Bereaved Family Members’ Satisfaction with Care during the Last Three Months of Life for People with Advanced Illness


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Context and Sample
2.2. Recruitment and Data Collection
The VOICES (SF) Questionnaire
2.3. Statistical Analysis
2.4. Qualitative Descriptive Analysis
3. Results
3.1. Deceased Individuals’ Characteristics
3.2. Participant Characteristics—Family Members
3.3. Satisfaction with Care
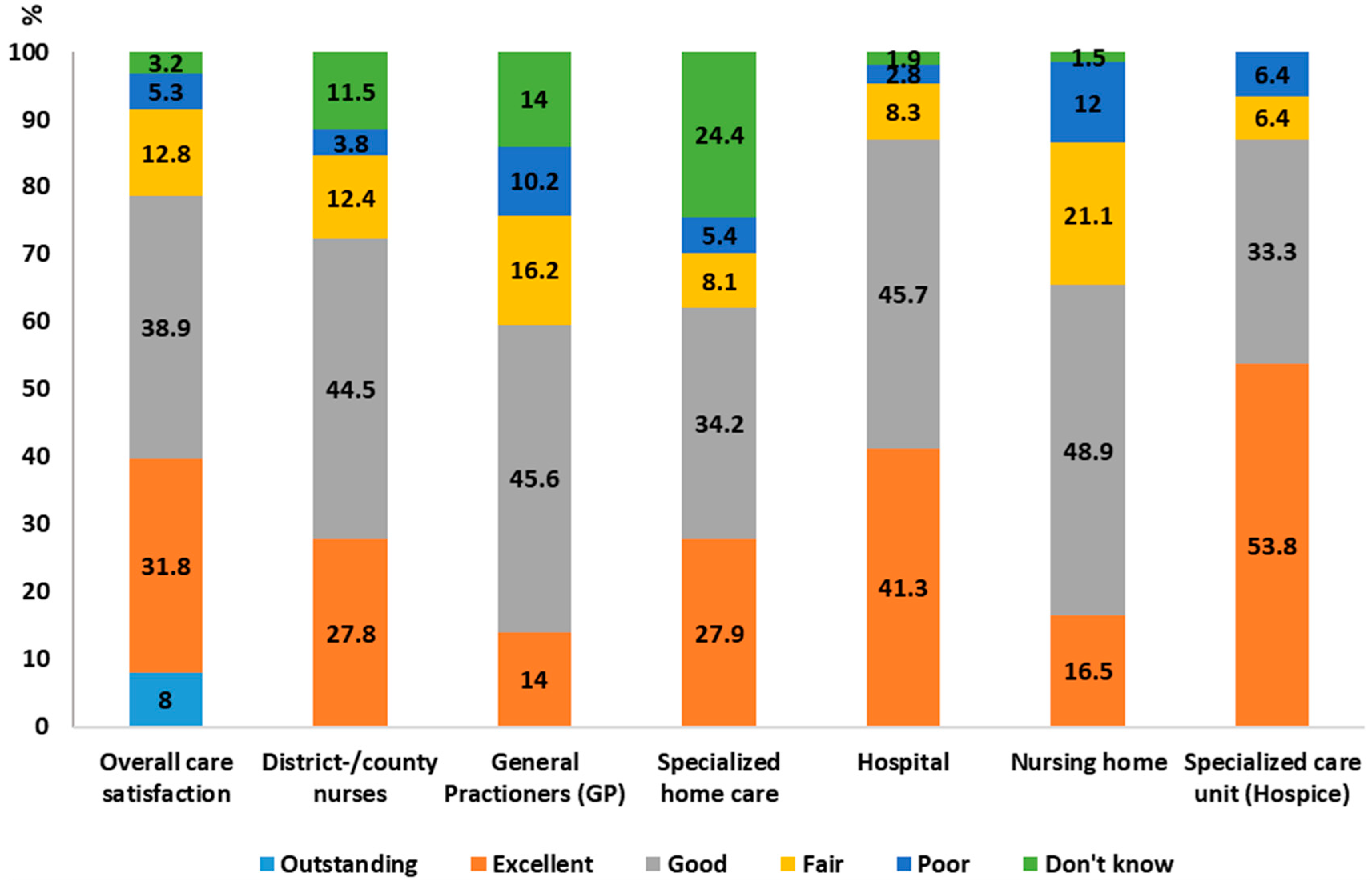
3.3.1. Ratings
3.3.2. Descriptive Responses
Information and Communication
Staff Performance
Care Places and Types of Care Services
3.4. Associations between Satisfaction with Care and Co-Variables
4. Discussion
Methodological Considerations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Murtagh, F.E.; Bausewein, C.; Verne, J.; Groeneveld, E.I.; Kaloki, Y.E.; Higginson, I.J. How many people need palliative care? A study developing and comparing methods for population-based estimates. Palliat. Med. 2014, 28, 49–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morin, L.; Aubry, R.g.; Frova, L.; MacLeod, R.; Wilson, D.M.; Loucka, M.; Csikos, A.; Ruiz-Ramos, M.; Cardenas-Turanzas, M.; YongJoo, R.; et al. Estimating the need for palliative care at the population level: A cross-national study in 12 countries. Palliat. Med. 2017, 21, 526–536. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO) Definition of Palliative Care. Geneva. World Health Organization. Available online: http://www.who.int/cancer/palliative/definition/en/ (accessed on 20 September 2018).
- Radbruch, L. White Paper on standards and norms for hospice and palliative care in Europe: Part 1 Recommendations from the European Association for Palliative Care. Eur. J. Palliat. Care 2010, 17, 22–33. [Google Scholar]
- Payne, M. Inequalities, end-of-life care and social work. Prog. Palliat. Care 2010, 18, 221–227. [Google Scholar] [CrossRef]
- Gardiner, C.; Cobb, M.; Gott, M.; Ingleton, C. Barriers to providing palliative care for older people in acute hospitals. Age Ageing 2011, 40, 233–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindskog, M.; Tavelin, B.; Lundström, S. Old age as risk indicator for poor end-of-life care quality—A population-based study of cancer deaths from the swedish register of palliative care. Eur. J. Cancer 2015, 51, 1331–1339. [Google Scholar] [CrossRef] [PubMed]
- Bossuyt, N.; Van den Block, L.; Cohen, J.; Meeussen, K.; Bilsen, J.; Echteld, M.; Deliens, L.; Van Casteren, V. Is individual educational level related to end-of-life care use? Results from a nationwide retrospective cohort study in belgium. J. Palliat. Med. 2011, 14, 1135–1141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmadi, Z.; Lundström, S.; Janson, C.; Strang, P.; Emtner, M.; Currow, D.C.; Ekström, M. End-of-life care in oxygen-dependent copd and cancer: A national population-based study. Eur. Respir. J. 2015, 46, 1190–1193. [Google Scholar] [CrossRef] [PubMed]
- Romem, A.; Tom, S.E.; Beauchene, M.; Babington, L.; Scharf, S.M. Pain management at the end of life: A comparative study of cancer, dementia, and chronic obstructive pulmonary disease patients. Palliat. Med. 2015, 29, 464–469. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, H.; Milberg, A.; Hjelm, K.; Friedrichsen, M. End of life care for patients dying of stroke: A comparative registry study of stroke and cancer. PLoS ONE 2016, 11, e0147694. [Google Scholar] [CrossRef] [PubMed]
- Bausewein, C.; Daveson, B.A.; Currow, D.C.; Downing, J.; Deliens, L.; Radbruch, L.; Defilippi, K.; Lopes Ferreira, P.; Costantini, M.; Harding, R.; et al. Eapc white paper on outcome measurement in palliative care: Improving practice, attaining outcomes and delivering quality services—Recommendations from the european association for palliative care (eapc) task force on outcome measurement. Palliat. Med. 2016, 30, 6–22. [Google Scholar] [CrossRef] [PubMed]
- McPherson, C.J.; Addington-Hall, J.M. Judging the quality of care at the end of life: Can proxies provide reliable information? Soc. Sci. Med. 2003, 56, 95–109. [Google Scholar] [CrossRef]
- Henoch, I.; Lövgren, M.; Wilde-Larsson, B.; Tishelman, C. Perception of quality of care: Comparison of the views of patients’ with lung cancer and their family members. J. Clin. Nurs. 2012, 21, 585–594. [Google Scholar] [CrossRef] [PubMed]
- Erin, S.; Brigette, H.; Blair, H.; Wei, X.; Jeff, M.; Lesia, W.; Ru, T.; Daren, H.; Robert, F. Factors affecting family satisfaction with inpatient end-of-life care. PLoS ONE 2014, 11, e110860. [Google Scholar]
- Virdun, C.; Luckett, T.; Davidson, P.M.; Phillips, J. Dying in the hospital setting: A systematic review of quantitative studies identifying the elements of end-of-life care that patients and their families rank as being most important. Palliat. Med. 2015, 29, 774–796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Addington-Hall, J.M.; O’Callaghan, A.C. A comparison of the quality of care provided to cancer patients in the uk in the last three months of life in in-patient hospices compared with hospitals, from the perspective of bereaved relatives: Results from a survey using the voices questionnaire. Palliat. Med. 2009, 23, 190–197. [Google Scholar] [CrossRef] [PubMed]
- Hunt, K.J.; Shlomo, N.; Richardson, A.; Addington-Hall, J. Voices Re-Design and Testing to Inform a National End-of-Life Care Survey; Final report for the department for health; University of South Hampton: Southampton, UK, 2011. [Google Scholar]
- Roza, K.A.; Lee, E.J.; Meier, D.E.; Goldstein, N.E. A survey of bereaved family members to assess quality of care on a palliative care unit. J. Palliat. Med. 2015, 18, 358–365. [Google Scholar] [CrossRef] [PubMed]
- Ong, J.; Brennsteiner, A.; Chow, E.; Hebert, R.S. Correlates of family satisfaction with hospice care: General inpatient hospice care versus routine home hospice care. J. Palliat. Med. 2016, 19, 97–100. [Google Scholar] [CrossRef] [PubMed]
- Kaarbø, E. End-of-life care in two norwegian nursing homes: Family perceptions. J. Clin. Nurs. 2011, 20, 1125–1132. [Google Scholar] [CrossRef] [PubMed]
- Andersson, S.; Lindqvist, O.; Fürst, C.J.; Brännström, M. End-of-life care in residential care homes: A retrospective study of the perspectives of family members using the voices questionnaire. Scand. J. Caring Sci. 2016, 31, 72–84. [Google Scholar] [CrossRef] [PubMed]
- Pivodic, L.; Pardon, K.; Morin, L.; Addington-Hall, J.; Miccinesi, G.; Cardenas-Turanzas, M.; Onwuteaka-Philipsen, B.; Naylor, W.; Ruiz Ramos, M.; Van den Block, L.; et al. Place of death in the population dying from diseases indicative of palliative care need: A cross-national population-level study in 14 countries. J. Epidemiol. Community Health 2016, 70, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Al-Qurainy, R.; Collis, E.; Feuer, D. Dying in an acute hospital setting: The challenges and solutions. Int. J. Clin. Pract. 2009, 63, 508–515. [Google Scholar] [CrossRef] [PubMed]
- Woo, J.; Lo, R.; Cheng, J.O.Y.; Wong, F.; Mak, B. Quality of end-of-life care for non-cancer patients in a non-acute hospital. J. Clin. Nurs. 2011, 20, 1834–1841. [Google Scholar] [CrossRef] [PubMed]
- Reyniers, T.; Houttekier, D.; Cohen, J.; Pasman, H.R.; Deliens, L. The acute hospital setting as a place of death and final care: A qualitative study on perspectives of family physicians, nurses and family carers. Health Place 2014, 27, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Penders, Y.W.; Van den Block, L.; Donker, G.A.; Deliens, L.; Onwuteaka-Philipsen, B.; Euro, I. Comparison of end-of-life care for older people living at home and in residential homes: A mortality follow-back study among gps in the netherlands. Br. J. Gen. Pract. 2015, 65, e724–e730. [Google Scholar] [CrossRef] [PubMed]
- Morin, L.; Johnell, K.; Van den Block, L.; Aubry, R.g. Discussing end-of-life issues in nursing homes: A nationwide study in france. Age Ageing 2016, 45, 395–402. [Google Scholar] [CrossRef] [PubMed]
- Smedbäck, J.; Öhlen, J.; Årestedt, K.; Alvariza, A.; Fürst, C.J.; Håkanson, C. Palliative care during the final week of life of older people in nursing homes: A register-based study. Palliat. Support. Care 2017, 15, 417–424. [Google Scholar] [CrossRef] [PubMed]
- Håkanson, C.; Öhlen, J.; Morin, L.; Cohen, J. A population-level study of place of death and associated factors in sweden. Scand. J. Public Health 2015, 43, 744–751. [Google Scholar] [CrossRef] [PubMed]
- Young, A.J.; Rogers, A.; Addington-Hall, J.M. The quality and adequacy of care received at home in the last 3 months of life by people who died following a stroke: A retrospective survey of surviving family and friends using the views of informal carers evaluation of services questionnaire. Health Soc. Care Community 2008, 16, 419–428. [Google Scholar] [CrossRef] [PubMed]
- Young, A.J.; Rogers, A.; Dent, L.; Addington-Hall, J.M. Experiences of hospital care reported by bereaved relatives of patients after a stroke: A retrospective survey using the voices questionnaire. J. Adv. Nurs. 2009, 65, 2161–2174. [Google Scholar] [CrossRef] [PubMed]
- Hughes, R.; Saleem, T.; Addington-Hall, J. Towards a culturally acceptable end-of-life survey questionnaire: A bengali translation of voices. Int. J. Palliat. Nurs. 2005, 11, 116–123. [Google Scholar] [CrossRef] [PubMed]
- Ross, L.; Neergaard, M.A.; Petersen, M.A.; Groenvold, M. Measuring the quality of end-of-life care: Development, testing, and cultural validation of the danish version of views of informal carers’ evaluation of services--short form. Palliat. Med. 2018, 32, 804–814. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, A.; Öhlen, J.; Alvariza, A.; Håkanson, C. Adaptation and validation of the voices (sf) questionnaire—For evaluation of end-of-life care in sweden. Scand. J. Caring Sci. 2017, 32, 1254–1260. [Google Scholar] [CrossRef] [PubMed]
- Krippendorff, K. Content Analysis: An Introduction to Its Methodology, 3rd ed.; SAGE: Los Angeles, CA, USA, 2013. [Google Scholar]
- Ringdal, G.I.; Jordhøy, M.S.; Kaasa, S. Family satisfaction with end-of-life care for cancer patients in a cluster randomized trial. J. Pain Symptom Manag. 2002, 24, 53–63. [Google Scholar] [CrossRef]
- Ozcelik, H.; Cakmak, D.E.; Fadiloglu, C.; Yildirim, Y.; Uslu, R. Determining the satisfaction levels of the family members of patients with advanced-stage cancer. Palliat. Support. Care 2015, 13, 741–747. [Google Scholar] [CrossRef] [PubMed]
- Brown, C.E.; Jecker, N.S.; Curtis, J.R. Inadequate palliative care in chronic lung disease. An issue of health care inequality. Ann. Am. Thorac. Soc. 2016, 13, 311–316. [Google Scholar] [CrossRef] [PubMed]
- Hess, S.; Stiel, S.; Hofmann, S.; Klein, C.; Lindena, G.; Ostgathe, C. Trends in specialized palliative care for non-cancer patients in germany—Data from the national hospice and palliative care evaluation (hope). Eur. J. Intern. Med. 2014, 25, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Lundström, S.; Fransson, G.; Axelsson, B. Specialized Palliative Care in Sweden, for Whom and How Well? Palliat. Med. 2016, 30, NP173. [Google Scholar]
- Rosenwax, L.; Spilsbury, K.; McNamara, B.; Semmens, J. A Retrospective Population Based Cohort Study of Access to Specialist Palliative Care in the Last Year of Life: Who Is Still Missing out a Decade on? BioMed Central Ltd.: London, UK, 2016. [Google Scholar]
- Witkamp, F.E.; van Zuylen, L.; Borsboom, G.; van der Rijt, C.C.; van der Heide, A. Dying in the hospital: What happens and what matters, according to bereaved relatives. J. Pain Symptom Manag. 2015, 49, 203–213. [Google Scholar] [CrossRef] [PubMed]
- de Boer, D.; Hofstede, J.M.; de Veer, A.J.E.; Raijmakers, N.J.H.; Francke, A.L. Relatives’ perceived quality of palliative care: Comparisons between care settings in which patients die. BMC Palliat. Care 2017, 16, 41. [Google Scholar] [CrossRef] [PubMed]
- National board of Health Care. Palliative Care Ath the End of life: Summary and Improvement Areas. (In Swedish: Palliativ vård i livets slutskede: Sammanfattning med förbättringsområden). Available online: http://www.socialstyrelsen.se/Lists/Artikelkatalog/Attachments/20396/2016-12-3.pdf (accessed on 30 October 2018).
- Mousing, C.A.; Timm, H.; Lomborg, K.; Kirkevold, M. Barriers to palliative care in people with chronic obstructive pulmonary disease in home care: A qualitative study of the perspective of professional caregivers. J. Clin. Nurs. 2018, 27, 650–660. [Google Scholar] [CrossRef] [PubMed]
- Van Riet Paap, J.; Vernooij-Dassen, M.; Brouwer, F.; Meiland, F.; Iliffe, S.; Davies, N.; Leppert, W.; Jaspers, B.; Mariani, E.; Sommerbakk, R.; et al. Improving the organization of palliative care: Identification of barriers and facilitators in five European countries. Implement Sci. 2014, 9, 130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lundquist, G.; Rasmussen, B.H.; Axelsson, B. Information of imminent death or not: Does it make a difference? J. Clin. Oncol. 2011, 29, 3927–3931. [Google Scholar] [CrossRef] [PubMed]
- Robinson, J.; Gott, M.; Ingleton, C. Patient and family experiences of palliative care in hospital: What do we know? An integrative review. Palliat. Med. 2014, 28, 18–33. [Google Scholar] [CrossRef] [PubMed]
- De Santo-Madeya, S.; Safizadeh, P. Family satisfaction with end-of-life care in the intensive care unit: A systematic review of the literature. Dimens. Crit. Care Nurs. 2017, 36, 278–283. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Deceased Individuals | Family Members | ||
|---|---|---|---|---|
| % a | n | % a | n | |
| Sex (Missing = x/485) | - | (0/485) | - | (0/485) |
| Male | 50.3 | (244) | 29.3 | (142) |
| Female | 49.7 | (241) | 70.7 | (343) |
| Age (Missing = x/485) | - | (1/485) | - | (8/485) |
| 18–29 | - | - | 0.8 | (4) |
| 30–39 | - | - | 1.6 | (8) |
| 40–49 | 1.2 | (6) | 6.8 | (33) |
| 50–59 | 2.3 | (11) | 22.3 | (108) |
| 60–69 | 8.9 | (43) | 31.3 | (152) |
| 70–79 | 23.1 | (112) | 22.9 | (111) |
| 80–89 | 36.7 | (178) | 11.3 | (55) |
| 90+ | 27.6 | (134) | 1.2 | (6) |
| Educational attainment (Missing = x/485) | - | (5/485) | - | (3/485) |
| Lower secondary education | 72.4 | (351) | 29.5 | (143) |
| Higher secondary education | 11.1 | (54) | 30.5 | (148) |
| Higher education | 15.5 | (75) | 39.4 | (191) |
| Direct cause of death b | - | - | - | - |
| Cancer | 20.2 | (66) | - | - |
| Heart diseases (incl. cerebrovascular) | 42.5 | (139) | - | - |
| Alzheimer’s | 0 | (0) | - | - |
| Respiratory diseases | 32.4 | (106) | - | - |
| Renal diseases | 3.1 | (10) | - | - |
| Neurodegenerative diseases | 0.6 | (2) | - | - |
| Liver diseases | 1.2 | (4) | - | - |
| Underlying cause of death 1 b | - | - | - | - |
| Cancer | 15.8 | (64) | - | - |
| Heart diseases (incl. cerebrovascular) | 56.3 | (228) | - | - |
| Alzheimer’s | 1.0 | (4) | - | - |
| Respiratory diseases | 15.1 | (61) | - | - |
| Renal diseases | 9.4 | (38) | - | - |
| Neurodegenerative diseases | 1.0 | (4) | - | - |
| Liver diseases | 1.5 | (6) | - | - |
| Underlying cause of death 2 b | - | - | - | - |
| Cancer | 15.2 | (52) | - | - |
| Heart diseases (incl. cerebrovascular) | 64.3 | (220) | - | - |
| Alzheimer’s | 3.5 | (12) | - | - |
| Respiratory diseases | 10.2 | (35) | - | - |
| Renal diseases | 4.4 | (15) | - | - |
| Neurodegenerative diseases | 0.9 | (3) | - | - |
| Liver diseases | 1.2 | (4) | - | - |
| HIV/Aids | 0.3 | (1) | - | - |
| Length of illness before death (Missing = x/485) | - | (6/485) | - | - |
| Sudden | 5.4 | (26) | - | - |
| <24 h | 2.1 | (10) | - | - |
| >24 h–1 week | 10.7 | (52) | - | - |
| >1 week–1 month | 13.0 | (63) | - | - |
| >1 month–6 months | 14.8 | (72) | - | - |
| >6 months–1 year | 10.3 | (50) | - | - |
| 1 year or more | 42.5 | (206) | - | - |
| Relationship (Missing = x/485) | - | (4/485) | - | - |
| Spouse | 34.5 | (166) | - | - |
| Child | 51.8 | (249) | - | - |
| Other c | 13.7 | (66) | - | - |
| Co-Variables | Overall High Satisfaction OR a 95% CI b | p-Value c |
|---|---|---|
| Deceased individuals | - | - |
| Sex | - | - |
| Male | 1 d | |
| Female | 0.98 (0.62–1.56) | 0.95 |
| Age | - | - |
| <85 | 1 | - |
| >85 | 1.54 (0.94–2.51) | 0.08 |
| Underlying cause of death | - | - |
| Non-cancer | 1 | - |
| Cancer | 2.10 (1.19–3.73) | 0.01 |
| Length of illness before death | - | - |
| Less than 1 year | 1 | - |
| 1 year or more | 0.57 (0.35–0.91) | 0.01 |
| Health Care region | - | - |
| Southeast | 1 | - |
| Stockholm | 1.29 (0.81–2.07) | 0.27 |
| Bereaved family members | - | - |
| Sex | - | - |
| Male | 1 | - |
| Female | 0.84 (0.49–1.43) | 0.53 |
| Age | - | - |
| 18–59 | 1 | - |
| 60+ | 1.05 (0.37–1.93) | 0.85 |
| Relationship | - | - |
| Spouse | 2.86 (1.40–5.80) | 0.00 |
| Child | 1.98 (1.07–3.69) | 0.03 |
| Other e | 1 | - |
| Educational attainment | - | - |
| Lower/elementary | 1 | - |
| Higher secondary/higher | 0.49 (0.26–0.92) | 0.02 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
O’Sullivan, A.; Alvariza, A.; Öhlen, J.; Håkanson, C. Bereaved Family Members’ Satisfaction with Care during the Last Three Months of Life for People with Advanced Illness. Healthcare 2018, 6, 130. https://doi.org/10.3390/healthcare6040130
O’Sullivan A, Alvariza A, Öhlen J, Håkanson C. Bereaved Family Members’ Satisfaction with Care during the Last Three Months of Life for People with Advanced Illness. Healthcare. 2018; 6(4):130. https://doi.org/10.3390/healthcare6040130
Chicago/Turabian StyleO’Sullivan, Anna, Anette Alvariza, Joakim Öhlen, and Cecilia Håkanson. 2018. "Bereaved Family Members’ Satisfaction with Care during the Last Three Months of Life for People with Advanced Illness" Healthcare 6, no. 4: 130. https://doi.org/10.3390/healthcare6040130