
Gait Compensation among Children with Non-Operative Legg–Calvé–Perthes Disease: A Systematic Review

Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Selection Criteria
2.3. Data Extraction
2.4. Methodological Quality
2.5. Analysis
3. Results
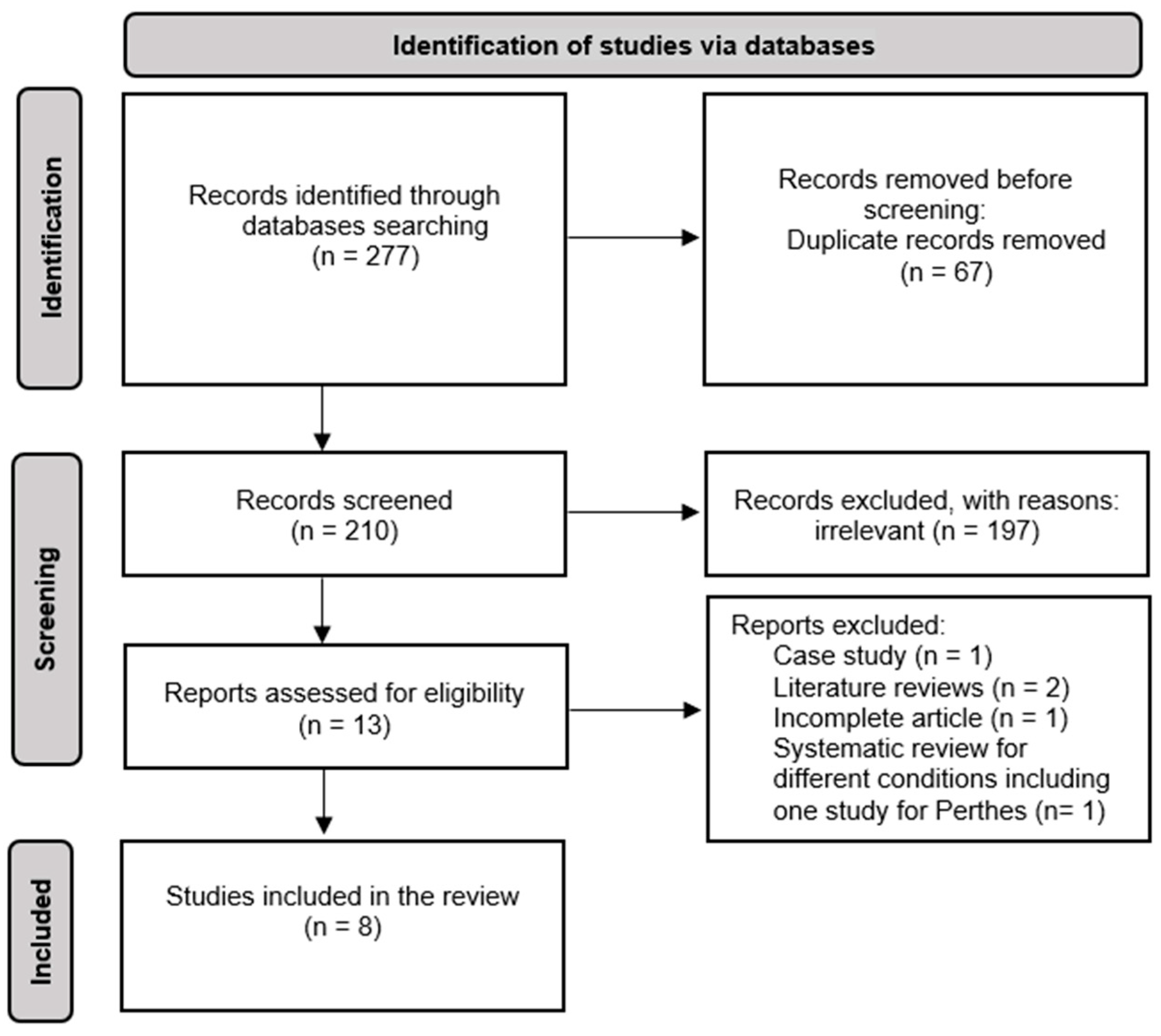
3.1. Selection of Studies
3.2. Methodological Quality
3.3. Methodological Data
4. Discussion
4.1. Biomechanical Gait Consideration
4.2. Identification and Interpretation of Compensatory Movement
4.2.1. Temporospatial Outcome Measures
4.2.2. Kinematic Outcome Measures
4.2.3. Kinetic Parameters
5. Clinical Implications
6. Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| 1 | Keywords | [Perthes [or] Necrosis [or] Hip Pathology] and [Non-Operative [or] Non-Surgical] |
|---|---|---|
| 2 | Keywords | Three-dimension motion analysis [or] two-dimensional movement analysis [or] gait analysis [or] walk * [or] locomotion [or] ambulation [or] mobility |
| 3 | Keywords | Compensate * [or] adapt * [or] deviate * [or] variation [or] alter * [or] change * |
| 4 | Keywords | kinematic * [or] kinetic * [or] spatiotemporal [or] spatio-temporal [or] angle * [or] torque * [or] moment * [or] GRF [or] ground reaction force * |
| 5 | Combine | 1 [and] 2 [and] 3 [and] 4 |
Appendix B
| Reporting | Score | |
|---|---|---|
| (1) Is the hypothesis/aim/objective of the study clearly described? | Yes No | 1 0 |
| (2) Are the main outcome variables to be measured clearly described in the Introduction or Methods section? If the main outcomes are first mentioned in the Results section, the question should be answered “No”. | Yes No | 1 0 |
| (3) Are the characteristics of the patients included in the study clearly described? For patients: inclusion and/or exclusion criteria or case definition as well as a description of pathology/problem. Controls: short characteristics description, e.g., “healthy normal controls without previous injuries”. | Yes No | 1 0 |
| (4) Are the distributions of principal confounders in each group of subjects to be compared clearly described? A list of principal confounders is provided. Principal confounders include age, sex, height, and weight. | Yes Partially No | 2 1 0 |
| (5) Are measurement devices and data analysis procedures clearly stated? The type of device and resolution as well as the placement of the markers (model or exact placement) should be described. | Yes Partially No | 2 1 0 |
| (6) Are the main findings of the study clearly described? Simple outcome data (including denominators and numerators) should be reported for all major findings so that the reader can check the major analyses and conclusions. (This question does not cover statistical tests, which are considered below). | Yes No | 1 0 |
| (7) Does the study provide estimates of the random variability in the data for the main outcomes? In non-normally distributed data, the inter-quartile range of results should be reported. In normally distributed data, the standard error, standard deviation, or confidence intervals should be reported. If the distribution of the data is not described, it must be assumed that the estimates used were appropriate and the question should be answered “Yes”. | Yes No | 1 0 |
| (8) Have actual probability values been reported (e.g., 0.035 rather than <0.05) for the main outcomes, except where the probability value is less than 0.001? | Yes No | 1 0 |
| External validity | ||
| (9) Were the subjects asked to participate in the study representative of the entire population from which they were recruited? The study must identify the source population for patients and describe how the patients were selected. Patients would be representative if they comprised the entire source population, an unselected sample of consecutive patients, or a random sample. Random sampling is only feasible where a list of all members of the relevant population exists. Where a study does not report the proportion of the source population from which the patients are derived, the question should be answered “Unable to determine”. | Yes No Unable to determine | 1 0 U |
| (10) Were those subjects who were prepared to participate representative of the entire population from which they were recruited? The proportion of those asked who agreed should be stated. Validation that the sample was representative would include demonstrating that the distribution of the main confounding factors was the same in the study sample and the source population. | Yes No Unable to determine | 1 0 U |
| (11) Were the staff, places, and facilities optimal for the measurements? If the measurements took place in a laboratory, it can be assumed that the staff of the laboratory performed the measurements, and the question should be answered “Yes”. | Yes No Unable to determine | 1 0 U |
| Internal validity—bias | ||
| (12) If any of the results of the study were based on “data dredging”, was this made clear? Any analyses that had not been planned at the outset of the study should be clearly indicated. If no retrospective unplanned subgroup analyses were reported, then answer “Yes”. | Yes No Unable to determine | 1 0 U |
| (13) Were the statistical tests used to assess the main outcomes appropriate? The statistical techniques used must be appropriate to the data. For example, non-parametric methods should be used for small sample sizes. Where little statistical analysis has been undertaken but where there is no evidence of bias, the question should be answered “Yes”. If the distribution of the data (normal or not) is not described, it must be assumed that the estimates used were appropriate and the question should be answered “Yes”. | Yes No Unable to determine | 1 0 U |
| (14) Were the main outcome measures used accurate (valid and reliable)? For studies where the outcome measures are clearly described, the question should be answered “Yes”. For studies that refer to other work or that demonstrate that the outcome measures are accurate, the question should be answered “Yes”. | Yes No Unable to determine | 1 0 U |
| Internal validity—confounding (selection bias) | ||
| (15) Was there adequate adjustment for confounding factors in the analyses from which the main findings were drawn? If the effect of the main confounders was not investigated or confounding factors was demonstrated but no adjustment was made (e.g., kinetic values normalised to body weight or height etc.) in the final analyses, the question should be answered “No”. | Yes No Unable to determine | 1 0 U |
| (16) Were losses of patients to data contamination taken into account? If the number of patients lost to data contamination is not reported, the question should be answered “Unable to determine”. If the proportion lost to data contamination was too small to affect the main findings, the question should be answered “Yes”. | Yes No Unable to determine | 1 0 U |
| Power | ||
| (17) Did the study have sufficient power to detect a clinically important effect where the probability value for a difference being due to chance is less than 5%? | No power analysis done or power < 70% Power 70–80% Power > 80% | 0 1 2 |
| Total available score | 20 | |
References
- Krauspe, R.; Orthopade, P.R. Morbus Perthes; Springer Science and Media: Berlin, Germany, 1997; pp. 289–302. [Google Scholar]
- Nelitz, M.; Lippacher, S.; Krauspe, R.; Reichel, H. Morbus Perthes: Diagnostische Und Therapeutische Prinzipien. Dtsch. Arztebl. 2009, 106, 517–523. [Google Scholar] [CrossRef]
- Karimi, M.T.; Gutierrez-Farewik, L.; McGarry, A. Evaluation of the Hip Joint Contact Force in Subjects with Perthes Based on OpenSIM. Med. Eng. Phys. 2019, 67, 44–48. [Google Scholar] [CrossRef]
- Westhoff, B.; Martiny, F.; Reith, A.; Willers, R.; Krauspe, R.R.; Petermann, A.; Hirsch, M.A.; Willers, R.; Krauspe, R.R. Computerized Gait Analysis in Legg Calve Perthes Disease--Analysis of the Frontal Plane. Gait Posture 2006, 24, 196–202. [Google Scholar] [CrossRef]
- Svehlik, M.; Kraus, T.; Steinwender, G.; Zwick, E.B.; Linhart, W.E.; Švehlík, M.; Kraus, T.; Steinwender, G.; Zwick, E.B.; Linhart, W.E.; et al. Pathological Gait in Children with Legg-Calve-Perthes Disease and Proposal for Gait Modification to Decrease the Hip Joint Loading. Int. Orthop. 2012, 36, 1235–1241. [Google Scholar] [CrossRef] [PubMed]
- Stief, F.; Böhm, H.; Ebert, C.; Döderlein, L.; Meurer, A. Effect of Compensatory Trunk Movements on Knee and Hip Joint Loading during Gait in Children with Different Orthopedic Pathologies. Gait Posture 2014, 39, 859–864. [Google Scholar] [CrossRef]
- Westhoff, B.; Martiny, F.; Reith, A.; Willers, R.; Krauspe, R. Computerized Gait Analysis in Legg–Calvé–Perthes Disease—Analysis of the Sagittal Plane. Gait Posture 2012, 35, 541–546. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372. [Google Scholar] [CrossRef]
- Godin, K.; Stapleton, J.; Kirkpatrick, S.I.; Hanning, R.M.; Leatherdale, S.T. Applying Systematic Review Search Methods to the Grey Literature: A Case Study Examining Guidelines for School-Based Breakfast Programs in Canada. Syst. Rev. 2015, 4, 138. [Google Scholar] [CrossRef] [PubMed]
- Downs, S.H.; Black, N. The Feasibility of Creating a Checklist for the Assessment of the Methodological Quality Both of Randomised and Non-Randomised Studies of Health Care Interventions. J. Epidemiol. Community Health (1978) 1998, 52, 377–384. [Google Scholar] [CrossRef]
- Schmid, S.; Schweizer, K.; Romkes, J.; Lorenzetti, S.; Brunner, R. Secondary Gait Deviations in Patients with and without Neurological Involvement: A Systematic Review. Gait Posture 2013, 480–493. [Google Scholar] [CrossRef]
- Alle, L.; Armand, S.; Golay, A.; Monnin, D.; de Bie, R.A.; de Bruin, E.D. Gait Characteristics of Diabetic Patients: A Systematic Review. Diabetes Metab. Res. Rev. 2008, 24, 173–191. [Google Scholar] [CrossRef] [PubMed]
- Gouda, M.A. Common Pitfalls in Reporting the Use of SPSS Software. In Medical Principles and Practice; S. Karger AG: Basel, Switzerland, 2015; p. 300. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The Measurement of Observer Agreement for Categorical Data. Biometrics 1977, 33, 159. [Google Scholar] [CrossRef]
- Yoo, W.J.; Choi, I.H.; Cho, T.-J.; Chung, C.Y.; Park, M.S.; Lee, D.Y. Out-Toeing and in-Toeing in Patients with Perthes Disease: Role of the Femoral Hump. J. Pediatr. Orthop. 2008, 28, 717–722. [Google Scholar] [CrossRef] [PubMed]
- Stief, F.; Schmidt, A.; Adolf, S.; Kremer, L.; Brkic, M.; Meurer, A. Development of Gait Performance and Dynamic Hip and Knee Joint Loading after Containment Improving Surgery in Patients with Legg-Calvé-Perthes Disease. Gait Posture 2016, 47, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Stevens, W.R.; Podeszwa, D.A.; Tulchin-Francis, K. Compensatory Sagittal Plane Ankle Gait Mechanics: Are They Present in Patients with a Weak or Stiff Hip? Gait Posture 2019, 74, 250–254. [Google Scholar] [CrossRef] [PubMed]
- Wagenaar, R.C.; van Emmerik, R.E.A. Dynamics of Pathological Gait. Hum. Mov. Sci. 1994, 13, 441–471. [Google Scholar] [CrossRef]
- van der Linden, M.L.; Kerr, A.M.; Hazlewood, M.E.; Hillman, S.J.; Robb, J.E. Kinematic and Kinetic Gait Characteristics of Normal Children Walking at a Range of Clinically Relevant Speeds. J. Pediatr. Orthop. 2002, 22, 800–806. [Google Scholar] [CrossRef] [PubMed]
- Arnold, A.S.; Schwartz, M.H.; Thelen, D.G.; Delp, S.L. Contributions of Muscles to Terminal-Swing Knee Motions Vary with Walking Speed. J. Biomech. 2007, 40, 3660–3671. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, M.H.; Rozumalski, A.; Trost, J.P. The Effect of Walking Speed on the Gait of Typically Developing Children. J. Biomech. 2008, 41, 1639–1650. [Google Scholar] [CrossRef]
- Murley, G.S.; Landorf, K.B.; Menz, H.B.; Bird, A.R. Effect of Foot Posture, Foot Orthoses and Footwear on Lower Limb Muscle Activity during Walking and Running: A Systematic Review. Gait Posture 2009, 29, 172–187. [Google Scholar] [CrossRef]
- Radzimski, A.O.; Mündermann, A.; Sole, G. Effect of Footwear on the External Knee Adduction Moment—A Systematic Review. Knee 2012, 19, 163–175. [Google Scholar] [CrossRef]
- Hailer, Y.D.; Montgomery, S.; Ekbom, A.; Nilsson, O.; Bahmanyar, S. Legg-Calvé-Perthes Disease and the Risk of Injuries Requiring Hospitalization. Acta Orthop. 2012, 83, 572–576. [Google Scholar] [CrossRef]
- Karimi, M.; Esrafilian, A. Evaluation of the Stability of Normal Subjects and Patients with Perthes and Spinal Cord Injury Disorders during Short and Long Periods of Time. In Prosthetics and Orthotics International; SAGE Publications Ltd.: New York, NY, USA, 2013; Volume 37, pp. 22–29. [Google Scholar] [CrossRef]
- van der Krogt, M.M.M.M.; Sloot, L.H.L.H.; Harlaar, J. Overground versus Self-Paced Treadmill Walking in a Virtual Environment in Children with Cerebral Palsy. Gait Posture 2014, 40, 587–593. [Google Scholar] [CrossRef]
- Lin, X.; Meijer, O.G.; Lin, J.; Wu, W.; Lin, X.; Liang, B.; Van Dieën, J.H.; Bruijn, S.M. Frontal Plane Kinematics in Walking with Moderate Hip Osteoarthritis: Stability and Fall Risk. Clin. Biomech. 2015, 30, 874–880. [Google Scholar] [CrossRef]
- Tracy, J.B.; Petersen, D.A.; Pigman, J.; Conner, B.C.; Wright, H.G.; Modlesky, C.M.; Miller, F.; Johnson, C.L.; Crenshaw, J.R. Dynamic Stability during Walking in Children with and without Cerebral Palsy. Gait Posture 2019, 72, 182–187. [Google Scholar] [CrossRef]
- Frigo, C.; Bardare, M.; Corona, F.; Casnaghi, D.; Cimaz, R.; Naj Fovino, P.L.; Pedotti, A. Gait Alteration in Patients with Juvenile Chronic Arthritis: A Computerized Analysis. J. Orthop. Rheumatol. 1996, 9, 82–90. [Google Scholar]
- Krautwurst, B.K.; Wolf, S.I.; Heitzmann, D.W.W.; Gantz, S.; Braatz, F.; Dreher, T. The Influence of Hip Abductor Weakness on Frontal Plane Motion of the Trunk and Pelvis in Patients with Cerebral Palsy. Res. Dev. Disabil. 2013, 34, 1198–1203. [Google Scholar] [CrossRef]
- Sharma, L.; Lou, C.; Cahue, S.; Dunlop, D.D. The Mechanism of the Effect of Obesity in Knee Osteoarthritis: The Mediating Role of Malalignment. Arthritis. Rheum. 2000, 43, 568. [Google Scholar] [CrossRef]
- Williams, J.J.; Graham, G.P.; Dunne, K.B.; Menelaus, M.B. Late Knee Problems in Myelomeningocele. J. Pediatr. Orthop. 1993, 13, 701–703. [Google Scholar] [CrossRef]
- Horsak, B.; Schwab, C.; Baca, A.; Greber-Platzer, S.; Kreissl, A.; Nehrer, S.; Keilani, M.; Crevenna, R.; Kranzl, A.; Wondrasch, B. Effects of a Lower Extremity Exercise Program on Gait Biomechanics and Clinical Outcomes in Children and Adolescents with Obesity: A Randomized Controlled Trial. Gait Posture 2019, 70, 122–129. [Google Scholar] [CrossRef]
- Derrick, T.R.; van den Bogert, A.J.; Cereatti, A.; Dumas, R.; Fantozzi, S.; Leardini, A. ISB Recommendations on the Reporting of Intersegmental Forces and Moments during Human Motion Analysis. J. Biomech. 2020, 99, 109533. [Google Scholar] [CrossRef]

| Category | Inclusion | Exclusion |
|---|---|---|
| Type of Study | Published in peer-reviewed scientific journals in the English language | Reviews, conference papers, abstracts, letters, cases series, and pilot studies |
| Main Outcomes | Clearly identified gait data; data had to be retrieved from skin-mounted markers by means of at least two-dimensional kinematic data | Single video data without markers |
| Subjects | Human cohorts presenting non-operative children with Perthes gait pattern aged between 5 to 12 years | Individuals with musculoskeletal impairment or surgery in the lower limb, individuals with a neurological impairment such as cerebral palsy or Down’s syndrome (due to complex cognitive impairments). |
| Measurement Conditions | Walking on level ground or treadmills with a smooth surface and without any obstacles | Stair climbing, walking uphill or downhill, and walking on uneven ground or a slippery surface |
| Walking Characteristics | Subjects walked freely without any kind of walking aid at either normal (self-selected), fast, slow, or default (e.g., paced) gait speed and either barefoot or in normal footwear (e.g., flat-heeled shoes) | Running studies with special footwear |
| Author | Reporting | External Validity | Internal Validity (Bias) | Internal Validity (Confounding) | Power | Total Score | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| R.A. | M.S.A. | R.A. | M.S.A. | R.A. | M.S.A. | R.A. | M.S.A. | R.A. | M.S.A. | R.A. | M.S.A. | |
| 1. [4] | 9 | 9 | 1 | 1 | 3 | 3 | 2 | 2 | 0 | 0 | 15 | 15 |
| 2. [15] | 7 | 7 | 1 | 1 | 2 | 2 | 2 | 2 | 0 | 0 | 12 | 12 |
| 3. [5] | 9 | 9 | 2 | 2 | 2 | 2 | 2 | 2 | 0 | 0 | 15 | 15 |
| 4. [7] | 9 | 9 | 1 | 1 | 3 | 3 | 1 | 1 | 0 | 0 | 14 | 14 |
| 5. [6] | 10 | 10 | 2 | 2 | 2 | 2 | 2 | 2 | 0 | 0 | 16 | 16 |
| 6. [16] | 10 | 10 | 3 | 2 | 2 | 2 | 2 | 2 | 0 | 0 | 17 | 16 |
| 7. [17] | 10 | 10 | 2 | 2 | 2 | 2 | 2 | 2 | 0 | 0 | 16 | 16 |
| 8. [3] | 10 | 10 | 1 | 1 | 3 | 2 | 2 | 2 | 0 | 0 | 16 | 15 |
| Total Mean (SD) | 9.25 (1) | 1.5 (0.6) | 2.3 (0.4) | 1.8 (0.3) | 0 | 15 (1.4) | ||||||
| Study | Diagnosis | Number of Subjects (Gender) C: Control. P: Perthes | Age (Years) Mean (SD) | Parameters Evaluated | Joints Evaluated | Outcome Parameters | Perthes Mean (SD) | Control Mean (SD) | p-Value | |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. [4] | A diagnosis of Perthes with unilateral involvement was confirmed on radiographs. |
C: 30 (14 boys and 16 girls)
P: 33 (24 boys and 9 girls) |
C: 8.1 (1.2)
P: 8.0 (2.0) | Temporospatial, kinematic and kinetic | Thoracic, spinal, pelvic, and hip | Gait speed (m/s) Stride length (m) Stance phase (s) At single-limb stance Thorax obliquity° Pelvic obliquity° Hip adduction° Hip abd moment (Nm/kg) | 1.08 (0.19) 0.74 (0.07) 59 (2.2) Type 1–Type 2 −4.3 (5.7)–−5 (1.9) 4.3 (3.2)–0.2 (2.7) 9.4 (1.7)–1.1 (3.2) 0.43 (0.1)–0.24 (0.1) | 1.18 (0.18) 0.8 (0.06) 58.3 (1.2) −0.8 (1) 1.5 (1.1) 4.9 (2.9) 0.40 (0.08) | p = 0.045 p = 0.001 p = 1.18 | |
| 2. [15] | A 3D CT of the hip along with 3D gait analysis was performed to diagnose Perthes disease. |
P, out-toeing: 5
P, in-toeing: 4 (7 boys and 2 girls) |
P:11; range
7.0–15.3 years. | Kinematic | Pelvic and hip | At midstance phase Pelvic obliquity° Pelvis rotation° Hip flex/ext° Hip add/abd° Hip rotation° | Out-toeing Affected–Non-affected −3.3 (2.6)–−4.5 (4.4) 7 (5.6)–−13.8 (4.2) 10 (7.3)–7.8 (5.9) 2.5 (2.9)–3.5 (2.5) −10 (0)–3 (2.5) | In-toeing Affected_Non-affected −7.5 (3.5)–5.5 (1.9) −3.8 (2.9)–4 (3.9) 17.8 (6.8)–11.5 (6.2) 2.3 (3.6)–9 (±2.7) 12.5 (7.7)–1.5 (0.8) | ||
| 3. [5] | Diagnosis of Perthes disease was confirmed by X-ray. | C: 10 | 8.3 | Temporospatial, kinematic, and kinetic | Pelvic, hip, Knee, and ankle |
Gait speed (m/s)
Stride length (m) Stride time (s) Cadence (steps/min) At single-limb stance Hip abduction ° Hip rotation ° Pelvic obliquity ° Hip abd moment (Nm/kg) | Overloading 1.65 (4) 0.93 (0.12) 1.02 (0.45) 130.1 (34.03) 5.96 (2.03) −3.54 (7.93) 2.39 (3.13) 22.5 (3.94) | Normloading 1.94 (3) 1.01 (0.16) 0.87 (0.07) 138.8 (12.67) 1.76 (3.6) −5.69 (8.21) −1.3 (3.63) 11.87 (2.23) | Unloading 2.07 (0.26) 1.05 (0.16) 0.85 (0.12) 144 (20.7) −1.8 (4.13) −12.8 (9.9) −2.22 (2.8) 3.72 (4.57) | Control 2.06 (0.3) 1.09 (0.11) 0.90 (0.12) 136.6 (15) 3.99 (2.35) −4.91(6.57) 1.5 (1.87) 12.6 (3.87) |
| P: hip overloading 8 boys | 11.4 | |||||||||
|
P: hip normloading 19
(16 boys) | 6.5 | |||||||||
|
P: hip unloading 13
(11 boys) | 7.6 | |||||||||
| 4. [7] | Perthes disease with unilateral involvement was diagnosed and confirmed by radiograph. |
C: 30 (14 boys and 16 girls)
P: 49 (38 boys and 11 girls) Group 1, florid: 36 Group 2, advanced: 13 |
C: 8.1 (1.2)
P: 7.8 (2.3) | Kinematic and kinetic | Thoracic, spinal, pelvic, hip, knee, and ankle | Thorax ROM ° Pelvis ROM ° Hip ROM ° (florid) Knee ROM ° (florid) Hip positive work Hip negative work Knee positive work Knee negative work Ankle positive work Ankle negative work | Group 1–Group 2 4.4 (2.4)–3.4 (0.9) 6.2 (3.2)–3.5 (2.2) Affected–Non-affected 33.2 (9.2)–49 (6.7) 50.7 (7.1)–55.7 (5.6) 0.06 (0.03)–0.2 (0.09) 0.1 (0.06)–0.18 (0.1) 0.05 (0.05)–0.08 (0.06) 0.13 (0.07)–0.18 (0.10) 0.24 (0.09)–0.27 (0.09) 0.13 (0.05)–0.12 (0.04) | Control 3.2 (0.9) 2 (0.8) 44.5 (3.7) 55.7 (4.8) 0.15 (0.07) 0.15 (0.07) 0.06 (0.07) 0.18 (0.06) 0.28 (0.06) 0.13 (0.03) | Group1–control p = 0.018 p = 0.001 p = 0.001 p = 0.001 p = 0.001 p = 0.03 p = 0.636 p = 0.014 p = 0.052 p= 0.558 | |
| 5. [6] | Children with ipsilateral trunk lean, including children with Perthes, were observed in two gait laboratories. |
C: 20 (11 boys and 9 girls)
P: 27 (19 boys and 8 girls) Group 1, natural ipsilateral trunk lean (NTL): 19 Group 2, excessive ipsilateral trunk lean (ETL): 8 |
C: 9.3 (2.3)
P: 6.1 (1.8) | Temporospatial, kinematic, and kinetic | Thoracic, pelvic, hip, knee, and foot | Gait speed (m/s) Thorax max obliquity ° Pelvis max obliquity ° Foot rotation ° Hip add moment (Nm/kg) Knee add moment (Nm/kg) | NTL_ETL 0.48 (0.07)–0.44 (0.06) −4.3 (1.8)–−10.3 (3.5) 3.7 (3)–2.2 (3.4) −2.8 (10.7)–−7.3 (9.1) 0.60 (0.12)–0.51 (0.17) 0.29 (0.14)–0.16 (0.08) | 0.49 (0.06) −3.2 (2.2) 5.9 (2) −7 (5.1) 0.73 (0.14) 0.47 (0.16) | p > 0.05 p < 0.001 p > 0.05 p > 0.05 p > 0.05 p < 0.05 | |
| 6. [16] | Children with the unilateral diagnosis of Perthes confirmed on X-ray. |
C: 19 (14 boys and 5 girls)
P: 12 (10 boys and 2 girls) |
C: 7 (2.5)
P: 5.9 (2) | Temporospatial, kinematic, and kinetic | Thoracic, pelvic, hip, and knee |
Gait speed (m/s)
Step length (m) At midstance phase Thorax max obliquity ° Pelvis max obliquity ° Hip flex/ext ROM ° Knee flex/ext ROM ° Hip abd moment (Nm/kg) Knee abd moment (Nm/kg) | 0.45 (0.05) 0.81 (0.06) −6.1 (3.2) 3.7 (3.3) 33.2 (9.8) 11.8 (4.1) 0.59 (0.18) 0.26 (0.18) | 0.47 (0.06) 0.84 (0.06) −1.9 (2.2) 4.4 (2.9) 46.7 (6) 17.3 (6) 0.7 (0.13) 0.37 (0.15) | ||
| 7. [17] | A retrospective analysis of gait data including children with Perthes with other conditions. | C: 20 P: 45 | C 22 (2) P: 14 (2) | Temporospatial kinematic, and kinetic | Hip, knee, and ankle | Gait speed (m/s) Step length (m) Ankle plantarflexion° Hip work (Nm/kg) Knee work (Nm/kg) Ankle work (Nm/kg) | Affected_Non-affected 0.27 (0.06) 0.36 (0.06)–0.56 (0.1) 13.8 (7.3)–21.6 (11.9) 0.31 (0.3)–0.56 (0.22) 0.14 (0.11)–0.22 (0.16) 0.66 (0.18)–0.69 (0.25) | Control 0.33 (0.03) 0.41 (0.03) 23.5 (8.7) 0.68 (0.18) 0.27 (0.1) 0.88 (0.26) | p < 0.05 p < 0.05 p < 0.05 p < 0.05 p < 0.05 p > 0.05 | |
| 8. [3] | Children with unilateral Perthes disease classified by Mose classification based on latest follow-up X-ray. | C: 10 P: 10 | C: 8.5 (2.3) P: 9.1 (2.1) | Temporospatial, kinematic, and kinetic | Thoracic, pelvic, and hip | Gait speed (m/min) Stride length (m) Cadence (steps/min) Thorax flex/ext ROM° Thorax add/abd ROM° Thorax rotation ROM° Pelvis flex/ext ROM° Pelvis add/abd ROM° Pelvis rotation ROM° Hip flex/ext ROM° Hip add/abd ROM° Hip rotation ROM° VGR force (N/BW) | 57.4 (6.97) 1.06 (0.21) 107.6 (12.8) 11.12 (1.87) 14.04 (3.12) 16.85 (1.1) 10.26 (3.6) 8.25 (4.45) 18 (6.48) 40 (5.6) 13 (2.3) 14.7(12.2) 4.8 (1.7) | 63.79 (8.1) 1.23 (0.15) 103.5 (7.7) 9.43 (3.52) 12.6 (3.82) 22.55 (3.33) 7.83 (3.12) 10.25 (4.2) 21 (10.46) 46.4 (5.6) 16.9 (9.3) 23.6 (8.8) 7.6 (2.5) | p < 0.05 p = 0.05 p > 0.05 p < 0.05 p < 0.05 p < 0.05 p < 0.05 p < 0.05 p < 0.05 p < 0.05 p < 0.05 p < 0.05 p < 0.05 | |
| Study | Gait Compensation |
|---|---|
| 1. [4] | Temporospatial: Lower gait speed, shorter stride, and longer stance phase in the Perthes group. Kinematics: Two gait patterns; type 1 (trendelenburg) with pelvic drop, increased hip adduction, and trunk lean; type 2 (Duchenne) with trunk lean towards the affected limb. Kinetics: Type 1 showed increased hip abductor moment; type 2 showed reduced hip abductor moment. |
| 2. [15] | Out-toeing: Marked decrease in hip internal rotation on the affected Perthes side. In all out-toeing patients, affected hips were externally rotated almost throughout the gait cycle, whereas the pelvis rotated internally. At the midstance phase, the external rotation of the affected hip increased in comparison with the unaffected side, and there was an increase in internal pelvic rotation. In the sagittal plane, flexion of the affected hips decreased during gait in all out-toeing patients; hip flexion at the initial heel contact decreased compared with the unaffected side. In the coronal plane, no gait deviation was observed in terms of hip adduction and pelvic obliquity. In-toeing group: Marked decrease in hip external rotation. The affected hips showed persistently increased internal rotation and external pelvic rotation during gait. At the midstance phase, internal rotation of the affected hips increased, and external pelvic rotation was compared with the unaffected side. In the sagittal plane, hip extension was decreased during gait in three patients: maximal hip extension decreased compared with the unaffected side. In the coronal plane, all affected hips in in-toeing patients showed increased downward pelvic obliquity. |
| 3. [5] | Temporospatial: The normloading and overloading groups walked slower than the controls, while the unloading group walked faster. All Perthes groups had shorter stride lengths. Normloading and unloading groups showed less stride time, whereas the overloading group showed longer time. Both normloading and unloading groups had a higher cadence than the controls, with the overloading group having a lower cadence. Stance time was slightly longer in all Perthes groups. Kinematic: The overloading group demonstrated longer hip adduction during the stance phase, with normal pelvic motion except for a drop towards the swinging limb in the frontal plane. In the normloading group, the hip did not fully extend, with abnormal elevation of the pelvis on the swinging side. The unloading group showed slight hip abduction with external rotation during the stance phase, marked by more pronounced pelvic elevation. |
| 4. [7] | Kinematics: The Perthes groups showed deviations mainly at the pelvis and hip level, which were more pronounced in the florid stage (Group 1). Group 1 showed a significant increase in trunk total ROM with a significant posterior tilt position compared to normal. At the pelvis level, both Perthes groups showed a significant maximum pelvis anterior tilt compared to the controls. At the hip joint level, Group 1 demonstrated a significant reduction in maximum hip extension on both affected and non-affected sides. ROM was significantly reduced on the involved side at the knee joint level compared to the controls due to reduced maximum flexion in the swing. On the non-involved side, there was no significant deviation. At the level of the ankle, no significant difference was found. In Group 2, there were no significant differences at the level of the trunk, hip, knee, or ankle compared to the controls and compared to the non-involved side. Kinetics: Positive work: In Group 1, total work carried out (mainly in the hip joint) was significantly lower on the involved side than on the non-involved side compared to the controls. Negative work: Negative work carried out in Group 1 (mainly in the hip and knee) was also reduced compared to both the non-involved side and the controls. |
| 5. [6] | Temporospatial: Walking speed was slower in both NTL and ETL Perthes groups than the controls; however, there was no significant difference in walking speed between the Perthes groups and the control group. Kinematic: Thorax maximum obliquity was significantly higher in the ETL group than in the NTL and control groups. Pelvis maximum obliquity was lower in the ETL group than in the NTL and control groups. In foot rotation, less external foot rotation was seen in the NTL group than in the ETL and control groups. Kinetic: Hip adduction moment was lower in the ETL group than in the NTL and control groups. Knee adduction moment was significantly lower in the ETL group than in the NTL and control groups. |
| 6. [16] | Temporospatial: Insignificant differences in walking speed and step length in the Perthes group compared to the controls. Kinematics: Higher trunk obliquity, reduced pelvis obliquity, decreased hip extension, and increase in maximum knee extension in the Perthes group. Kinetics: Decreased hip and knee and adduction moments in the Perthes group. |
| 7. [17] | Temporospatial: Slower gait and shorter step length in the Perthes group. Step length was significantly shorter on the affected Perthes side and longer on the non-affected side than controls. Kinematic: Reduced ankle plantar flexion in the Perthes group. Kinetic: Reduced total positive work and lower hip and ankle work on the affected side. |
| 8. [3] | Temporospatial: Slower gait and shorter stride length in the Perthes group. Kinematics: Significant differences in trunk and pelvis ROM and reduced hip ROM in all planes. Kinetics: Lower hip extension and adduction moment. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mashabi, A.; Abdallat, R.; Alghamdi, M.S.; Al-Amri, M. Gait Compensation among Children with Non-Operative Legg–Calvé–Perthes Disease: A Systematic Review. Healthcare 2024, 12, 895. https://doi.org/10.3390/healthcare12090895
Mashabi A, Abdallat R, Alghamdi MS, Al-Amri M. Gait Compensation among Children with Non-Operative Legg–Calvé–Perthes Disease: A Systematic Review. Healthcare. 2024; 12(9):895. https://doi.org/10.3390/healthcare12090895
Chicago/Turabian StyleMashabi, Abdulrhman, Rula Abdallat, Mohammed S. Alghamdi, and Mohammad Al-Amri. 2024. "Gait Compensation among Children with Non-Operative Legg–Calvé–Perthes Disease: A Systematic Review" Healthcare 12, no. 9: 895. https://doi.org/10.3390/healthcare12090895