
Are Higher Body Mass Index and Worse Metabolic Parameters Associated with More Aggressive Differentiated Thyroid Cancer? A Retrospective Cohort Study
 ,
,
Abstract
:1. Introduction
2. Material and Methods
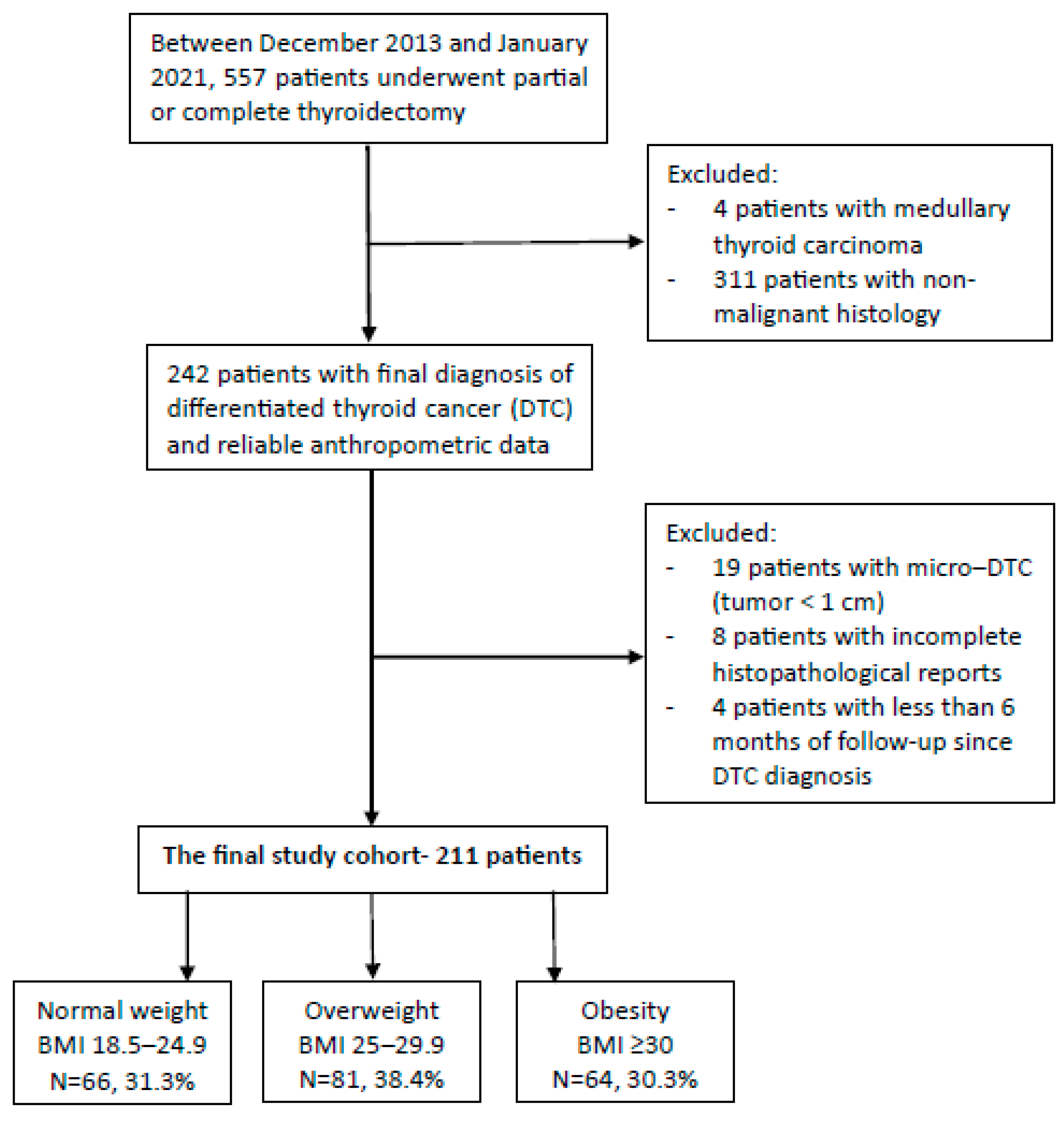
2.1. Study Population
2.2. Data Sources
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Histopathological Features
3.3. Treatment Modalities and Follow-Up
3.4. Logistic Regression Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 30 January 2024).
- Congdon, P.; Amugsi, D. Editorial: The Obesity Epidemic: Causes, Context, Prevention. Front. Public Health 2022, 10, 1030180. [Google Scholar] [CrossRef] [PubMed]
- GBD 2015 Obesity Collaborators; Afshin, A.; Forouzanfar, M.H.; Reitsma, M.B.; Sur, P.; Estep, K.; Lee, A.; Marczak, L.; Mokdad, A.H.; Moradi-Lakeh, M.; et al. Health Effects of Overweight and Obesity in 195 Countries over 25 Years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Qie, R.; Han, M.; Huang, S.; Wu, X.; Zhang, Y.; Feng, Y.; Yang, X.; Li, Y.; Wu, Y.; et al. Association of BMI with Cardiovascular Disease Incidence and Mortality in Patients with Type 2 Diabetes Mellitus: A Systematic Review and Dose-Response Meta-Analysis of Cohort Studies. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 1976–1984. [Google Scholar] [CrossRef] [PubMed]
- Quek, J.; Chan, K.E.; Wong, Z.Y.; Tan, C.; Tan, B.; Lim, W.H.; Tan, D.J.H.; Tang, A.S.P.; Tay, P.; Xiao, J.; et al. Global Prevalence of Non-Alcoholic Fatty Liver Disease and Non-Alcoholic Steatohepatitis in the Overweight and Obese Population: A Systematic Review and Meta-Analysis. Lancet Gastroenterol. Hepatol. 2023, 8, 20–30. [Google Scholar] [CrossRef]
- Sung, H.; Siegel, R.L.; Torre, L.A.; Pearson-Stuttard, J.; Islami, F.; Fedewa, S.A.; Goding Sauer, A.; Shuval, K.; Gapstur, S.M.; Jacobs, E.J.; et al. Global Patterns in Excess Body Weight and the Associated Cancer Burden. CA Cancer J. Clin. 2019, 69, 88–112. [Google Scholar] [CrossRef] [PubMed]
- Avgerinos, K.I.; Spyrou, N.; Mantzoros, C.S.; Dalamaga, M. Obesity and Cancer Risk: Emerging Biological Mechanisms and Perspectives. Metabolism 2019, 92, 121–135. [Google Scholar] [CrossRef]
- Nguyen, H.-L.; Geukens, T.; Maetens, M.; Aparicio, S.; Bassez, A.; Borg, A.; Brock, J.; Broeks, A.; Caldas, C.; Cardoso, F.; et al. Obesity-Associated Changes in Molecular Biology of Primary Breast Cancer. Nat. Commun. 2023, 14, 4418. [Google Scholar] [CrossRef]
- Seib, C.D.; Sosa, J.A. Evolving Understanding of the Epidemiology of Thyroid Cancer. Endocrinol. Metab. Clin. N. Am. 2019, 48, 23–35. [Google Scholar] [CrossRef]
- Pizzato, M.; Li, M.; Vignat, J.; Laversanne, M.; Singh, D.; La Vecchia, C.; Vaccarella, S. The Epidemiological Landscape of Thyroid Cancer Worldwide: GLOBOCAN Estimates for Incidence and Mortality Rates in 2020. Lancet Diabetes Endocrinol. 2022, 10, 264–272. [Google Scholar] [CrossRef]
- Chen, D.W.; Lang, B.H.H.; McLeod, D.S.A.; Newbold, K.; Haymart, M.R. Thyroid Cancer. Lancet 2023, 401, 1531–1544. [Google Scholar] [CrossRef]
- Mazumder, H.; Husain, M.; Hossain, M.F.; Mahmud, S. Prevalence, Trend and Associated Factors of Obesity-Related Cancers among U.S. Adults with Metabolic Syndrome: Evidence from the National Health and Nutrition Examination Survey 2001-2018. PLoS ONE 2023, 18, e0290994. [Google Scholar] [CrossRef]
- Wirth, L.J.; Sherman, E.; Robinson, B.; Solomon, B.; Kang, H.; Lorch, J.; Worden, F.; Brose, M.; Patel, J.; Leboulleux, S.; et al. Efficacy of Selpercatinib in RET-Altered Thyroid Cancers. N. Engl. J. Med. 2020, 383, 825–835. [Google Scholar] [CrossRef]
- Schmid, D.; Ricci, C.; Behrens, G.; Leitzmann, M.F. Adiposity and Risk of Thyroid Cancer: A Systematic Review and Meta-Analysis. Obes. Rev. 2015, 16, 1042–1054. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Feng, X.; Yang, W.; Li, X.; Zhang, K.; Feng, S.; Wang, F.; Yang, X. Appraising the Effect of Potential Risk Factors on Thyroid Cancer: A Mendelian Randomization Study. J. Clin. Endocrinol. Metab. 2022, 107, e2783–e2791. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, S.M.; Urbute, A.; Frederiksen, K.; Kjaer, S.K. Prepregnancy Body Mass Index and Risk of Differentiated Thyroid Cancer: A Prospective Cohort Study of More than 440,000 Danish Women. Thyroid 2023, 33, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Lauby-Secretan, B.; Scoccianti, C.; Loomis, D.; Grosse, Y.; Bianchini, F.; Straif, K. International Agency for Research on Cancer Handbook Working Group Body Fatness and Cancer—Viewpoint of the IARC Working Group. N. Engl. J. Med. 2016, 375, 794–798. [Google Scholar] [CrossRef] [PubMed]
- Kitahara, C.M.; McCullough, M.L.; Franceschi, S.; Rinaldi, S.; Wolk, A.; Neta, G.; Olov Adami, H.; Anderson, K.; Andreotti, G.; Beane Freeman, L.E.; et al. Anthropometric Factors and Thyroid Cancer Risk by Histological Subtype: Pooled Analysis of 22 Prospective Studies. Thyroid 2016, 26, 306–318. [Google Scholar] [CrossRef] [PubMed]
- Shin, A.; Cho, S.; Jang, D.; Abe, S.K.; Saito, E.; Rahman, M.S.; Islam, M.R.; Sawada, N.; Shu, X.-O.; Koh, W.-P.; et al. Body Mass Index and Thyroid Cancer Risk: A Pooled Analysis of Half a Million Men and Women in the Asia Cohort Consortium. Thyroid 2022, 32, 306–314. [Google Scholar] [CrossRef] [PubMed]
- Kitahara, C.M. Obesity, Physical Activity, and Thyroid Cancer Risk: Disentangling True Associations from Detection Bias. Thyroid 2023, 33, 276–277. [Google Scholar] [CrossRef]
- Park, J.; Kim, W.G.; Zhao, L.; Enomoto, K.; Willingham, M.; Cheng, S.-Y. Metformin Blocks Progression of Obesity-Activated Thyroid Cancer in a Mouse Model. Oncotarget 2016, 7, 34832–34844. [Google Scholar] [CrossRef]
- Park, J.W.; Han, C.R.; Zhao, L.; Willingham, M.C.; Cheng, S. Inhibition of STAT3 Activity Delays Obesity-Induced Thyroid Carcinogenesis in a Mouse Model. Endocr. Relat. Cancer 2016, 23, 53–63. [Google Scholar] [CrossRef]
- Park, S.; Willingham, M.C.; Qi, J.; Cheng, S.-Y. Metformin and JQ1 Synergistically Inhibit Obesity-Activated Thyroid Cancer. Endocr. Relat. Cancer 2018, 25, 865–877. [Google Scholar] [CrossRef]
- Matrone, A.; Ceccarini, G.; Beghini, M.; Ferrari, F.; Gambale, C.; D’Aqui, M.; Piaggi, P.; Torregrossa, L.; Molinaro, E.; Basolo, F.; et al. Potential Impact of BMI on the Aggressiveness of Presentation and Clinical Outcome of Differentiated Thyroid Cancer. J. Clin. Endocrinol. Metab. 2020, 105, dgz312. [Google Scholar] [CrossRef]
- Economides, A.; Giannakou, K.; Mamais, I.; Economides, P.A.; Papageorgis, P. Association Between Aggressive Clinicopathologic Features of Papillary Thyroid Carcinoma and Body Mass Index: A Systematic Review and Meta-Analysis. Front. Endocrinol. 2021, 12, 692879. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Tian, Y.; Jia, Z.; Yao, J.; Liao, L.; Dong, J. Abnormal Glucose Metabolism Parameters and the Aggressiveness of Differentiated Thyroid Carcinoma: A Hospital-Based Cross-Section Study in China. Front. Endocrinol. 2022, 13, 806349. [Google Scholar] [CrossRef] [PubMed]
- Yuge, H.; Okada, H.; Hamaguchi, M.; Kurogi, K.; Murata, H.; Ito, M.; Fukui, M. Triglycerides/HDL Cholesterol Ratio and Type 2 Diabetes Incidence: Panasonic Cohort Study 10. Cardiovasc. Diabetol. 2023, 22, 308. [Google Scholar] [CrossRef]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef]
- Hildrum, B.; Mykletun, A.; Hole, T.; Midthjell, K.; Dahl, A.A. Age-Specific Prevalence of the Metabolic Syndrome Defined by the International Diabetes Federation and the National Cholesterol Education Program: The Norwegian HUNT 2 Study. BMC Public Health 2007, 7, 220. [Google Scholar] [CrossRef]
- Jia, L.; Du, Y.; Chu, L.; Zhang, Z.; Li, F.; Lyu, D.; Li, Y.; Li, Y.; Zhu, M.; Jiao, H.; et al. Prevalence, Risk Factors, and Management of Dementia and Mild Cognitive Impairment in Adults Aged 60 Years or Older in China: A Cross-Sectional Study. Lancet Public Health 2020, 5, e661–e671. [Google Scholar] [CrossRef]
- Pizzimenti, C.; Fiorentino, V.; Ieni, A.; Martini, M.; Tuccari, G.; Lentini, M.; Fadda, G. Aggressive Variants of Follicular Cell-Derived Thyroid Carcinoma: An Overview. Endocrine 2022, 78, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Kluijfhout, W.P.; Pasternak, J.D.; Lim, J.; Kwon, J.S.; Vriens, M.R.; Clark, O.H.; Shen, W.T.; Gosnell, J.E.; Suh, I.; Duh, Q.-Y. Frequency of High-Risk Characteristics Requiring Total Thyroidectomy for 1–4 Cm Well-Differentiated Thyroid Cancer. Thyroid 2016, 26, 820–824. [Google Scholar] [CrossRef]
- Lee, J.S.; Lee, J.S.; Yun, H.J.; Kim, S.M.; Chang, H.; Lee, Y.S.; Chang, H.-S.; Park, C.S. Aggressive Subtypes of Papillary Thyroid Carcinoma Smaller Than 1 Cm. J. Clin. Endocrinol. Metab. 2023, 108, 1370–1375. [Google Scholar] [CrossRef]
- Feng, J.-W.; Yang, X.-H.; Wu, B.-Q.; Sun, D.-L.; Jiang, Y.; Qu, Z. Influence of Body Mass Index on the Clinicopathologic Features of Papillary Thyroid Carcinoma. Ann. Otol. Rhinol. Laryngol. 2019, 128, 625–632. [Google Scholar] [CrossRef] [PubMed]
- Friedenreich, C.M.; Ryder-Burbidge, C.; McNeil, J. Physical Activity, Obesity and Sedentary Behavior in Cancer Etiology: Epidemiologic Evidence and Biologic Mechanisms. Mol. Oncol. 2021, 15, 790–800. [Google Scholar] [CrossRef] [PubMed]
- Brenta, G.; Di Fermo, F. Thyroid Cancer and Insulin Resistance. Rev. Endocr. Metab. Disord. 2024, 25, 19–34. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Normal Weight | Overweight | Obesity | p Value * | ||
|---|---|---|---|---|---|
| BMI 18.5–24.9 | BMI 25–29.9 | BMI ≥ 30 | |||
| N = 66, 31.3% | N = 81, 38.4% | N = 64, 30.3% | |||
| Age at diagnosis, years (mean ± SD) | 41.53 ± 15.37 | 52.64 ± 16.26 | 51.14 ± 13.5 | * <0.001 | |
| a 0.001 | |||||
| b <0.001 | |||||
| c 1 | |||||
| Sex | Females (n, %) | 57, 86.36% | 61, 75.31% | 50, 78.13% | * 0.239 |
| a 0.094 | |||||
| Males (n, %) | 9, 13.64% | 20, 24.69% | 14, 21.88% | b 0.218 | |
| c 0.691 | |||||
| Ethnicity | Jewish (n, %) | 41, 62.12% | 58, 71.6% | 35, 54.69% | * 0.106 |
| a 0.223 | |||||
| Arab (n, %) | 25, 37.88% | 23, 28.4% | 29, 45.31% | b 0.39 | |
| c 0.035 | |||||
| Hypertension (n, %) | 4, 6.06% | 30, 37.04% | 19, 29.69% | * <0.001 | |
| a <0.001 | |||||
| b <0.001 | |||||
| c 0.433 | |||||
| Pre-diabetes or diabetes mellitus (n, %) | 6, 9.09% | 11, 13.58% | 17, 26.56% | * 0.014 | |
| a 0.385 | |||||
| b 0.007 | |||||
| c 0.041 | |||||
| Fasting glucose, mmol/L [mg/dL] (median, Q1–Q3) | 5.05, 4.77–5.47 [91, 86–98.5] | 5.27, 5–5.66 [95, 90–102] | 5.49, 5.05–6.22 [99, 91–112] | * 0.001 | |
| a 0.131 | |||||
| b <0.001 | |||||
| c 0.111 | |||||
| Glycated hemoglobin (HbA1c), mmol/mol [gr%] (median, Q1–Q3) | 37, 31–40 [5.5, 5–5.8] | 38, 33–41 [5.6, 5.2–5.9] | 40, 37–49 [5.8, 5.5–6.55] | * 0.012 | |
| a 0.925 | |||||
| b 0.015 | |||||
| c 0.098 | |||||
| Total cholesterol, mmol/L [mg/dL] (median, Q1–Q3) | 4.27, 3.73–5.08 [165, 144–196] | 4.64, 4.12–5.34 [179, 159–206] | 4.55, 4.04–5.27 [175.5, 156–203.5] | * 0.075 | |
| a 0.093 | |||||
| b 0.24 | |||||
| c 1 | |||||
| Triglycerides, mmol/L [mg/dL] (median, Q1–Q3) | 1.07, 0.81–1.71 [95, 72–151] | 1.33, 1.01–1.81 [118, 89–160] | 1.39, 1.06–2.43 [123, 93.5–215] | * 0.014 | |
| a 0.156 | |||||
| b 0.012 | |||||
| c 0.801 | |||||
| HDL-C, mmol/L [mg/dL] (mean ± SD) | 1.3 ± 0.3 [50.24 ± 11.68] | 1.27 ± 0.26 [49.06 ± 10.18] | 1.15 ± 0.28 [44.45 ± 10.67] | * 0.009 | |
| a 1 | |||||
| b 0.012 | |||||
| c 0.042 | |||||
| Triglycerides/HDL-C (median, Q1–Q3) | 2, 1.35–3.34 | 2.39, 1.72–3.63 | 2.79, 2.06–5.56 | * 0.006 | |
| a 0.395 | |||||
| b 0.004 | |||||
| c 0.18 | |||||
| TSH ¥, µIU/mL (median, Q1–Q3) | 0.45, 0.27–0.7 | 0.41, 0.28–0.78 | 0.42, 0.31–0.6 | * 0.977 | |
| Normal Weight | Overweight | Obesity | p Value * | |||
|---|---|---|---|---|---|---|
| BMI 18.5–24.9 | BMI 25–29.9 | BMI ≥ 30 | ||||
| N = 66, 31.3% | N = 81, 38.4% | N = 64, 30.3% | ||||
| T | pT (n, %) | pT 1–2 | 55, 83.33% | 63, 77.78% | 50, 78.13% | * 0.763 |
| a 0.484 | ||||||
| pT 3–4 | 11, 16.67% | 17, 20.99% | 13, 20.31% | b 0.563 | ||
| c 0.929 | ||||||
| Histological sub-type (n, %) | PTC | 60, 90.91% | 75, 92.59% | 60, 93.75% | * 1 | |
| a 1 | ||||||
| FTC | 5, 7.58% | 6, 7.41% | 4, 6.25% | b 1 | ||
| c 1 | ||||||
| PTC variant (n, %) | Classic | 32, 48.48% | 25, 30.86% | 20, 31.25% | * 0.62 | |
| a 0.6 | ||||||
| Follicular | 24, 36.36% | 41, 50.62% | 30, 46.88% | b 0.332 | ||
| Aggressive ¥ | 4, 6.06% | 9, 11.11% | 10, 15.63% | c 0.69 | ||
| Multifocality (n, %) | 26, 39.39% | 38, 46.91% | 24, 37.5% | * 0.486 | ||
| a 0.403 | ||||||
| b 0.771 | ||||||
| c 0.255 | ||||||
| Any extrathyroidal extension (n, %) | 14, 21.21% | 23, 28.4% | 20, 31.25% | * 0.399 | ||
| a 0.345 | ||||||
| b 0.232 | ||||||
| c 0.717 | ||||||
| LN | LN MTS (n, %) | No | 52, 78.79% | 59, 72.84% | 41, 64.06% | * 0.349 |
| a 0.372 | ||||||
| N1a | 6, 9.09% | 14, 17.28% | 13, 20.31% | b 0.129 | ||
| N1b | 7, 10.61% | 8, 9.88% | 9, 14.06% | c 0.576 | ||
| Bilateral lateral neck LN MRS (n, %) | 0, 0% | 2, 2.47% | 3, 4.69% | * 0.233 | ||
| a 0.502 | ||||||
| b 0.116 | ||||||
| c 0.655 | ||||||
| LN diameter ≥ 3 cm # (n, %) | 2, 3.03% | 0, 0% | 4, 6.25% | * 0.037 | ||
| a 0.2 | ||||||
| b 0.437 | ||||||
| c 0.036 | ||||||
| Extra-nodal extension # (n, %) | 4, 6.06% | 7, 8.64% | 8, 12.5% | * 0.436 | ||
| a 0.754 | ||||||
| b 0.204 | ||||||
| c 0.46 | ||||||
| Distal MTS (n, %) | 4, 6.06% | 2, 2.47% | 0, 0% | * 0.134 | ||
| a 0.407 | ||||||
| b 0.119 | ||||||
| c 0.504 | ||||||
| Normal Weight | Overweight | Obesity | p Value * | ||
|---|---|---|---|---|---|
| BMI 18.5–24.9 | BMI 25–29.9 | BMI ≥ 30 | |||
| N = 66, 31.3% | N = 81, 38.4% | N = 64, 30.3% | |||
| Thyroid surgery (n,%) | Partial | 23, 34.85% | 15, 18.52% | 17, 26.56% | * 0.08 |
| a 0.024 | |||||
| Complete | 43, 65.15% | 66, 81.48% | 47, 73.44% | b 0.306 | |
| c 0.246 | |||||
| RAI treatment (n,%) | No | 31, 46.97% | 30, 37.04% | 29, 45.31% | * 0.839 |
| a 0.532 | |||||
| 30 mCi | 10, 15.15% | 16, 19.75% | 11, 17.19% | b 0.948 | |
| ≥100 mCi | 21, 31.82% | 27, 33.33% | 20, 31.25% | c 0.697 | |
| Risk of disease recurrence ¥ (n,%) | Low | 37, 56.06% | 36, 44.44% | 29, 45.31% | * 0.363 |
| a 0.228 | |||||
| Intermediate or high | 25, 37.88% | 39, 48.15% | 30, 46.88% | b 0.276 | |
| c 1 | |||||
| Response to treatment § (n,%) | Excellent | 49, 74.24% | 57, 70.37% | 37, 57.81% | * 0.108 |
| a 0.79 | |||||
| Incomplete # | 7, 10.61% | 7, 8.64% | 12, 18.75% | b 0.111 | |
| c 0.056 | |||||
| Additional intervention @ (n,%) | 0, 0% | 5, 6.17% | 5, 7.81% | * 0.049 | |
| a 0.062 | |||||
| b 0.024 | |||||
| c 0.75 | |||||
| Histopathological Feature | Sub-Categories | Unadjusted | Adjusted @ |
|---|---|---|---|
| Odds Ratio (95% CI) * | Odds Ratio (95% CI) * | ||
| Histological sub-type and variants | PTC—classic variant | 1.00 (REF) | 1.00 (REF) |
| PTC—Follicular variant | 1.043 (0.982–1.107) | 1.024 (0.962–1.09) | |
| Aggressive variant ¥ of PTC and/or FTC | 1.089 (1.011–1.172) | 1.055 (0.973–1.143) | |
| Extrathyroidal extension | None | 1.00 (REF) | 1.00 (REF) |
| Microscopic | 1.016 (0.997–1.129) | 1.061 (0.993–1.133) | |
| Gross | 0.968 (0.869–1.079) | 0.915 (0.806–1.04) | |
| Vascular invasion | No | 1.00 (REF) | 1.00 (REF) |
| Yes | 0.984 (0.92–1.052) | 0.984 (0.917–1.056) | |
| Multifocality | No | 1.00 (REF) | 1.00 (REF) |
| Yes | 1.004 (0.954–1.057) | 0.997 (0.943–1.054) | |
| Any lymph node metstasis | None | 1.00 (REF) | 1.00 (REF) |
| Any | 1.061 (1.003–1.123) | 1.077 (1.013–1.145) | |
| Lateral neck LN MTS | No | 1.00 (REF) | 1.00 (REF) |
| Yes | 1.117 (0.978–1.275) | 1.129 (0.969–1.316) | |
| LN MTS ≥ 3 cm | No | 1.00 (REF) | 1.00 (REF) |
| Yes | 1.084 (0.952–1.233) | 1.101 (0.966–1.255) | |
| Extra-nodal extension | No | 1.00 (REF) | 1.00 (REF) |
| Gross | 1.040 (0.958–1.130) | 1.037 (0.948–1.135) | |
| Distal MTS | No | 1.00 (REF) | 1.00 (REF) |
| Yes | 0.863 (0.709–1.05) | 0.81 (0.645–1.017) |
| Histopathological Feature | Sub-Categories | Unadjusted | Adjusted @ |
|---|---|---|---|
| Odds Ratio (95% CI) * | Odds Ratio (95% CI) * | ||
| Histological sub-type and variants | PTC classic variant | 1.00 (REF) | 1.00 (REF) |
| PTC—follicular variant | 1.13 (0.942–1.355) | 1.125 (0.922–1.372) | |
| Aggressive variant ¥ of PTC and/or FTC | 1.302 (1.047–1.619) | 1.269 (1.001–1.61) | |
| Extrathyroidal extension | None | 1.00 (REF) | 1.00 (REF) |
| Microscopic | 1.007 (0.839–1.208) | 0.999 (0.819–1.219) | |
| Gross | 0.839 (0.581–1.211) | 0.716 (0.465–1.104) | |
| Vascular invasion | No | 1.00 (REF) | 1.00 (REF) |
| Yes | 0.995 (0.805–1.229) | 0.999 (0.796–1.255) | |
| Multifocality | No | 1.00 (REF) | 1.00 (REF) |
| Yes | 1.137 (0.975–1.326) | 1.072 (0.908–1.266) | |
| Lateral neck LN MTS | No | 1.00 (REF) | 1.00 (REF) |
| Yes | 1.029 (0.658–1.61) | 0.931 (0.572–1.517) | |
| LN MTS ≥ 3 cm | No | 1.00 (REF) | 1.00 (REF) |
| Yes | 1.25 (0.893–1.749) | 1.163 (0.796–1.699) | |
| Extra-nodal extension | No | 1.00 (REF) | 1.00 (REF) |
| Yes | 1.101 (0.845–1.435) | 1.022 (0.759–1.376) | |
| Distal MTS | No | 1.00 (REF) | 1.00 (REF) |
| Yes | 1.146 (0.652–2.016) | 1.134 (0.481–2.675) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abu Arar, Y.; Shilo, M.; Bilenko, N.; Friger, M.; Marsha, H.; Fisher, D.; Fraenkel, M.; Yoel, U. Are Higher Body Mass Index and Worse Metabolic Parameters Associated with More Aggressive Differentiated Thyroid Cancer? A Retrospective Cohort Study. Healthcare 2024, 12, 581. https://doi.org/10.3390/healthcare12050581
Abu Arar Y, Shilo M, Bilenko N, Friger M, Marsha H, Fisher D, Fraenkel M, Yoel U. Are Higher Body Mass Index and Worse Metabolic Parameters Associated with More Aggressive Differentiated Thyroid Cancer? A Retrospective Cohort Study. Healthcare. 2024; 12(5):581. https://doi.org/10.3390/healthcare12050581
Chicago/Turabian StyleAbu Arar, Yasmin, Michael Shilo, Natalya Bilenko, Michael Friger, Hagit Marsha, David Fisher, Merav Fraenkel, and Uri Yoel. 2024. "Are Higher Body Mass Index and Worse Metabolic Parameters Associated with More Aggressive Differentiated Thyroid Cancer? A Retrospective Cohort Study" Healthcare 12, no. 5: 581. https://doi.org/10.3390/healthcare12050581