M | 56 | Tonsil | 2 | 2b | 3 | Positive | 4.7 | 1.6 | 6.3 |
| 3 | M | 45 | Base of tongue | 4a | 2b | 3 | Positive | 6.1 | 8.7 | 10.1 |
| 4 | M | 61 | Base of tongue | 2 | 2b | 3 | Positive | 5.3 | 5.8 | 7.0 |
| 5 | M | 53 | Tonsil | 4b | 3 | 3 | Positive | 20.2 | 21.9 | 27.2 |
| 6 | M | 59 | Base of tongue | 4 | 2b | 3 | Positive | 12.5 | 15.3 | 17.8 |
| 7 | M | 57 | Tonsil | 3 | 3 | 3 | Positive | 17.7 | 15.7 | 23.3 |
| 8 | F | 53 | Base of tongue | 2 | 2b | 3 | Positive | 6.4 | 7.1 | 8.5 |
| 9 | F | 66 | Pharyngeal wall | 3 | 1 | 3 | Positive | 21.2 | 18.5 | 23.0 |
| 10 | F | 50 | Base of tongue | 2 | 1 | 3 | Negative | 7.4 | 7.2 | 8.1 |
| 11 | M | 55 | Tonsil | 4a | 2b | 2 | Positive | 22.3 | 29.1 | 30.8 |
| 12 | F | 61 | Base of tongue | 4a | 2b | 3 | Unknown | 24.6 | 28.1 | 31.0 |
| 13 | M | 53 | Tonsil | 2 | 2b | 3 | Positive | 14.8 | 9.6 | 17.7 |
| 14 | M | 65 | Base of tongue | 2 | 2c | 3 | Positive | 4.7 | 11.0 | 11.6 |
| 15 | M | 58 | Tonsil | 4a | 2b | 3 | Negative | 24.0 | 26.5 | 30.8 |
| 16 | M | 49 | Tonsil | 3 | 0 | 3 | Positive | 24.9 | 22.7 | 30.8 |
| 17 | M | 56 | Base of tongue | 4a | 2b | 3 | Positive | 17.0 | 18.8 | 22.7 |
| 18 | F | 62 | Pharyngeal wall | 1 | 2b | 3 | Unknown | 3.5 | 6.0 | 6.3 |
| 19 | F | 62 | Base of tongue | 2 | 2 | 3 | Negative | 7.1 | 9.0 | 11.8 |
| 20 | M | 53 | Base of tongue | 1 | 2b | 2 | Unknown | 3.8 | 3.9 | 5.5 |
| 21 | M | 66 | Tonsil | 2 | 2b | 3 | Unknown | 41.7 | 38.3 | 41.9 |
| 22 | F | 66 | Soft palate | 4a | 1 | 3 | Unknown | 8.3 | 11.5 | 14.7 |
| Modality | Modality GTV Volumes (cm3) | |||||
|---|---|---|---|---|---|---|
| Mean | Median | Mean St. Dev. | Range | GTV Comparison (Wilcoxon Signed Rank Test) | ||
| Max | Min | |||||
| CT | 15.3 | 13.7 | 11.1 | 41.7 | 3.5 | GTVCT–GTVMR, p = 0.47 |
| MR | 15.9 | 13.4 | 10.2 | 38.3 | 1.6 | GTVCTMR–GTVCT, p = 0.018 |
| CT–MR | 19.6 | 17.8 | 11.8 | 44.6 | 5.5 | GTVCTMR–GTVMR, p = 0.010 |
| Metric | DSC | Conformity Index | MDC (mm) | CGD (mm) | |
|---|---|---|---|---|---|
| GTVCTMR−GTVCT Mean (SD) | 0.84 (0.10) | 0.66 (0.12) | 3.74 (1.19) | 2.02 (1.40) | |
| GTVCTMR−GTVMR Mean (SD) | 0.82 (0.10) | 0.65 (0.14) | 4.03 (1.10) | 1.86 (1.59) | |
| GTVCT−GTVMR Mean (SD) | 0.71 (0.13) | 0.50 (0.15) | 5.09 (1.89) | 3.08 (2.37) | |
| Statistical Comparisons of Positional Metrics: p Values | GTVCT−GTVMR versus GTVCTMR−GTVCT | <0.01 | <0.01 | <0.01 | <0.01 |
| GTVCT−GTVMR versus GTVCTMR−GTVMR | <0.01 | <0.01 | <0.01 | <0.01 | |
| GTVCTMR−GTVMR versus GTVCTMR−GTVCT | 0.71 | 0.82 | 0.15 | 0.70 | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Taylor, A.; Sen, M.; Prestwich, R.J.D. Assessment of the Impact of Deformable Registration of Diagnostic MRI to Planning CT on GTV Delineation for Radiotherapy for Oropharyngeal Carcinoma in Routine Clinical Practice. Healthcare 2018, 6, 135. https://doi.org/10.3390/healthcare6040135
Taylor A, Sen M, Prestwich RJD. Assessment of the Impact of Deformable Registration of Diagnostic MRI to Planning CT on GTV Delineation for Radiotherapy for Oropharyngeal Carcinoma in Routine Clinical Practice. Healthcare. 2018; 6(4):135. https://doi.org/10.3390/healthcare6040135
Chicago/Turabian StyleTaylor, Alice, Mehmet Sen, and Robin J. D. Prestwich. 2018. "Assessment of the Impact of Deformable Registration of Diagnostic MRI to Planning CT on GTV Delineation for Radiotherapy for Oropharyngeal Carcinoma in Routine Clinical Practice" Healthcare 6, no. 4: 135. https://doi.org/10.3390/healthcare6040135