Development and Psychometric Properties of The Delayed Childbearing Questionnaire (DCBQ-55)

 , and
, and 
Abstract
:1. Introduction
2. Material and Methods
2.1. The Qualitative Phase
2.2. The Quantitative Phase
2.2.1. Initial Item Generation
2.2.2. Face Validity
2.2.3. Content Validity
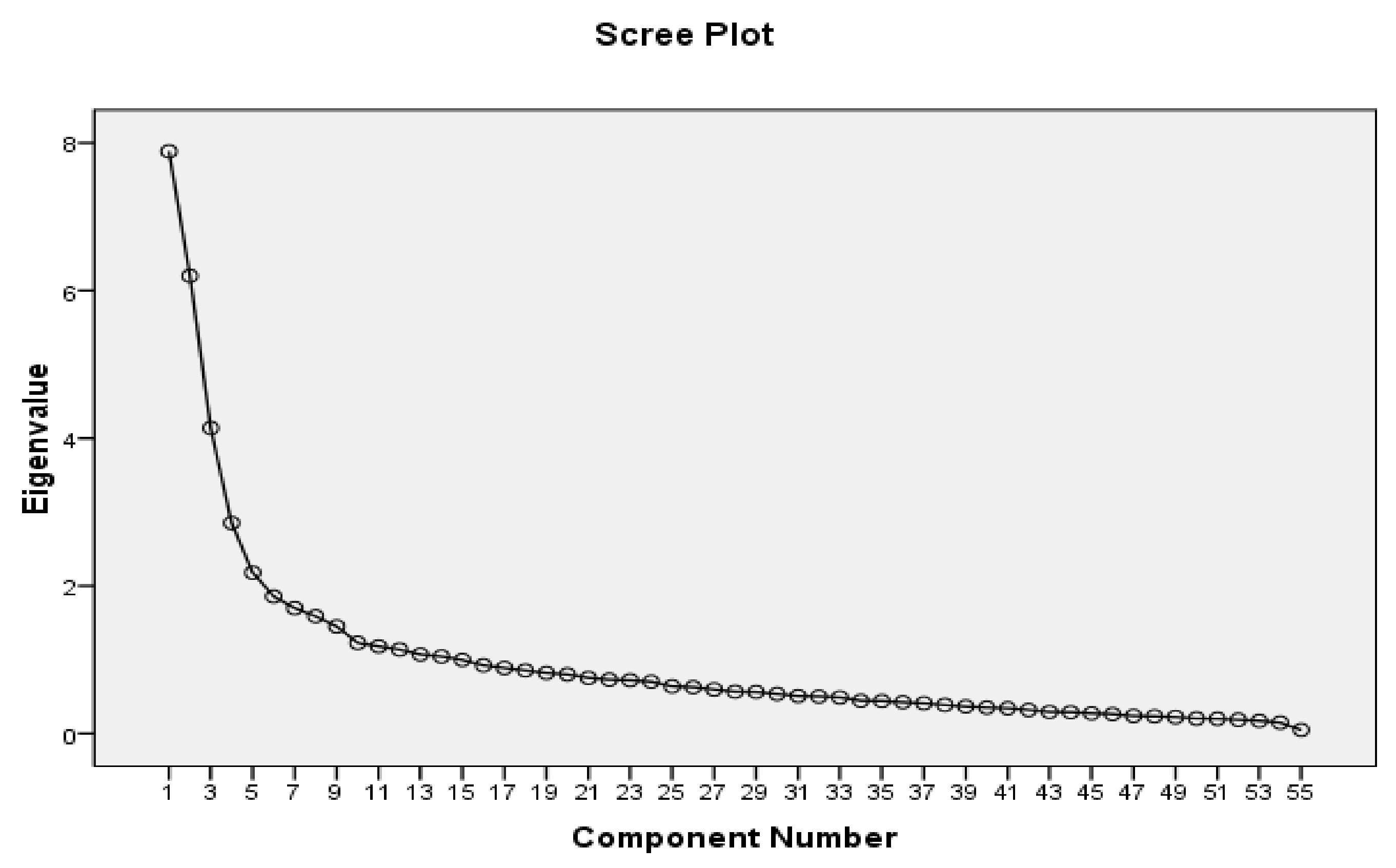
2.2.4. Construct Validity
2.2.5. Reliability
2.2.6. Statistical Analysis
2.3. Ethical Considerations
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Wiebe, E.; Chalmers, A.; Yager, H. Delayed motherhood: Understanding the experiences of women older than age 33 who are having abortions but plan to become mothers later. Can. Fam. Physician 2012, 58, e588–e595. [Google Scholar] [PubMed]
- Behboudi-Gandevani, S.; Ziaei, S.; Khalajabadi Farahani, F.; Jasper, M. The Perspectives of Iranian Women on Delayed Childbearing: A Qualitative Study. J. Nurs. Res. 2015, 23, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Balasch, J.; Gratacós, E. Delayed childbearing: Effects on fertility and the outcome of pregnancy. Curr. Opin. Obstet. Gynecol. 2012, 24, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Maheshwari, A.; Porter, M.; Shetty, A.; Bhattacharya, S. Women’s awareness and perceptions of delay in childbearing. Fertil. Steril. 2008, 90, 1036–1042. [Google Scholar] [CrossRef] [PubMed]
- Mills, M.; Rindfuss, R.R.; McDonald, P.; te Velde, E. Why do people postpone parenthood? Reasons and social policy incentives. Hum. Reprod. Update 2011, 17, 848–860. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Proudfoot, S.; Wellings, K.; Glasier, A. Analysis why nulliparous women over age 33 wish to use contraception. Contraception 2009, 79, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Sol Olafsdottir, H.; Wikland, M.; Möller, A. Reasoning about timing of wanting a child: A qualitative study of Nordic couples from fertility clinics. J. Reprod. Infant. Psychol. 2011, 29, 493–505. [Google Scholar] [CrossRef]
- Kenny, L.C.; Lavender, T.; McNamee, R.; O’Neill, S.; Mills, T.; Khashan, A.S. Advanced maternal age and adverse pregnancy outcome: Evidence from a large contemporary cohort. PLoS ONE 2013, 8, e56583. [Google Scholar] [CrossRef] [PubMed]
- Weng, Y.-H.; Yang, C.-Y.; Chiu, Y.-W. Risk assessment of adverse birth outcomes in relation to maternal age. PLoS ONE 2014, 9, e114843. [Google Scholar] [CrossRef] [PubMed]
- Petersen, K.B.; Hvidman, H.W.; Sylvest, R.; Pinborg, A.; Larsen, E.C.; Macklon, K.T.; Andersen, A.N.; Schmidt, L. Family intentions and personal considerations on postponing childbearing in childless cohabiting and single women aged 35–43 seeking fertility assessment and counselling. Hum. Reprod. 2015, 30, 2563–2574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varea, C.; Terán, J.M.; Bernis, C.; Bogin, B. The impact of delayed maternity on foetal growth in Spain: An assessment by population attributable fraction. Women Birth 2018, 31, e190–e196. [Google Scholar] [CrossRef] [PubMed]
- Asgharpour, M.; Villarreal, S.; Schummers, L.; Hutcheon, J.; Shaw, D.; Norman, W.V. Inter-pregnancy interval and pregnancy outcomes among women with delayed childbearing: Protocol for a systematic review. Syst. Rev. 2017, 6, 75. [Google Scholar] [CrossRef] [PubMed]
- Koert, E.; Daniluk, J.C. When time runs out: Reconciling permanent childlessness after delayed childbearing. J. Reprod. Infant Psychol. 2017, 35, 342–352. [Google Scholar] [CrossRef] [PubMed]
- Sylvest, R.; Koert, E.; Birch Petersen, K.; Malling, G.M.H.; Hald, F.; Nyboe Andersen, A.; Schmidt, L. Attitudes towards family formation among men attending fertility counselling. Reprod. Biomed. Soc. Online 2018, 6, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Adashi, E.Y.; Gutman, R. Delayed Childbearing as a Growing, Previously Unrecognized Contributor to the National Plural Birth Excess. Obstet. Gynecol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Te Velde, E.; Habbema, D.; Leridon, E.; Eijkemans, M. The effect of postponement of first motherhood on permanent involuntary childlessness and total fertility rate in six European countries since the 1970s. Hum. Reprod. 2012, 27, 1179–1183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sobotka, T. Post-transitional fertility: The role of childbearing postponement in fuelling the shift to low and unstable fertility levels. J. Biosoc. Sci. 2017, 49, S20–S45. [Google Scholar] [CrossRef] [PubMed]
- Eurostat Statistics Explained, Fertility Statistics. 2018. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php/Fertility_statistics (accessed on 15 September 2018).
- Saadat, S.; Chowdhury, S.; Mehryar, A. Fertility Decline in the Islamic Republic of Iran, 1980–2006: A Case Study. Available online: http://siteresources.worldbank.org/INTPRH/Resources/376374-1278599377733/Iran62910PRINT.pdf (accessed on 15 September 2018).
- Aghajanian, A. Family Planning Program and Recent Fertility Trends in Iran. Measure Evaluation, Carolina Population Center, University of North Carolina at Chapel Hill, March 1998. Available online: https://www.measureevaluation.org/resources/publications/wp-98-04 (accessed on 15 September 2018).
- McDonald, P.; Hosseini-Chavoshi, M.; Abbasi-Shavazi, M.J.; Rashidian, A. An assessment of recent Iranian fertility trends using parity progression ratios. Demogr. Res. 2015, 32, 1581–1602. [Google Scholar] [CrossRef] [Green Version]
- The Iran’s National Statistics Organization. Based on the Results of the Census of 2016, the Total Fertility Rate of Iran in the Period of 2012–2016 Reached to 2.01 Children. 2017. Available online: https://www.amar.org.ir/DesktopModules/DnnForge%20-%20NewsArticles/Print.aspx?tabid=123&tabmoduleid=507&articleId=5080&moduleId=613&PortalID=0 (accessed on 15 September 2018).
- Kazemijaliseh, H.; Tehrani, F.R.; Behboudi-Gandevani, S.; Hosseinpanah, F.; Khalili, D.; Azizi, F. The Prevalence and Causes of Primary Infertility in Iran: A Population-Based Study. Glob. J. Health Sci. 2015, 7, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Behboudi-Gandevani, S.; Ziaei, S.; Khalajabadi-Farahani, F.; Jasper, M. Iranian primigravid women’s awareness of the risks associated with delayed childbearing. Eur. J. Contracept. Reprod. Health Care 2013, 18, 460–467. [Google Scholar] [CrossRef] [PubMed]
- Nasrabad, H.B.R.; Abbasi-Shavazi, M.J.; Hosseini-Chavoshi, M.; Karegar-Shoraki, M.R. Trend and Patterns of Childlessness in Iran. In Proceedings of the XXVII International Population Conference of the IUSSP, Busan, Korea, 26–31 August 2013; Available online: https://iussp.org/sites/default/files/event_call_for_papers/Childlessness%20in%20Iran%20-%20draft.pdf (accessed on 15 September 2018).
- Shorey, S.; Yang, Y.Y.; Ang, E. The impact of negative childbirth experience on future reproductive decisions: A quantitative systematic review. J. Adv. Nurs. 2018, 74, 1236–1244. [Google Scholar] [CrossRef] [PubMed]
- Ivankova, N.V.; Creswell, J.W.; Stick, S.L. Using mixed-methods sequential explanatory design: From theory to practice. Field Methods 2006, 18, 3–20. [Google Scholar] [CrossRef]
- Graneheim, U.H.; Lundman, B. Qualitative content analysis in nursing research: Concepts, procedures and measures to achieve trustworthiness. Nurse. Educ. Today 2004, 24, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Vaismoradi, M.; Turunen, H.; Bondas, T. Content analysis and thematic analysis: Implications for conducting a qualitative descriptive study. Nurs. Health Sci. 2013, 15, 398–405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waltz, C.F.; Strickland, O.L.; Lenz, E.R. Measurement in Nursing and Health Research; Springer Publishing Company: New York, NY, USA, 2010. [Google Scholar]
- Munro, B.H. Statistical Methods for Health Care Research; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2005. [Google Scholar]
- Bland, J.M.; Altman, D.G. Statistics notes: Cronbach’s alpha. BMJ 1997, 314, 572. [Google Scholar] [CrossRef] [PubMed]
- Polit, D.F.; Beck, C.T. Essential of Nursing Research: Appraising Evidence for Nursing Practice; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2018. [Google Scholar]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed]
- Taheri, M.; Takian, A.; Taghizadeh, Z.; Jafari, N.; Sarafraz, N. Creating a positive perception of childbirth experience: Systematic review and meta-analysis of prenatal and intrapartum interventions. Reprod Health 2018, 15, 73. [Google Scholar] [CrossRef] [PubMed]
- Williams, K.; Sassler, S.; Frech, A.; Addo, F.; Cooksey, E. Nonmarital Childbearing, Union History, and Women’s Health at Midlife. Am. Sociol. Rev. 2011, 76, 465–486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liefbroer, A.C. Changes in Family Size Intentions Across Young Adulthood: A Life-Course Perspective. Eur. J. Popul. 2009, 25, 363–386. [Google Scholar] [CrossRef] [PubMed]
- Olusanya, B.O.; Solanke, O.A. Perinatal correlates of delayed childbearing in a developing country. Arch. Gynecol. Obstet. 2012, 285, 951–957. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, L.; Sobotka, T.; Bentzen, J.G.; Andersen, A.N.; ESHRE Reproduction and Society Task Force. Demographic and medical consequences of the postponement of parenthood. Hum. Reprod. Update 2012, 18, 29–43. [Google Scholar] [CrossRef] [PubMed]
- Sheinis, M.; Carpe, N.; Gold, S.; Selk, A. Ignorance is bliss: Women’s knowledge regarding age-related pregnancy risks. J. Obstet. Gynaecol. 2018, 38, 344–351. [Google Scholar] [CrossRef] [PubMed]
- Simoni, M.K.; Mu, L.; Collins, S.C. Women’s career priority is associated with attitudes towards family planning and ethical acceptance of reproductive technologies. Hum. Reprod. 2017, 32, 2069–2075. [Google Scholar] [CrossRef] [PubMed]
- Maeda, E.; Nakamura, F.; Boivin, J.; Kobayashi, Y.; Sugimori, H.; Saito, H. Fertility knowledge and the timing of first childbearing: A cross-sectional study in Japan. Hum. Fertil. 2016, 19, 275–281. [Google Scholar]
- Shah, M.A.; Shah, N.M.; Chowdhury, R.I.; Menon, I. Unmet need for contraception in Kuwait: Issues for health care providers. Soc. Sci. Med. 2004, 59, 1573–1580. [Google Scholar] [CrossRef] [PubMed]
- Simmonds, D.M.; West, L.; Porter, J.; Davies, M.; Holland, C.; Preston-Thomas, A.; O’Rourke, P.K.; Tangey, A. The role of support person for Ngaanyatjarra women during pregnancy and birth. Women Birth 2012, 25, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Arhin, A.O.; Cormier, E. Factors influencing decision-making regarding contraception and pregnancy among nursing students. Nurse Educ. Today 2008, 28, 210–217. [Google Scholar] [CrossRef] [PubMed]
- Allen, L.; Fountain, L. Addressing sexuality and pregnancy in childbirth education classes. J. Perinat. Educ. 2007, 16, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Jamali, S.; Mosalanejad, L. Sexual dysfnction in Iranian pregnant women. Iran. J. Reprod. Med. 2013, 11, 479–486. [Google Scholar] [PubMed]
- Moscrop, A. Can sex during pregnancy cause a miscarriage? A concise history of not knowing. Br. J. Gen. Pract. 2012, 62, e308–e310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andraweera, P.; Roberts, C.T.; Leemaqz, S.; McCowan, L.; Myers, J.; Kenny, L.C.; Walker, J.; Poston, L.; Dekker, G.; SCOPE Consortium. The duration of sexual relationship and its effects on adverse pregnancy outcomes. J. Reprod. Immunol. 2018, 128, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Mbekenga, C.K.; Pembe, A.B.; Darj, E.; Christensson, K.; Olsson, P. Prolonged sexual abstinence after childbirth: Gendered norms and perceived family health risks. Focus group discussions in a Tanzanian suburb. BMC Int. Health Hum. Rights 2013, 13, 4. [Google Scholar] [CrossRef] [Green Version]
- Cooke, A.; Mills, T.A.; Lavender, T. Advanced maternal age: Delayed childbearing is rarely a conscious choice. A qualitative study of women’s views and experiences. Int. J. Nurs. Stud. 2012, 49, 30–39. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Response (n = 300) |
|---|---|
| Age, mean (SD), y | 36.1 (8.2) |
| Marital age, mean (SD), y | 8.2 (3.9) |
| Husband’s age, mean (SD), y | 40.1 (5.7) |
| Education level, n (%) | |
| ≥High school graduate | 162 (54) |
| Bachelor’s degree | 90 (30) |
| Postgraduate | 48 (16) |
| Job status, n (%) | |
| Employed | 192 (64) |
| Unemployed | 108 (36) |
| Household income *, n (%) | |
| Poor | 54 (18) |
| Middle | 216 (72) |
| Well-off | 30 (10) |
| Items | Factor 1 | Factor 2 | Factor 3 | Factor 4 | Factor 5 | Factor 6 |
|---|---|---|---|---|---|---|
| Factor 1: Readiness for childbearing | ||||||
| Being sure about physical health before pregnancy | 0.821 | 0.471 | 0.017 | 0.067 | 0.074 | 0.017 |
| Control of chronic diseases before pregnancy | 0.819 | 0.215 | 0.063 | 0.084 | 0.051 | 0.036 |
| Having mental peace before pregnancy | 0.815 | 0.015 | 0.074 | 0.128 | 0.121 | 0.097 |
| Ability to transfer mental safety and security to the spouse before pregnancy | 0.798 | 0.122 | 0.005 | 0.014 | 0.224 | 0.215 |
| Having concerns about being a good mother and wife at the same time | 0.777 | 0.168 | 0.084 | 0.157 | 0.168 | 0.254 |
| Meeting the basic necessities before pregnancy | 0.763 | 0.101 | 0.054 | 0.108 | 0.185 | 0.135 |
| Having suitable financial savings before pregnancy | 0.755 | 0.020 | 0.035 | 0.114 | 0.117 | 0.136 |
| Having a suitable and secure job before pregnancy | 0.745 | 0.187 | 0.150 | 0.168 | 0.231 | 0.198 |
| Ability to provide the best facilities for childcare | 0.732 | 0.096 | 0.220 | .0164 | 0.226 | 0.146 |
| Completing education and studies before pregnancy | 0.703 | 0.124 | 0.221 | 0.064 | 0.117 | 0.318 |
| Having concerns about financial problems during pregnancy | 0.620 | 0.183 | 0.012 | 0.134 | 0.091 | 0.018 |
| Having concerns about losing better economic situations during pregnancy | 0.581 | 0.163 | 0.187 | 0.078 | 0.107 | 0.015 |
| Lack of responsibility and commitment to have a child | 0.506 | 0.043 | 0.024 | 0.093 | 0.208 | 0.147 |
| Lack of self-confidence to be a mother | 0.506 | 0.123 | 0.014 | 0.215 | 0.018 | 0.095 |
| High costs of pregnancy and childbirth | 0.319 | 0.106 | 0.054 | 0.197 | 0.064 | 0.031 |
| Factor 2: Stability in the partner relationship | ||||||
| Achieving a comprehensive understanding of the spouse before pregnancy | 0.33 | 0.860 | 0.214 | 0.057 | 0.163 | 0.069 |
| Being sure of the reliability of the spouse for the rest of life | 0.051 | 0.741 | 0.011 | 0.001 | 0.002 | 0.101 |
| Developing strong relationships with the spouse | 0.43 | 0.714 | 0.197 | 0.036 | 0.102 | 0.111 |
| Feeling concerns about the ability to have enjoyable sexual relationships during pregnancy | 0.33 | 0.707 | 0.72 | 0.128 | 0.114 | 0.022 |
| Feeling concerns about personal attractiveness during pregnancy | 0.87 | 0.686 | 0.233 | 0.043 | 0.210 | 0.185 |
| Necessity of having children to achieve peace and stability in life | 0.051 | 0.317 | 0.114 | 0.045 | 0.084 | 0.036 |
| Factor 3: Awareness about the adverse outcomes of pregnancy in advanced maternal age | ||||||
| Increased risk of infertility in women older than 35 years | 0.047 | 0.124 | 0.617 | 0.165 | 0.036 | 0.182 |
| Increased risk of obstetrics complications in advanced maternal age | 0.088 | 0.065 | 0.611 | 0.109 | 0.062 | 0.126 |
| Increased risk of neonatal complications in advanced maternal age | 0.047 | 0.125 | 0.524 | 0.068 | 0.085 | 0.051 |
| Presence of effective treatments for infertility to solve related problems | 0.091 | 0.054 | 0.454 | 1.25 | 0.150 | 0.055 |
| Losing the chance of having a second child due to delayed childbearing | 0.158 | 0.026 | 0.409 | 0.001 | 1.05 | 0.201 |
| Factor 4: Attitudes toward delayed childbearing | ||||||
| Possibility of having a child at any age without facing any problem if God willing | 0.103 | 0.156 | 0.048 | 0.667 | 0.114 | 0.165 |
| Completion of the woman’s identity through motherhood | 0.147 | 0.121 | 0.039 | 0.633 | 0.065 | 0.195 |
| Giving a meaning to the life through having a child | 0.031 | 0.114 | 0.094 | 0.591 | 0.069 | 0.168 |
| Importance of bringing a male or female child | 0.085 | 0.032 | 0.129 | 0.588 | 0.142 | 0.024 |
| Delayed childbearing as an interference in God’s affairs | 0.044 | 0.052 | 0.152 | 0.580 | 0.063 | 0.065 |
| Creating a balance in the family decision-making between man and woman by delayed childbearing | 0.163 | 0.098 | 0.231 | 0.572 | 0.117 | 0.096 |
| Reduction of the women’s power in the family due to early childbearing | 0.047 | 0.187 | 0.011 | 0.570 | 0.016 | 0.048 |
| Sufficiency of having only one child for the family | 0.214 | 0.025 | 0.053 | 0.545 | 0.021 | 0.057 |
| Starting a family later in life due to marriage at the old age | 0.001 | 0.064 | 0.121 | 0.454 | 0.133 | 0.045 |
| Factor 5: Family support | ||||||
| Being under pressure by the couple’s families for delayed childbearing | 0.062 | 0.147 | 0.036 | 0.080 | 0.656 | 0.037 |
| Getting help from the couple’s families for taking care of the child | 0.142 | 0.015 | 0.199 | 0.142 | 0.614 | 0.091 |
| Successful experiences of delayed childbearing in the couple’s families | 0.070 | 0.088 | 0.078 | 0.058 | 0.602 | 0.158 |
| Persuasion of the couple to delay childbearing due to being raised in a small paternal family | 0.018 | 0.011 | 0.148 | 0.046 | 0.581 | 0.036 |
| Factor 6: Social support | ||||||
| Childbearing as one of the most important social functions of the family | 0.091 | 0.044 | 0.015 | 0.190 | 0.247 | 0.701 |
| Being encouraged by others to delay childbearing | 0.035 | 0.088 | 0.107 | 0.047 | 0.675 | 0.692 |
| Limitations in the freedom for getting engaged in social activities due to childbearing | 0.125 | 0.121 | 0.044 | 0.013 | 0.214 | 0.671 |
| Delayed childbearing as a sign of modernity | 0.017 | 0.014 | 0.125 | 0.166 | 0.118 | 0.657 |
| Popularity of early childbearing in families with a lower social status | 0.094 | 0.055 | 0.087 | 0.122 | 0.147 | 0.649 |
| Education regarding delayed childbearing in schools and universities | 0.225 | 0.024 | 0.096 | 0.085 | 0.129 | 0.629 |
| Free access to modern contraceptive methods | 0.019 | 0.035 | 0.067 | 0.101 | 0.155 | 0.625 |
| Lack of childcare facilities at the workplace | 0.195 | 0.128 | 0.088 | 0.032 | 0.138 | 0.624 |
| Giving the responsibility of child care to a nursery with confidence | 0.109 | 0.165 | 0.036 | 0.080 | 0.091 | 0.590 |
| The high cost of childcare in a nursery | 0.068 | 0.135 | 0.166 | 0.063 | 0.050 | 0.581 |
| The short period of maternity leave for employed mothers | 0.36 | 0.100 | 0.109 | 0.085 | 0.075 | 0.570 |
| Support of delayed childbearing in mass media | 0.015 | 0.121 | 0.094 | 0.021 | 0.150 | 0.564 |
| Lack of special laws to support pregnant women or mothers | 0.190 | 0.134 | 0.096 | 0.048 | 0.021 | 0.562 |
| Being fired from work due to getting pregnant | 0.087 | 0.087 | 0.148 | 0.046 | 0.107 | 0.513 |
| Threating the child due to social insecurity | 0.046 | 0.050 | 0.018 | 0.080 | 0.075 | 0.507 |
| Lack of a bright future to start a family | 0.011 | 0.010 | 0.115 | 0.198 | 0.114 | 0.481 |
| Domain | Item (Number) | Cronbach’s Alpha | ICC (95% CI) | Spearman’s Correlation Coefficient (n = 25) | p-Value |
|---|---|---|---|---|---|
| Readiness for childbearing | 15 | 0.833 | 0.83 (0.81–0.87) | 0.71 | 0.001 |
| Stability in the partner relationship | 6 | 0.735 | 0.69 (0.67–0.74) | 0.91 | 0.001 |
| Awareness about the adverse outcomes of pregnancy in advanced maternal age | 5 | 0.844 | 0.83 (0.80–0.88) | 0.85 | 0.001 |
| Attitude toward delayed childbearing | 9 | 0.839 | 0.82 (0.79–0.89) | 0.96 | 0.001 |
| Family support | 4 | 0.830 | 0.83 (0.79–0.85) | 0.91 | 0.001 |
| Social support | 16 | 0.815 | 0.70 (0.68–0.84) | 0.86 | 0.001 |
| Total | 55 | 0.836 | 0.81 (0.79–0.86) | 0.86 | 0.001 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Behboudi-Gandevani, S.; Ziaei, S.; Kazemnejad, A.; Khalajabadi Farahani, F.; Vaismoradi, M. Development and Psychometric Properties of The Delayed Childbearing Questionnaire (DCBQ-55). Healthcare 2018, 6, 120. https://doi.org/10.3390/healthcare6040120
Behboudi-Gandevani S, Ziaei S, Kazemnejad A, Khalajabadi Farahani F, Vaismoradi M. Development and Psychometric Properties of The Delayed Childbearing Questionnaire (DCBQ-55). Healthcare. 2018; 6(4):120. https://doi.org/10.3390/healthcare6040120
Chicago/Turabian StyleBehboudi-Gandevani, Samira, Saeideh Ziaei, Anoshirvan Kazemnejad, Farideh Khalajabadi Farahani, and Mojtaba Vaismoradi. 2018. "Development and Psychometric Properties of The Delayed Childbearing Questionnaire (DCBQ-55)" Healthcare 6, no. 4: 120. https://doi.org/10.3390/healthcare6040120