Subjective Assessment of Head and Facial Appearance in Children with Craniosynostoses after Surgical Treatment


Abstract
:1. Introduction
2. Methods
2.1. Participants and Research Strategies
2.2. Data Analysis
3. Results
3.1. Demographics
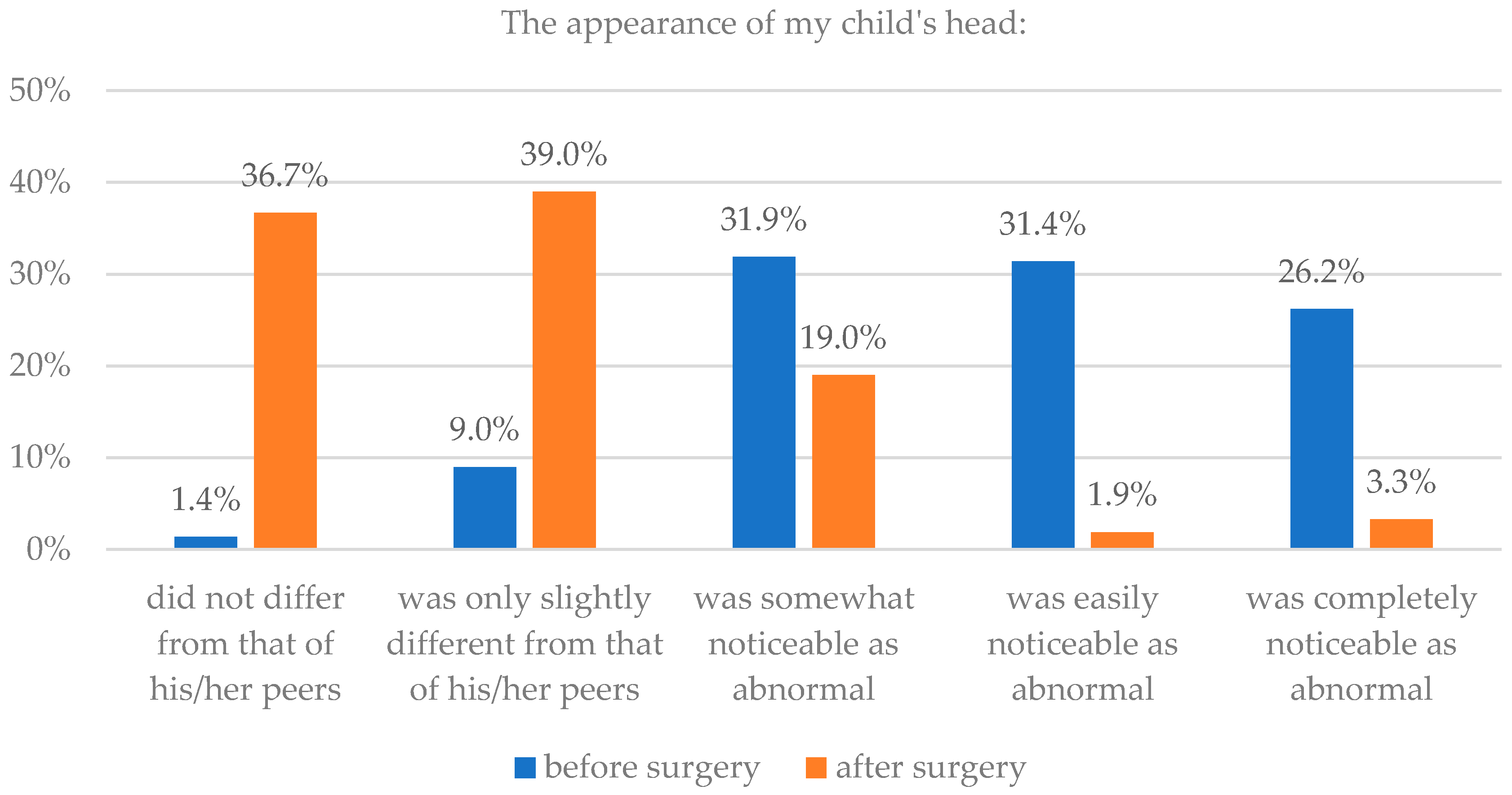
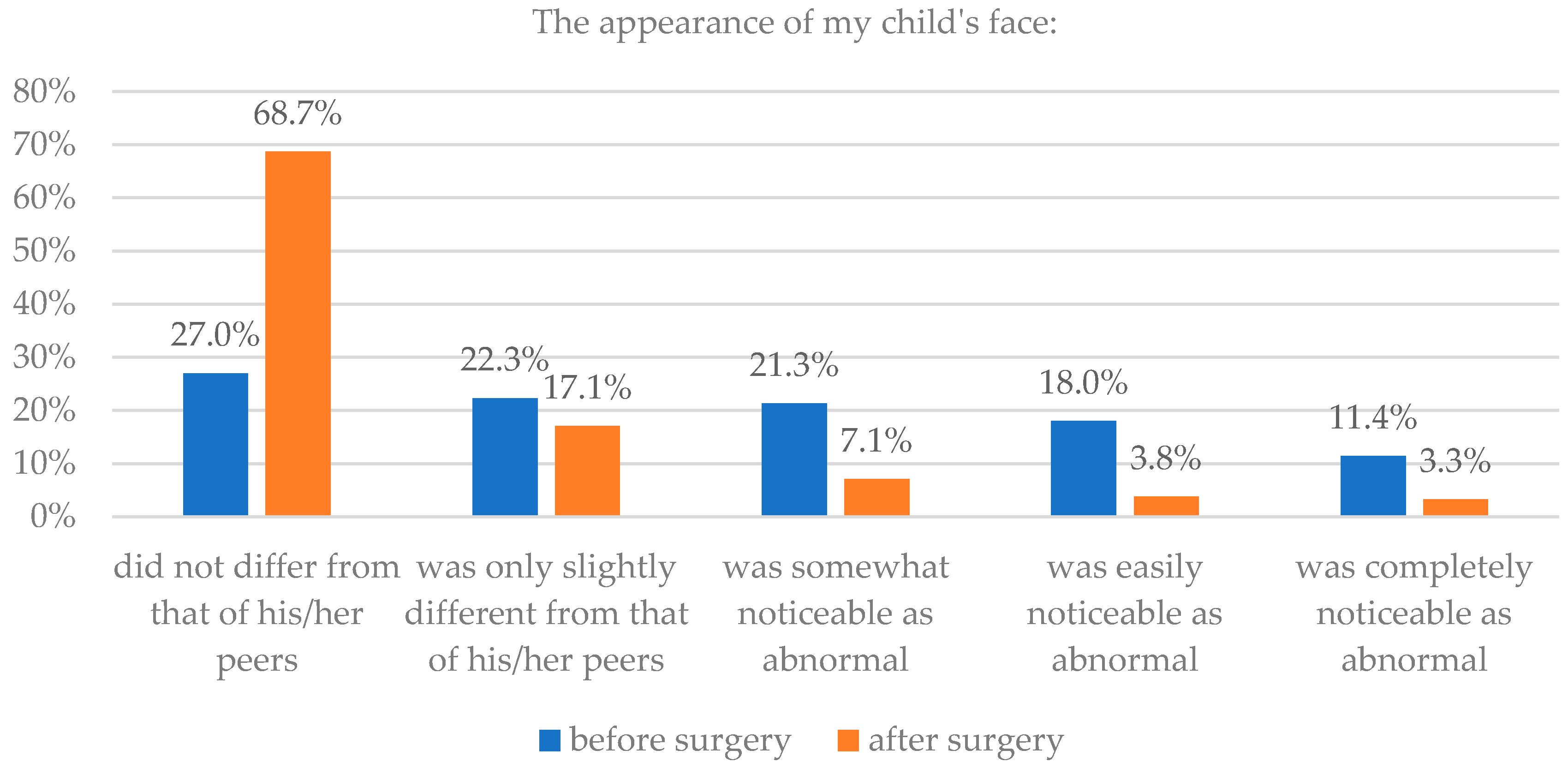
3.2. Parent Assessment of Head and Facial Appearance before and after Surgery
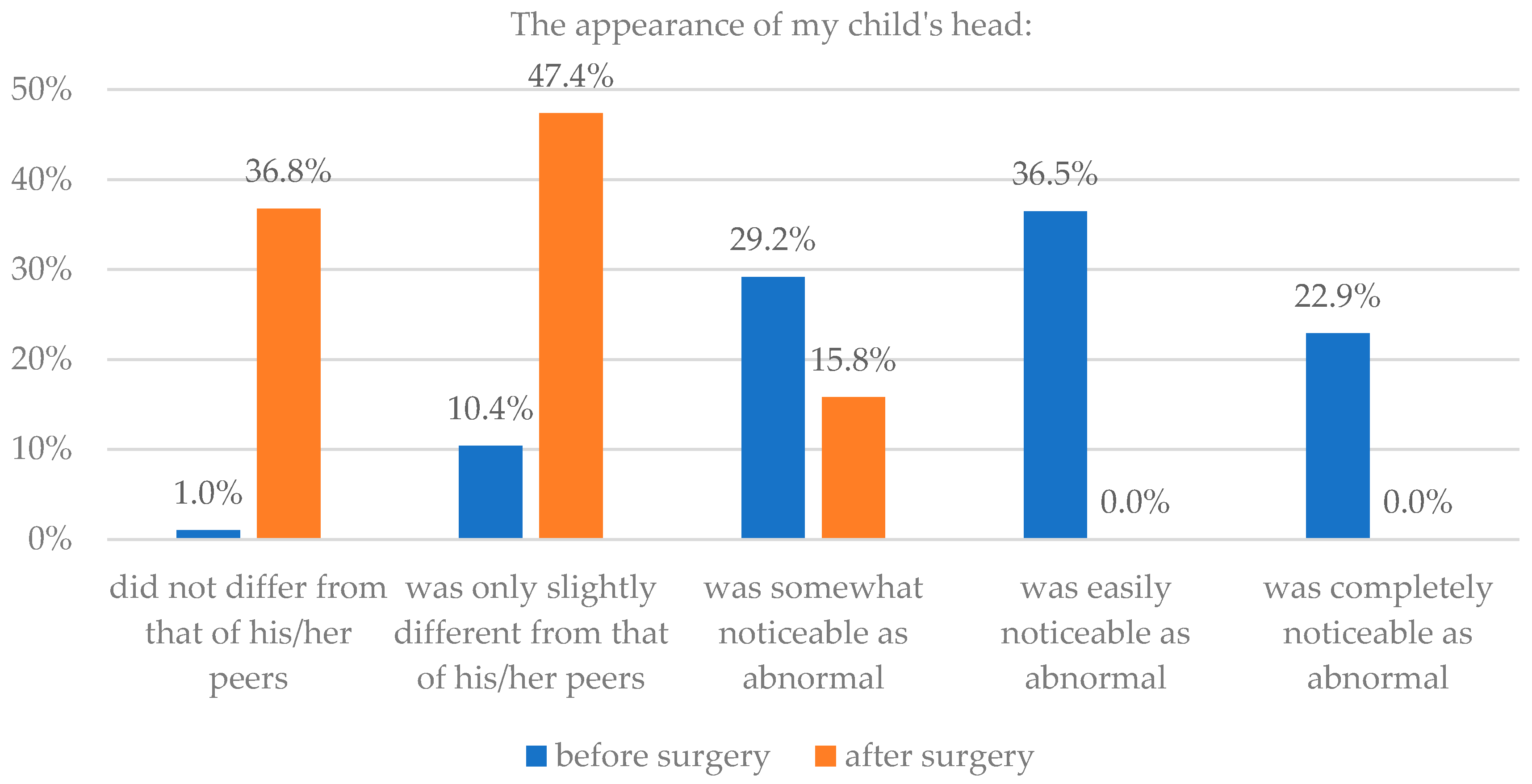
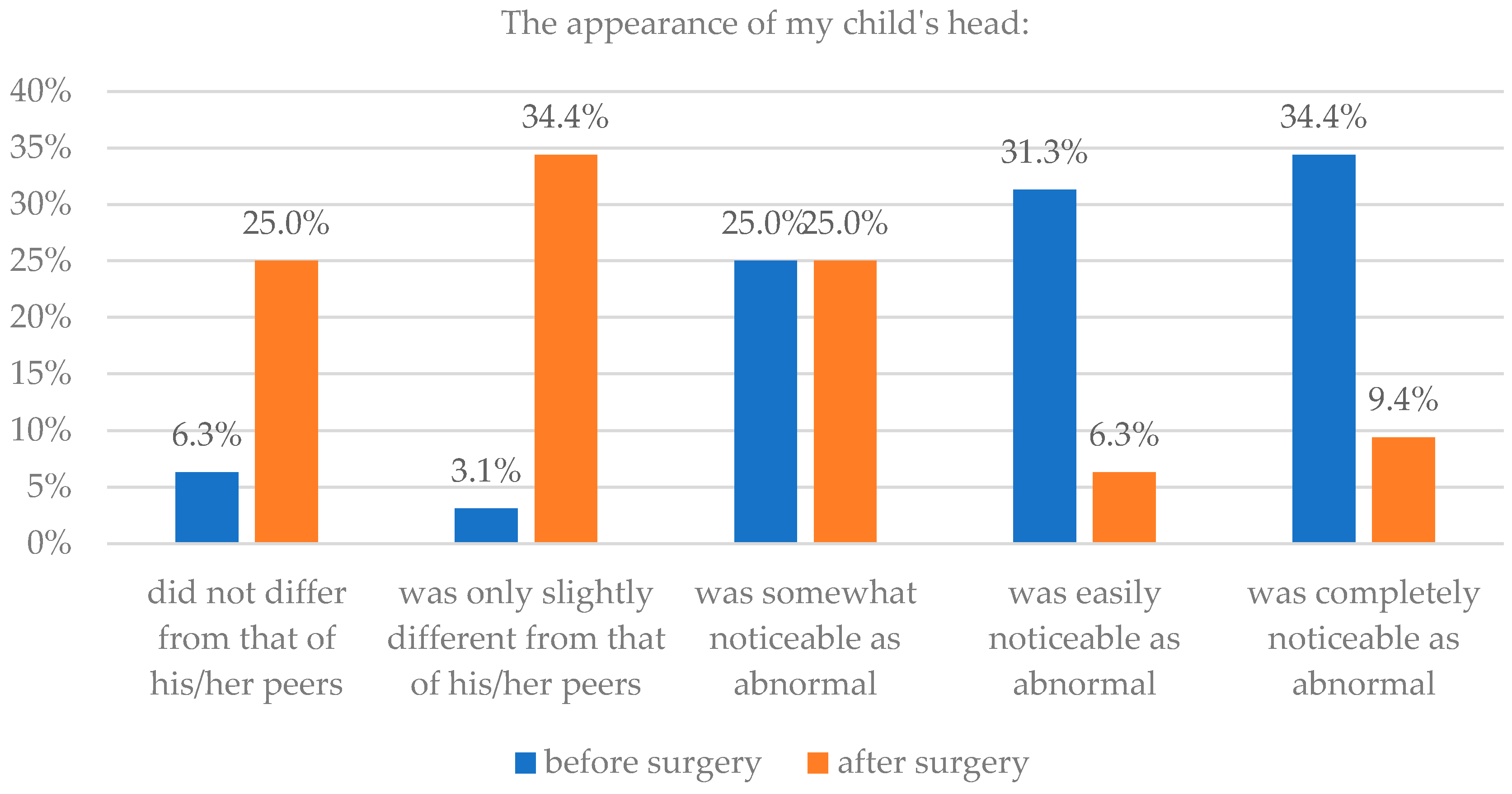
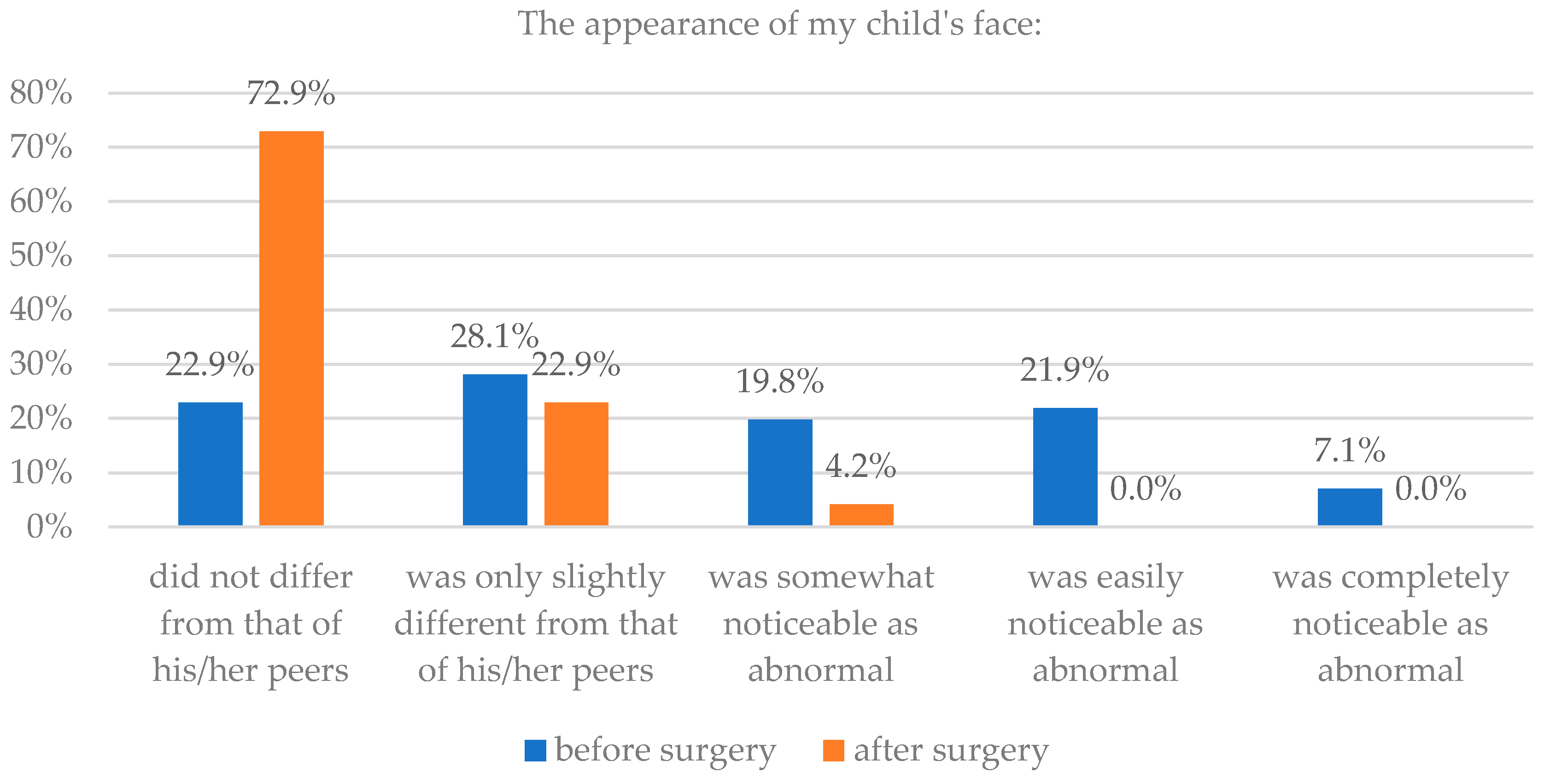
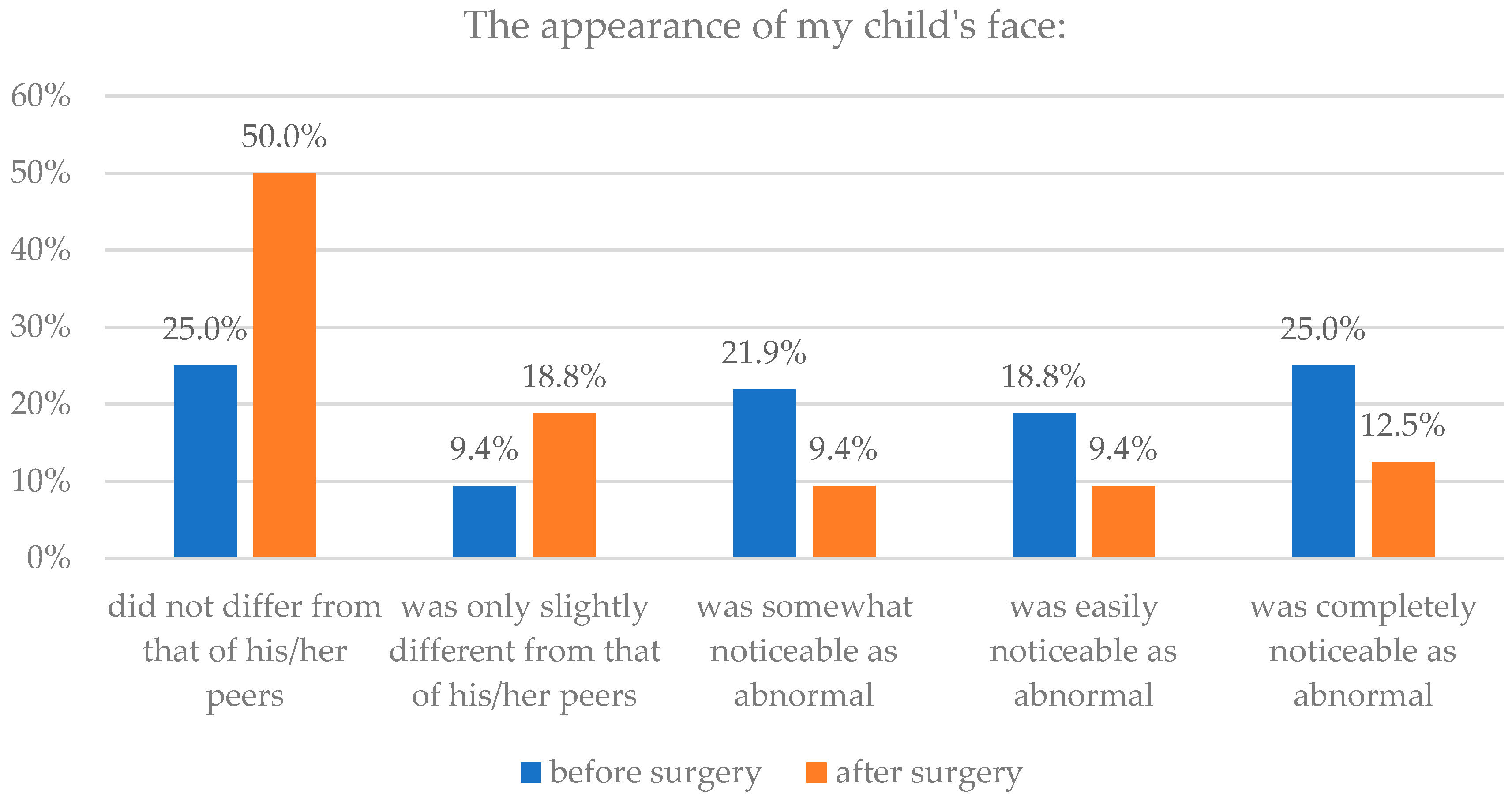
3.3. Influence of Type of Craniosynostosis on Parents’ Assessment of Head and Facial Appearance before and after Surgery
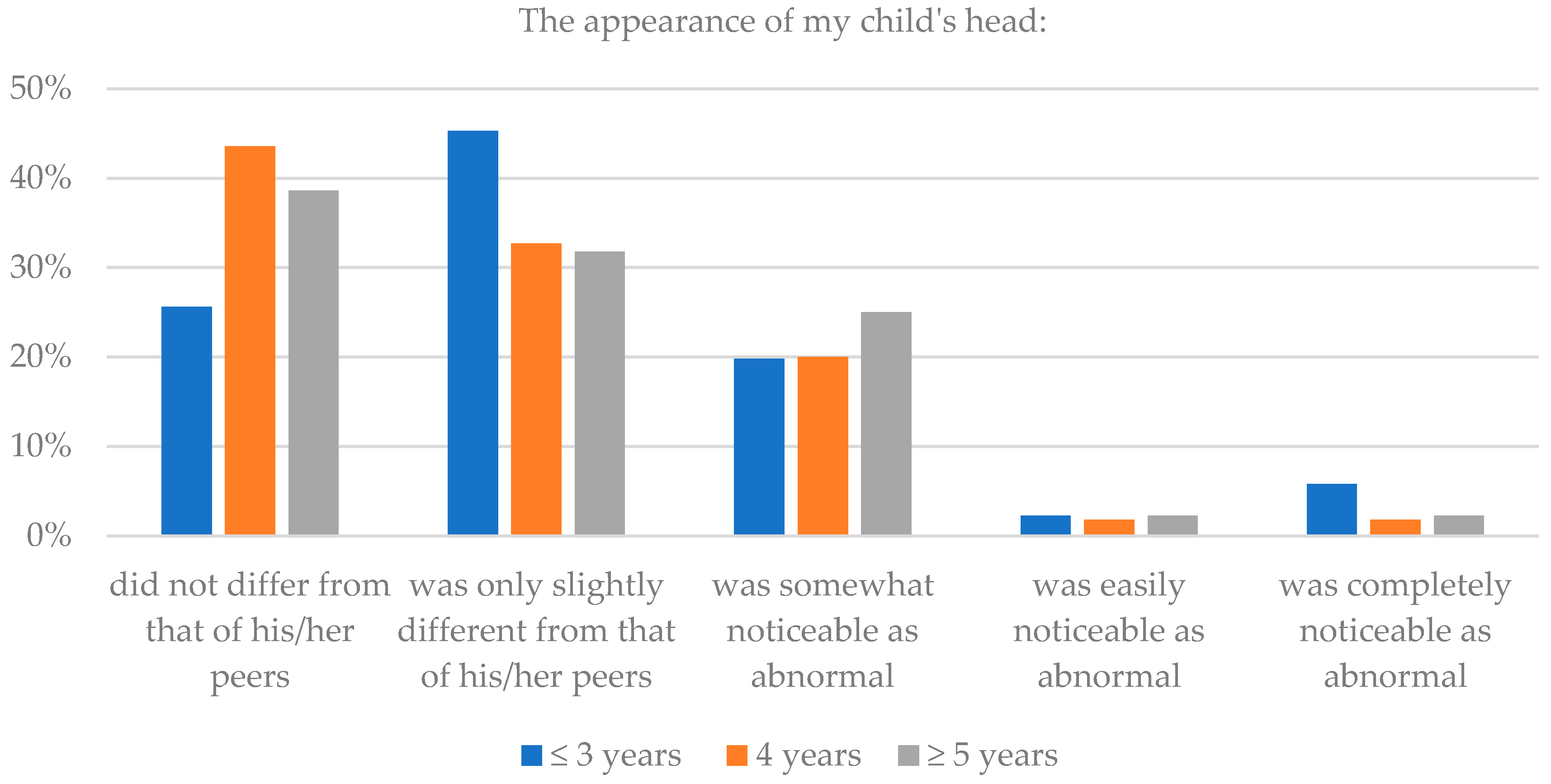
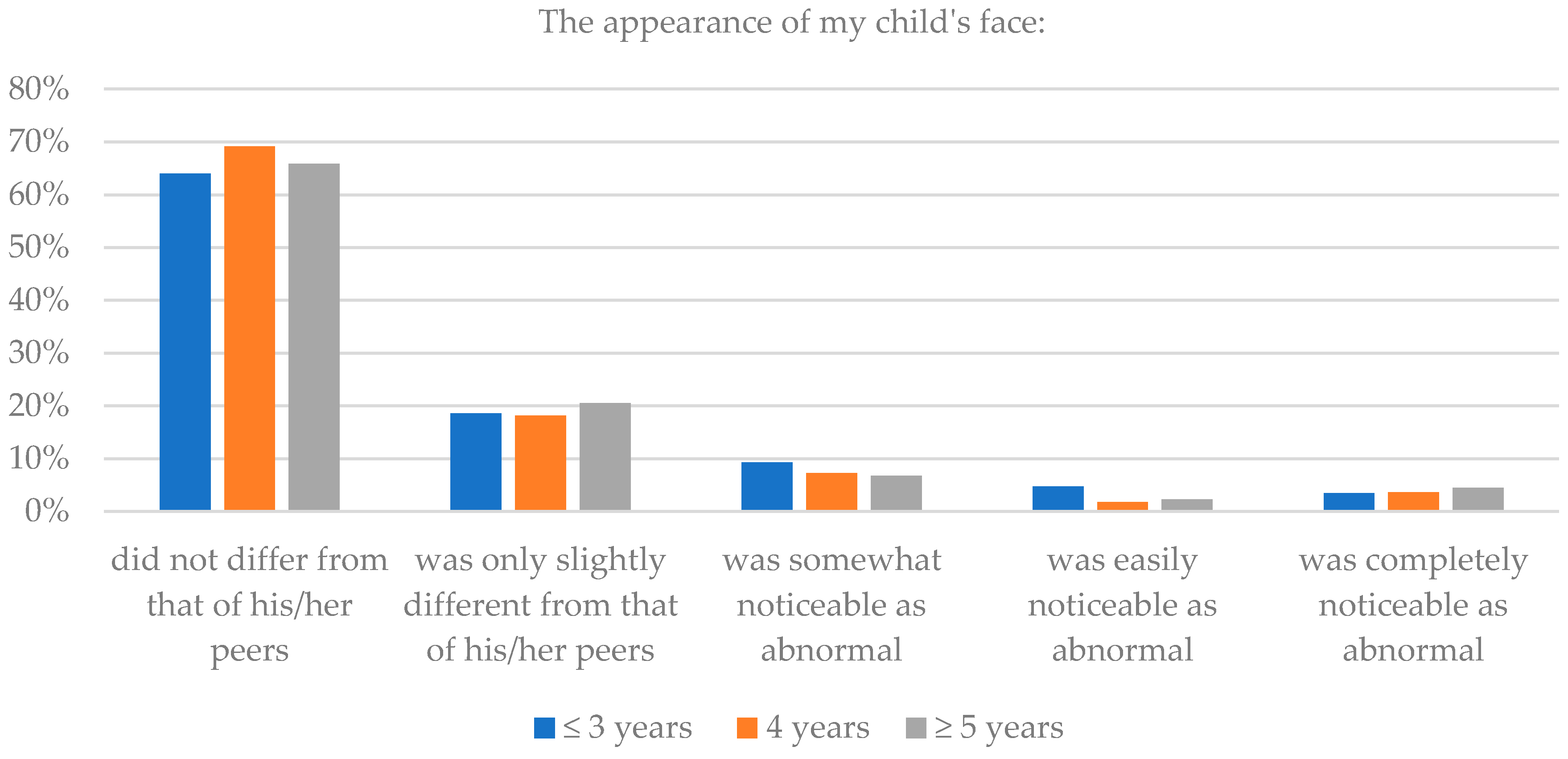
3.4. The Children’s Age (at the Moment of Survey) and Assessment of Head and Facial Appearance after Surgery
3.5. Parents’ Assessment of Their Child’s Interpersonal Relationships after Surgery
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Ethical Statement
Appendix A
- -
- Child’s sex: girl/boy
- -
- Age of child (in months)
- -
- Type of craniosynostosis: sagittal; metopic; unicoronal; bicoronal; lambdoid; complex; genetic syndrome
- -
- Surgery: yes/no
- -
- Age of child at the time of surgery (in months)
- -
- The appearance of my child’s head before surgery: did not differ from that of his/her peers; was only slightly different from that of his/her peers; was somewhat noticeable as abnormal; was easily noticeable as abnormal; was completely noticeable as abnormal
- -
- The appearance of my child’s head after surgery: do not differ from that of his/her peers; is only slightly different from that of his/her peers; is somewhat noticeable as abnormal; is easily noticeable as abnormal; is completely noticeable as abnormal
- -
- The appearance of my child’s face before surgery: did not differ from that of his/her peers; was only slightly different from that of his/her peers; was somewhat noticeable as abnormal; was easily noticeable as abnormal; was completely noticeable as abnormal
- -
- The appearance of my child’s face after surgery: do not differ from that of his/her peers; is only slightly different from that of his/her peers; is somewhat noticeable as abnormal; Is easily noticeable as abnormal; is completely noticeable as abnormal
- -
- How does your child relate to peers after surgery: very easily; rather easily; hard to say; not very well; poorly
- -
- How does your child relate to adults after surgery: very easily; rather easily; hard to say; not very well; poorly
- -
- Whether peers react negatively to the shape of your child’s head after surgery: never; seldom; sometimes; often; always
- -
- Whether adults react negatively to the shape of your child’s head after surgery: never; seldom; sometimes; often; always
- -
- Does your child like to play with peers after surgery: really like; like; hard to say; does not like; really does not like
- -
- How do peers relate to your child after surgery: very easily; rather easily; hard to say; not very well; poorly
References
- Kępiński, A. Twarz i ręka. Teksty Teor. Lit. Kryt. Interpret. 1997, 2, 9–34. [Google Scholar]
- Talley, H.L. Saving Face. Disfigurement and the Politics of Appearance; New York University Press: New York, NY, USA; London, UK, 2014; ISBN 978-0-8147-8410-5. [Google Scholar]
- Goffman, E. Behavior in Public Places. Notes on the Social Organization of Gatherings; The Free Press: New York, NY, USA, 1963; ISBN 978-0-02-911940-2. [Google Scholar]
- Goffman, E. Interaction Ritual. Essays in Face-to-Face Behawior; Anchor Books: New York, NY, USA, 1967; ISBN 0-394-70631-5. [Google Scholar]
- Macgregor, F.C. Facial disfigurement: Problems and management of social interaction and implications for mental health. Aesthet. Plast. Surg. 1990, 14, 249–257. [Google Scholar] [CrossRef]
- Rumsey, N.; Hacourt, D. The Psychology of Appearance; Open University Press: Maidenhead, UK, 2005; ISBN 10 033521276X. [Google Scholar]
- Pope, A.W.; Ward, J. Self-perceived facial appearance and psychosocial adjustment in preadolescents with craniofacial anomalies. Cleft Palate Craniofac. J. 1997, 34, 396–401. [Google Scholar] [CrossRef]
- Prior, J.; O’Dell, L. ‘Coping quite well with a few difficult bits’ living with disfigurement in early adolescence. J. Health Psychol. 2009, 14, 731–740. [Google Scholar] [CrossRef] [PubMed]
- Kish, V.; Lansdown, R. Meeting the psychosocial impact of facial disfigurement: Developing a clinical service for children and families. Clin. Child Psychol. Psychiatry 2000, 5, 497–512. [Google Scholar] [CrossRef]
- Caroll, P.; Shute, R. School peer victimization of young people with craniofacial conditions: A comparative study. Psychol. Health Med. 2005, 10, 291–305. [Google Scholar] [CrossRef]
- Harlock, N.; Vögelin, E.; Bradbury, E.T.; Grobbelaar, A.O.; Gault, D.T. Psychosocial outcome of patients after ear reconstruction: A retrospective study of 62 patients. Ann. Plast. Surg. 2005, 54, 517–524. [Google Scholar] [CrossRef]
- Kapp-Simon, K.A.; McGuire, D. Observed social interaction patterns in adolescents with and without craniofacial conditions. Cleft Palate Craniofac. J. 1997, 34, 380–384. [Google Scholar] [CrossRef]
- Lajeunie, E.; Le Merrer, M.; Marchac, D.; Renier, D. Syndromal and nonsyndromal primary trigonocephaly: Analysis of a series of 237 patients. Am. J. Med. Genet. 1998, 75, 211–215. [Google Scholar] [CrossRef]
- Slater, B.J.; Lenton, K.A.; Kwan, M.D.; Gupta, D.M.; Wan, D.C.; Longaker, M.T. Cranial sutures: A brief review. Plast. Reconstr. Surg. 2008, 121, 170e–178e. [Google Scholar] [CrossRef] [PubMed]
- Timberlake, A.T.; Furey, C.G.; Choi, J.; Nelson-Williams, C.; Loring, E.; Galm, A.; Kahle, K.T.; Steinbacher, D.M.; Larysz, D.; Persing, J.A.; et al. De novo mutations in inhibitors of Wnt, BMP, and Ras/ERK signaling pathways in non-syndromic midline craniosynostosis. Proc. Natl. Acad. Sci. USA 2017, 114, E7341–E7347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kana, M.A.; Baduku, T.S.; Bello-Manga, H.; Baduku, A.S. A 37-year-old Nigerian woman with Apert syndrome—Medical and psychosocial perspectives: A case report. J. Med. Case Rep. 2018, 12, 126. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, M.S.; Venugopal, A.; Horton, J.; Rodrigues, D.; Nishikawa, H.; White, N.; Solanki, G.; Noons, P.; Evans, M.; Dover, S. The quality of life in adult patients with syndromic craniosynostosis from their perspective. J. Craniofac. Surg. 2016, 27, 1510–1514. [Google Scholar] [CrossRef] [PubMed]
- Sandy, R.; Hennocq, Q.; Nysjö, J.; Giran, G.; Friess, M.; Khonsari, R.H. Orbital shape in intentional skull deformations and adult sagittal craniosynostoses. J. Anat. 2018. [Google Scholar] [CrossRef] [PubMed]
- Wall, S.A.; Thomas, G.P.; Johnson, D.; Byren, J.C.; Jayamohan, J.; Magdum, S.A.; McAuley, D.J.; Richards, P.G. The preoperative incidence of raised intracranial pressure in nonsyndromic sagittal craniosynostosis is underestimated in the literature. J. Neurosurg. Pediatr. 2014, 14, 674–681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, G.P.; Johnson, D.; Byren, J.C.; Judge, A.D.; Jayamohan, J.; Magdum, S.A.; Richards, P.G.; Wall, S.A. The incidence of raised intracranial pressure in nonsyndromic sagittal craniosynostosis following primary surgery. J. Neurosurg. Pediatr. 2015, 15, 350–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larysz, D.; Rożek, A. Incorrect structure of articulation organs and delayed speech development in children with non-syndromic craniosynostoses. Logop. Silesiana 2016, 5, 217–226. [Google Scholar]
- Larysz, D. Disorders of speech development in children with deformity of the skull. Logop. Silesiana 2012, 1, 47–60. [Google Scholar]
- Naran, S.; Miller, M.; Shakir, S.; Ware, B.; Camison, L.; Ford, M.; Goldstein, J.; Losee, J.E. Nonsyndromic craniosynostosis and associated abnormal speech and language development. Plast. Reconstr. Surg. 2017, 140, 62e–69e. [Google Scholar] [CrossRef] [PubMed]
- Chuang, C.; Rolison, M.; Yang, J.F.; Brooks, E.D.; Hashim, P.W.; Travieso, R.; Terner, J.; Steinbacher, D.M.; Landi, N.; Stavropoulos, K.K.M.; et al. Normalization of speech processing after whole-vault cranioplasty in sagittal synostosis. J. Craniofac. Surg. 2018, 29, 1132–1136. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, J.G.; Warren, S.M.; Bernstein, J.; Burnett, W.; Cunningham, M.L.; Edmond, J.C.; Figueroa, A.A.; Kapp-Simon, K.A.; Labow, B.I.; Peterson-Falzone, S.J.; et al. Craniosynostosis Working Group. Parameters of care for craniosynostosis. Cleft Palate Craniofac. J. 2012, 49 (Suppl. 1), 1–24. [Google Scholar] [CrossRef] [PubMed]
- Taylor, J.A.; Paliga, J.T.; Wes, A.M.; Tahiri, Y.; Goldstein, J.A.; Whitaker, L.A.; Bartlett, S.P. A critical evaluation of long-term aesthetic outcomes of fronto-orbital advancement and cranial vault remodeling in nonsyndromic unicoronal craniosynostosis. Plast. Reconstr. Surg. 2015, 135, 220–231. [Google Scholar] [CrossRef] [PubMed]
- Martini, M.; Klausing, A.; Messing-Jünger, M.; Lüchters, G. The self-defining axis of symmetry: A new method to determine optimal symmetry and its application and limitation in craniofacial surgery. J. Craniomaxillofac. Surg. 2017, 45, 1558–1565. [Google Scholar] [CrossRef] [PubMed]
- Care, H.; Dalton, L.; Johnson, D. The value of a photobook in informing families about the cosmetic results of surgery in craniosynostosis. J. Craniofac. Surg. 2018, 29, 88–91. [Google Scholar] [CrossRef] [PubMed]
- Wes, A.M.; Paliga, J.T.; Goldstein, J.A.; Whitaker, L.A.; Bartlett, S.P.; Taylor, J.A. An evaluation of complications, revisions, and long-term aesthetic outcomes in nonsyndromic metopic craniosynostosis. Plast. Reconstr. Surg. 2014, 133, 1453–1464. [Google Scholar] [CrossRef] [PubMed]
- Whitaker, L.A.; Bartlett, S.P.; Schut, L.; Bruce, D. Craniosynostosis: An analysis of the timing, treatment, and complications in 164 consecutive patients. Plast. Reconstr. Surg. 1987, 80, 195–212. [Google Scholar] [CrossRef] [PubMed]
- Kreppel, M.; Kauke, M.; Safi, A.F.; Grandoch, A.; Pocek-Behn, N.; Nickenig, H.J.; Zöller, J. Clinical evaluation of non-syndromic scaphocephaly surgically corrected with the procedure of total vertex craniectomy. J. Craniomaxillofac. Surg. 2018, 46, 1465–1469. [Google Scholar] [CrossRef] [PubMed]
- Burokas, L. Craniosynostosis: Caring for infants and their families. Crit. Care Nurse 2013, 33, 39–50. [Google Scholar] [CrossRef] [PubMed]
- Salokorpi, N.; Savolainen, T.; Sinikumpu, J.J.; Ylikontiola, L.; Sándor, G.K.; Pirttiniemi, P.; Serlo, W. Outcomes of 40 nonsyndromic sagittal craniosynostosis patients as adults: A case-control study with 26 years of postoperative follow-up. Oper. Neurosurg. 2018. [Google Scholar] [CrossRef] [PubMed]
- Wallace, E.R.; Collett, B.R.; Kapp-Simon, K.; Starr, J.R.; Birgfeld, C.; Speltz, M.L. Visuomotor function in school-age children with single-suture craniosynostosis. J. Dev. Behav. Pediatr. 2016, 37, 483–490. [Google Scholar] [CrossRef] [PubMed]
- Speltz, M.L.; Collett, B.R.; Wallace, E.R.; Kapp-Simon, K. Behavioral adjustment of school-age children with and without single-suture craniosynostosis. Plast. Reconstr. Surg. 2016, 138, 435–445. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parents’ Assessment | The Appearance of My Child’s Head | The Appearance of My Child’s Face | ||||||
|---|---|---|---|---|---|---|---|---|
| Before Surgery | After Surgery | Before Surgery | After Surgery | |||||
| n | % | n | % | n | % | n | % | |
| Did not differ from that of his/her peers | 3 | 1.4 | 77 | 36.7 | 57 | 27.0 | 145 | 68.7 |
| Was only slightly different from that of his/her peers | 19 | 9.0 | 82 | 39.0 | 47 | 22.3 | 36 | 17.1 |
| Was somewhat noticeable as abnormal | 67 | 31.9 | 40 | 19.0 | 45 | 21.3 | 15 | 7.1 |
| Was easily noticeable as abnormal | 66 | 31.4 | 4 | 1.9 | 38 | 18.0 | 8 | 3.8 |
| Was completely noticeable as abnormal | 55 | 26.2 | 7 | 3.3 | 24 | 11.4 | 7 | 3.3 |
| The Appearance of My Child’s Head | ||||||||
|---|---|---|---|---|---|---|---|---|
| Parents’ Assessment | Isolated Craniosynostoses | Syndromic Craniosynostoses | ||||||
| Before Surgery | After Surgery | Before Surgery | After Surgery | |||||
| n | % | n | % | n | % | n | % | |
| Did not differ from that of his/her peers | 1 | 1.0 | 35 | 36.8 | 2 | 6.3 | 8 | 25.0 |
| Was only slightly different from that of his/her peers | 10 | 10.4 | 45 | 47.4 | 1 | 3.1 | 11 | 34.4 |
| Was somewhat noticeable as abnormal | 28 | 29.2 | 15 | 15.8 | 8 | 25.0 | 8 | 25.0 |
| Was easily noticeable as abnormal | 35 | 36.5 | 0 | 0.0 | 10 | 31.3 | 2 | 6.3 |
| Was completely noticeable as abnormal | 22 | 22.9 | 0 | 0.0 | 11 | 34.4 | 3 | 9.4 |
| The Appearance of My Child’s Face | ||||||||
|---|---|---|---|---|---|---|---|---|
| Parents’ Assessment | Isolated Craniosynostoses | Syndromic Craniosynostoses | ||||||
| Before Surgery | After Surgery | Before Surgery | After Surgery | |||||
| n | % | n | % | n | % | n | % | |
| Did not differ from that of his/her peers | 22 | 22.9 | 70 | 72.9 | 8 | 25.0 | 16 | 50.0 |
| Was only slightly different from that of his/her peers | 27 | 28.1 | 22 | 22.9 | 3 | 9.4 | 6 | 18.8 |
| Was somewhat noticeable as abnormal | 19 | 19.8 | 4 | 4.2 | 7 | 21.9 | 3 | 9.4 |
| Was easily noticeable as abnormal | 21 | 21.9 | 0 | 0.0 | 6 | 18.8 | 3 | 9.4 |
| Was completely noticeable as abnormal | 7 | 7.1 | 0 | 0.0 | 8 | 25.0 | 4 | 12.5 |
| Parents’ Assessment | The Appearance of My Child’s Head | The Appearance of My Child’s Face | ||||
|---|---|---|---|---|---|---|
| ≤3 Years (%) | 4 Years (%) | ≥5 Years (%) | ≤3 Years (%) | 4 Years (%) | ≥5 Years (%) | |
| Did not differ from that of his/her peers | 25.6 | 43.6 | 38.6 | 64.0 | 69.1 | 65.9 |
| Was only slightly different from that of his/her peers | 45.3 | 32.7 | 31.8 | 18.6 | 18.2 | 20.5 |
| Was somewhat noticeable as abnormal | 19.8 | 20.0 | 25.0 | 9.3 | 7.3 | 6.8 |
| Was easily noticeable as abnormal | 2.3 | 1.8 | 2.3 | 4.7 | 1.8 | 2.3 |
| Was completely noticeable as abnormal | 5.8 | 1.8 | 2.3 | 3.5 | 3.6 | 4.5 |
| Parents’ Assessment | How Does Your Child Relate to Peers | How Does Your Child Relate to Adults | ||
|---|---|---|---|---|
| n | % | n | % | |
| Very easily | 87 | 41.4 | 70 | 33.3 |
| Rather easily | 94 | 44.8 | 114 | 54.3 |
| Hard to say | 19 | 9.0 | 17 | 8.1 |
| Not very well | 6 | 2.9 | 7 | 3.3 |
| Poorly | 4 | 1.9 | 2 | 1.0 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Larysz, D.; Nieroba, E. Subjective Assessment of Head and Facial Appearance in Children with Craniosynostoses after Surgical Treatment. Healthcare 2018, 6, 127. https://doi.org/10.3390/healthcare6040127
Larysz D, Nieroba E. Subjective Assessment of Head and Facial Appearance in Children with Craniosynostoses after Surgical Treatment. Healthcare. 2018; 6(4):127. https://doi.org/10.3390/healthcare6040127
Chicago/Turabian StyleLarysz, Dawid, and Elżbieta Nieroba. 2018. "Subjective Assessment of Head and Facial Appearance in Children with Craniosynostoses after Surgical Treatment" Healthcare 6, no. 4: 127. https://doi.org/10.3390/healthcare6040127