
Blood Transfusion Procedure: Assessment of Serbian Intensive Care Nurses’ Knowledge
 , , , , and
, , , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Settings
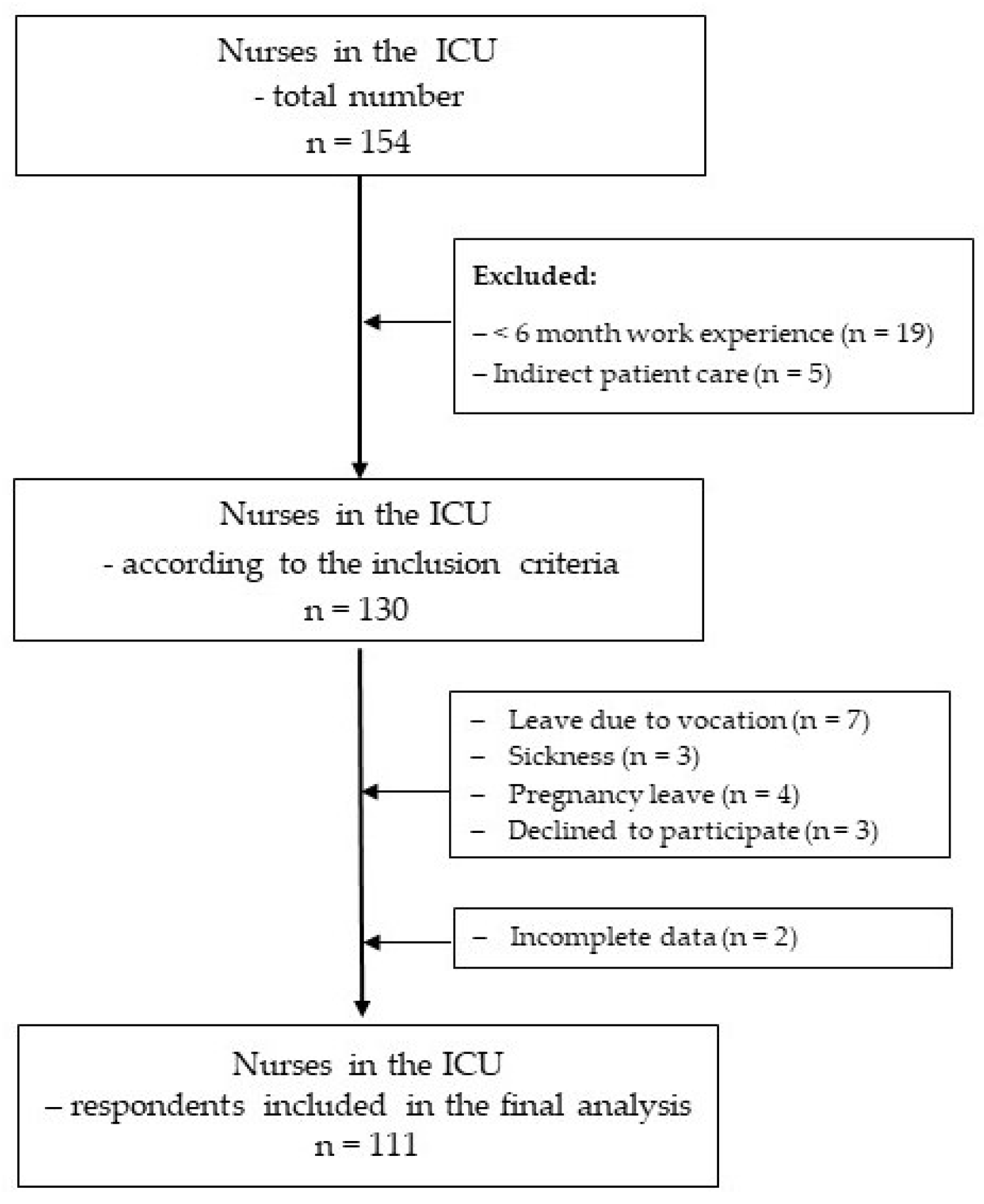
2.2. Sample
2.3. Instrument
2.4. Data Collection
2.5. Data Analysis
2.6. Ethical Consideration
3. Results
3.1. Sociodemographic Characteristics of the Study Sample
3.2. Analysis of Nurses’ Knowledge of the Blood Transfusion Procedure
3.3. Total Score on the Knowledge Test
3.4. Univariate Analysis of Mean Values on the Knowledge Test to the Sociodemographic Characteristics of Nurses
3.5. Standard Multiple Regression Analysis of the Effect of Sociodemographic Characteristics on the Knowledge Test Score
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Marshall, J.C.; Bosco, L.; Adhikari, N.K.; Connolly, B.; Diaz, J.V.; Dorman, T.; Fowler, R.A.; Meyfroidt, G.; Nakagawa, S.; Pelosi, P.; et al. What is an intensive care unit? A report of the task force of the World Federation of Societies of Intensive and Critical Care Medicine. J. Crit. Care 2017, 37, 270–276. [Google Scholar] [CrossRef]
- Neuenfeldt, F.S.; Weigand, M.A.; Fischer, D. Coagulopathies in Intensive Care Medicine: Balancing Act between Thrombosis and Bleeding. J. Clin. Med. 2021, 10, 5369. [Google Scholar] [CrossRef] [PubMed]
- Goel, R.; Patel, E.U.; Cushing, M.M.; Frank, S.M.; Ness, P.M.; Takemoto, C.M.; Vasovic, L.V.; Sheth, S.; Nellis, M.E.; Shaz, B.; et al. Association of Perioperative Red Blood Cell Transfusions With Venous Thromboembolism in a North American Registry. JAMA Surg. 2018, 153, 826–833. [Google Scholar] [CrossRef]
- Estcourt, L.J.; Malouf, R.; Trivella, M.; Fergusson, D.A.; Hopewell, S.; Murphy, M.F. Restrictive versus liberal red blood cell transfusion strategies for people with haematological malignancies treated with intensive chemotherapy or radiotherapy, or both, with or without haematopoietic stem cell support. Cochrane Database Syst. Rev. 2017, 1, CD011305. [Google Scholar] [CrossRef] [PubMed]
- Liumbruno, G.; Bennardello, F.; Lattanzio, A.; Piccoli, P.; Rossetti, G.; Italian Society of Transfusion Medicine and Immunohaematology (SIMTI) Work Group. Recommendations for the transfusion of plasma and platelets. Blood Transfus. 2009, 7, 132–150. [Google Scholar] [CrossRef] [PubMed]
- Nayeri, N.D.; Nadali, J.; Divani, A.; Hatefimoadab, N. Ways To Enhance Blood Transfusion Safety: A Systematic Review. Florence Nightingale J. Nurs. 2022, 30, 288–300. [Google Scholar] [CrossRef] [PubMed]
- Raasveld, S.J.; de Bruin, S.; Reuland, M.C.; Oord, C.v.D.; Schenk, J.; Aubron, C.; Bakker, J.; Cecconi, M.; Feldheiser, A.; Meier, J.; et al. Blood Cell Transfusion in the Intensive Care Unit. JAMA 2023, 330, 1852–1861. [Google Scholar] [CrossRef] [PubMed]
- Delaney, M.; Wendel, S.; Bercovitz, R.S.; Cid, J.; Cohn, C.; Dunbar, N.M.; O Apelseth, T.; Popovsky, M.; Stanworth, S.J.; Tinmouth, A.; et al. Transfusion reactions: Prevention, diagnosis, and treatment. Lancet 2016, 388, 2825–2836. [Google Scholar] [CrossRef]
- Sandler, S.G.; Vassallo, R.R. Anaphylactic transfusion reactions. Transfusion 2011, 51, 2265–2266. [Google Scholar] [CrossRef]
- Eder, A.F.; Dy, B.A.; Perez, J.M.; Rambaud, M.; Benjamin, R.J. The residual risk of transfusion-related acute lung injury at the American Red Cross (2008–2011): Limitations of a predominantly male-donor plasma mitigation strategy. Transfusion 2013, 53, 1442–1449. [Google Scholar] [CrossRef]
- Shander, A.; Javidroozi, M.; Lobel, G. Patient Blood Management in the Intensive Care Unit. Transfus. Med. Rev. 2017, 31, 264–271. [Google Scholar] [CrossRef] [PubMed]
- da Silva, K.F.N.; Duarte, R.D.; Floriano, D.R.; Andrade, L.F.; Tavares, J.L.; Félix, M.M.d.S.; Zuffi, F.B.; Pires, P.D.S.; Barbosa, M.H. Blood transfusion in Intensive Care Units: Knowledge of the nursing team. Av. En. Enfermería 2017, 35, 313–323. [Google Scholar] [CrossRef]
- Duarte, R.D.; da Silva, K.F.N.; dos Santos Félix, M.M.; Tavares, J.L.; Zuffi, F.B.; Barbosa, M.H. Knowledge about blood transfusion in a critical unit of a teaching hospital. Biosci. J. 2017, 33, 788–798. [Google Scholar] [CrossRef]
- Milutinović, D.; Lovrić, R.; Simin, D. Interprofessional education and collaborative practice: Psychometric analysis of the Readiness for Interprofessional Learning Scale in undergraduate Serbian healthcare student context. Nurse Educ. Today 2018, 65, 74–80. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Educational Modules on Clinical Use of Blood. 2021. Available online: https://iris.who.int/bitstream/handle/10665/350246/9789240033733-eng.pdf (accessed on 12 March 2022).
- Milosavljević, T. Postupak Primene Krvnih Komponenti i Transfuzijske Reakcije: Nacionalni Vodič: Republička Stručna Komisija za Transfuziologiju/The Procedure for Administration of Blood Components and Transfusion Reactions: A National Guide; Expert Commission for Transfusiology of the Republic of Serbia: Beograd, Serbia, 2005; pp. 2–59. [Google Scholar]
- Hijji, B.; Parahoo, K.; Hussein, M.M.; Barr, O. Knowledge of blood transfusion among nurses. J. Clin. Nurs. 2012, 22, 2536–2550. [Google Scholar] [CrossRef] [PubMed]
- Hijji, B.M.; Oweis, A.E.; Dabbour, R.S. Measuring knowledge of blood transfusion: A survey of Jordanian nurses. Am. Int. J. Contemp. Res. 2012, 2, 77–94. [Google Scholar]
- Encan, B.; Akin, S. Knowledge of Blood Transfusion Among Nurses. J. Contin. Educ. Nurs. 2019, 50, 176–182. [Google Scholar] [CrossRef]
- Jogi, I.E.; Mohanan, N.; Nedungalaparambil, N.M. Bedside blood transfusion—What nurses know and perform: A cross-sectional study from a tertiary-level cancer hospital in rural Kerala. Asia Pac. J. Oncol. Nurs. 2021, 8, 197–203. [Google Scholar] [CrossRef]
- Brown, M.; Brown, C. Improving nurses’ blood transfusion knowledge and skills. Br. J. Nurs. 2023, 32, 522–525. [Google Scholar] [CrossRef]
- Dubey, A.; Sonker, A.; Chaudhary, R. Evaluation of health care workers’ knowledge and functioning of blood centres in north India: A questionnaire based survey. Transfus. Apher. Sci. 2013, 4, 565–570. [Google Scholar] [CrossRef]
- Lee, S.L.E.; Rahim, A.N.A.; Azdiana, S.; Din, T.S.A. Knowledge of blood transfusion among nurses at hospital pulau pinang: Nursing responsibilities and patient management related to transfusion reactions. Educ. Med. J. 2016, 8, 47–56. [Google Scholar] [CrossRef]
- Noor, N.H.M.; Saad, N.H.; Khan, M.; Hassan, M.N.; Ramli, M.; Bahar, R.; Yusoff, S.M.; Iberahim, S.; Ab Rahman, W.S.W.; Zulkafli, Z.; et al. Blood Transfusion Knowledge among Nurses in Malaysia: A University Hospital Experience. Int. J. Environ. Res. Public. Health 2021, 18, 11194. [Google Scholar] [CrossRef]
- Gaur, R.; Mudgal, S.K.; Suyal, N.; Sharma, S.K.; Agarwal, R.; Raj, R.; Jitender, C. Nurses and nursing students’ knowledge regarding blood transfusion: A comparative cross-sectional study. J. Integr. Nurs. 2022, 4, 137–144. [Google Scholar] [CrossRef]
- Uzun, B.; Yılmaz, V.; Göklü, S.; Şahbaz, U.; Güvel, H. Blood transfusion knowledge levels of nurses in İzmir Atatürk training and research Hospital, turkey. Transfus. Clin. Biol. 2024, S1246-7820, 00002–00008. [Google Scholar] [CrossRef]
- Bolton-Maggs, P.H.B.; Wood, E.M.; Wiersum-Osselton, J.C. Wrong blood in tube—Potential for serious outcomes: Can it be prevented? Br. J. Haematol. 2015, 168, 3–13. [Google Scholar] [CrossRef]
- Vesga, M.A.; Azkárate, M. Information systems for a blood transfusion regional network. VOXS 2021, 16, 231–238. [Google Scholar] [CrossRef]
- Edwardson, S.; Cairns, C. Nosocomial infections in the ICU. Anaesth. Intensive Care Med. 2019, 20, 14–18. [Google Scholar] [CrossRef]
- Blot, S.; Ruppé, E.; Harbarth, S.; Asehnoune, K.; Poulakou, G.; Luyt, C.-E.; Rello, J.; Klompas, M.; Depuydt, P.; Eckmann, C.; et al. Healthcare-associated infections in adult intensive care unit patients: Changes in epidemiology, diagnosis, prevention and contributions of new technologies. Intensive Crit. Care Nurs. 2022, 70, 103227. [Google Scholar] [CrossRef]
- Freixo, A.; Matos, I.; Leite, A.; Silva, A.; Bischoff, F.; Carvalho, M.; Monteiro, C.; Ferreira, A.; Fernandes, S.; Lemos, N.; et al. Nurses knowledge in Transfusion Medicine in a Portuguese university hospital: The impact of an education. Blood Transfus. 2017, 15, 49–52. [Google Scholar] [CrossRef]
- Panchawagh, S.J.; Melinkeri, S.; Panchawagh, M.J. Assessment of Knowledge and Practice of Blood Transfusion Among Nurses in a Tertiary Care Hospital in India. Indian J. Hematol. Blood Transfus. 2020, 36, 393–398. [Google Scholar] [CrossRef]
- Louw, L.D.; Grobbelaar, J.; Henn, L.; van Zyl, L.; Wernich, C.; Wessels, P.-L.; Setlogelo, O.; Joubert, G.; Barrett, C. Management of blood products: Nursing knowledge and practices at an academic hospital. Transfus. Apher. Sci. 2021, 60, 102971. [Google Scholar] [CrossRef]
- Gorski, L.A.M.; Hadaway, L.M.; Hagle, M.E.P.; Broadhurst, D.M.; Clare, S.M.; Kleidon, T.M.; Meyer, B.M.P.; Nickel, B.A.-C.; Rowley, S.M.; Sharpe, E.D.; et al. Infusion therapy standards of practice, 8th Edition. J. Infus. Nurs. 2021, 44, S1–S224. [Google Scholar] [CrossRef]
- Mok, W.Q.; Wang, W.; Liaw, S.Y. Vital signs to detect deterioration. Int. J. Nurs. Pract. 2015, 21 (Suppl. S2), 91–98. [Google Scholar] [CrossRef]
- Kelly, C. Respiratory rate 1: Why measurement and recording are crucial. Nurs. Times 2018, 114, 23–24. [Google Scholar]
- Smith, A.; Gray, A.; Atherton, I.; Pirie, E.; Jepson, R. Does time matter? An investigation of knowledge and attitudes following blood transfusion training. Nurse Educ. Pract. 2014, 14, 176–182. [Google Scholar] [CrossRef]


{kind=link}
| N (%) | |||
|---|---|---|---|
| Variable | All Nurses | SMS | BA |
| Gender | |||
| Male | 18 (16.2) | 17 (19.8) | 1 (4.0) |
| Female | 93 (83.8) | 69 (80.2) | 24 (96.0) |
| Age (years) | |||
| 19–28 | 53 (47.7) | 50 (58.1) | 3 (12.0) |
| 29–38 | 36 (32.4) | 18 (20.9) | 18 (72.0) |
| 39–48 | 19 (17.1) | 15 (17.4) | 4 (16.0) |
| ≥49 | 3 (2.7) | 3 (3.5) | 0 (0.0) |
| Work experience | |||
| <1 | 38 (34.2) | 29 (33.7) | 9 (36.0) |
| 1–5 | 36 (32.4) | 31 (36.0) | 5 (20.0) |
| ≥5 | 37 (33.3) | 26 (30.2) | 11 (44.0) |
| Items Based on Knowledge of Correct Responses n (%) | |
|---|---|
| |
| 80 (72.1) |
| 26 (23.4) |
| 88 (79.3) |
| 65 (58.6) |
| 78 (70.3) |
| 53 (47.7) |
| 60 (54.1) |
| 90 (81.1) |
| 41 (36.9) |
| |
| 110 (99.1) |
| 79 (71.2) |
| 90 (81.1) |
| 80 (72.1) |
| 99 (89.2) |
| 59 (53.2) |
| 50 (45.0) |
| 67 (60.4) |
| |
| 51 (45.9) |
| 109 (98.2) |
| 64 (57.7) |
| 98 (88.3) |
| 54 (48.6) |
| 18 (16.2) |
| 38 (34.2) |
| 48 (43.2) |
| 82 (73.9) |
| 101 (91.0) |
| 51 (45.9) |
| 36 (32.4) |
| Knowledge TEST Score | Minimum | Maximum | Mean | SD |
|---|---|---|---|---|
| Total score (0–29) | 10.00 | 27.00 | 17.70 | 4.28 |
| Pretransfusion steps (0–9) | 2.00 | 9.00 | 5.23 | 1.58 |
| Initiating the transfusion (0–8) | 3.00 | 8.00 | 5.71 | 1.32 |
| Administration of transfusion and transfusion reactions (0–12) | 3.00 | 11.00 | 6.29 | 1.96 |
| Knowledge Level | |||
|---|---|---|---|
| Low (0–15) | Moderate (16–22) | High (23–29) | |
| n (%) | n (%) | n (%) | |
| Total | 26 (23.4) | 64 (57.7) | 21 (18.9) |
| Gender | |||
| Male | 1 (3.8) | 17 (26.6) | 0 (0.0) |
| Female | 25 (96.2) | 47 (73.4) | 64 (100) |
| Educational level | |||
| SMS | 26 (100.0) | 59 (92.2) | 1 (4.8) |
| BA | 0 (0.0) | 5 (7.8) | 20 (95.2) |
| Work experience (in years) | |||
| <1 | 16 (61.5) | 16 (25.0) | 6 (28.6) |
| 1–5 | 10 (38.5) | 22 (33.4) | 4 (19.0) |
| ≥5 | 0 (0.0) | 26 (46.0) | 11 (52.4) |
| Sociodemographic Characteristic | Total Score | Pretransfusion Steps | Initiating the Transfusion | Administration of Transfusion and Transfusion Reactions | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Gender | M ± SD | U | p | r | M ± SD | U | p | r | M ± SD | U | p | r | M ± SD | U | p | r |
| Male | 17.72 ± 1.93 | 835.00 | 0.987 | ns | 4.89 ± 1.13 | 707.00 | 0.288 | ns | 6.16 ± 1.04 | 654.00 | 0.132 | ns | 6.22 ± 1.11 | 797.00 | 0.746 | ns |
| Female | 17.69 ± 4.61 | 5.30 ± 1.65 | 5.62 ± 1.35 | 6.31 ± 2.10 | ||||||||||||
| Educational level | M ± SD | t (df) | p | d | M ± SD | t (df) | p | d | M ± SD | t (df) | p | d | M ± SD | t (df) | p | d |
| SMS | 16.03 ± 3.15 | 11.022 (109) | 0.000 | 0.53 * | 4.62 ± 1.07 | 11.053 (109) | 0.000 | 0.53 * | 5.43 ± 1.32 | 4.504 (109) | 0.000 | 0.16 * | 5.65 ± 1.57 | 8.086 (109) | 0.000 | 0.38 * |
| BA | 23.44 ± 2.14 | 7.36 ± 1.15 | 6.68 ± 0.75 | 8.51 ± 1.53 | ||||||||||||
| Work experience (in years) | M ± SD | F (df) | p | η2 | M ± SD | F (df) | p | η2 | M ± SD | F (df) | p | η2 | M ± SD | F (df) | p | η2 |
| <1 | 16.63 ± 5.17 | 9.201 (110) | 0.000 | 0.15 * | 5.11 ± 1.99 | 0.863 (110) | 0.425 | ns | 5.31 ± 1.56 | 14.467 (110) | 0.000 | 0.21 * | 5.82 ± 1.82 | 8.636 (110) | 0.000 | 0.14 * |
| 1–5 | 16.47 ± 3.65 | 5.08 ± 1.27 | 5.25 ± 0.94 | 5.75 ± 1.76 | ||||||||||||
| ≥5 | 20.00 ± 2.71 | 5.51 ± 1.37 | 6.56 ± 0.93 | 7.32 ± 1.93 | ||||||||||||
| Unstandardised Coefficient | Standardised Coefficient | t-Value | p-Value | Correlations Part | ||||
|---|---|---|---|---|---|---|---|---|
| ß | SE | Beta | F | p-Value | ||||
| Constant | 5.926 | 0.986 | 6.010 | 0.000 | 0.000 | |||
| Level Education | 7.237 | 0.617 | 0.710 | 11.731 | 0.000 | 0.708 | 83.152 | |
| Work experience | 1.461 | 0.314 | 0..282 | 4.661 | 0.000 | 0.281 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Simin, D.; Dolinaj, V.; Brestovački Svitlica, B.; Grujić, J.; Živković, D.; Milutinović, D. Blood Transfusion Procedure: Assessment of Serbian Intensive Care Nurses’ Knowledge. Healthcare 2024, 12, 720. https://doi.org/10.3390/healthcare12070720
Simin D, Dolinaj V, Brestovački Svitlica B, Grujić J, Živković D, Milutinović D. Blood Transfusion Procedure: Assessment of Serbian Intensive Care Nurses’ Knowledge. Healthcare. 2024; 12(7):720. https://doi.org/10.3390/healthcare12070720
Chicago/Turabian StyleSimin, Dragana, Vladimir Dolinaj, Branislava Brestovački Svitlica, Jasmina Grujić, Dragana Živković, and Dragana Milutinović. 2024. "Blood Transfusion Procedure: Assessment of Serbian Intensive Care Nurses’ Knowledge" Healthcare 12, no. 7: 720. https://doi.org/10.3390/healthcare12070720