
Life beyond Loss: A Retrospective Analysis of the Impact of Meaning of Life Therapy on the Grieving Process of Cancer Patients’ Family Caregivers
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Objectives
2.2. Method
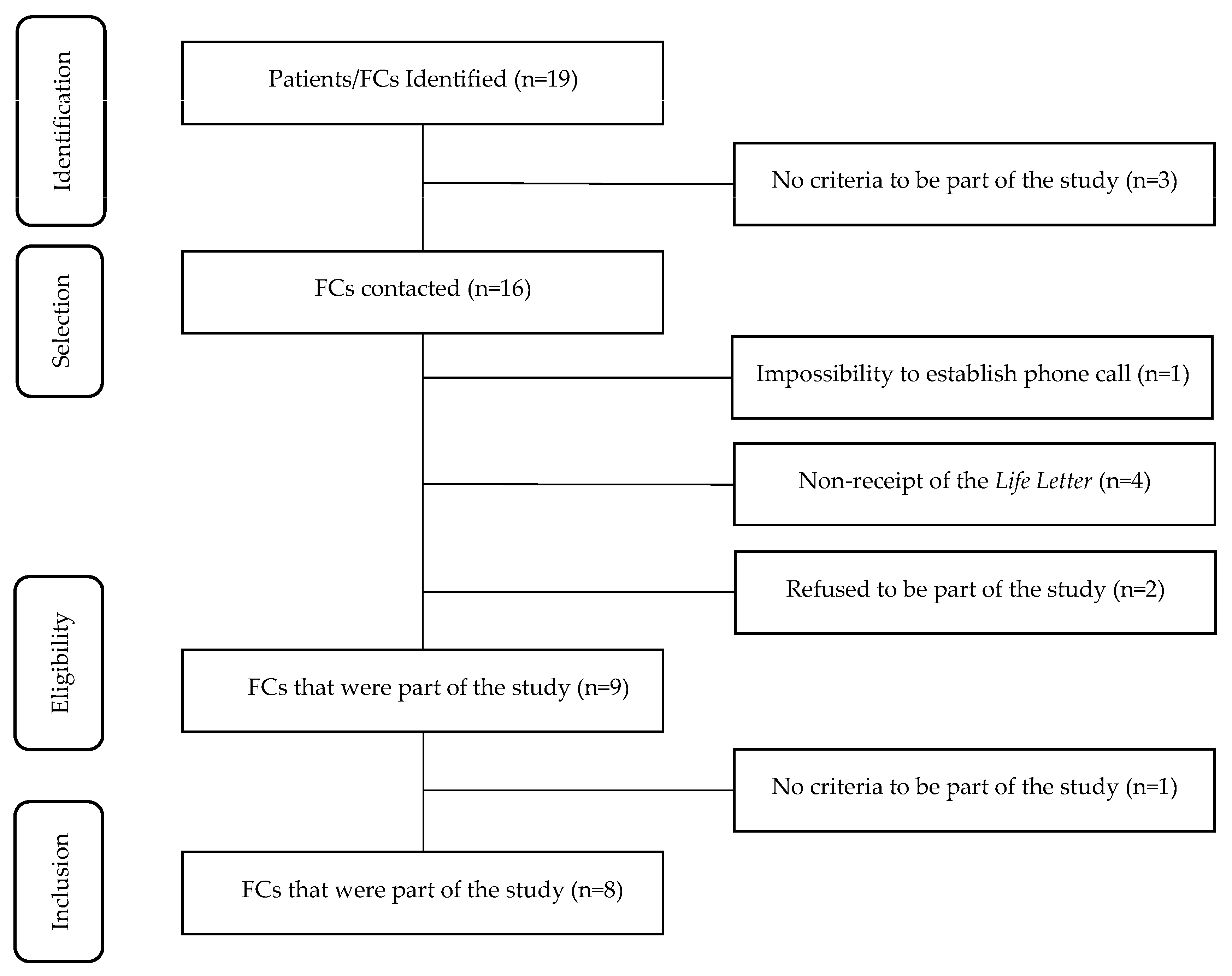
2.3. Participants
2.4. Procedure
2.5. Data Analysis
3. Results
3.1. Remembrance of the Intervention
3.2. FCs’ Perceptions about Patients’ Adaptation to the End-of-Life Stage
3.3. FCs’ Adaptation to Patients’ End of Life
3.4. The Role of the LL in the End-of-Life Adaptation Process
3.5. Grieving Process
4. Discussion
4.1. Implications for Clinical Practice
4.2. Limitations and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Scarton, L.J.; Boyken, L.; Lucero, R.J.; Fitchett, G.; Handzo, G.; Emanuel, L.; Wilkie, D.J. Effects of Dignity Therapy on family members: A systematic review. J. Hosp. Palliat. Nurs. 2018, 20, 542–547. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Chen, J.; Wang, Y.; Xu, W.; Xie, M.; Wu, Y.; Hu, R. Effects of family participatory dignity therapy on the psychological well-being and family function of patients with haematologic malignancies and their family caregivers: A randomised controlled trial. Int. J. Nurs. Stud. 2021, 118, 103922. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, A.J.; Ferguson, D.W.; Gill, J.; Paul, J.; Symonds, P. Depression and anxiety in long-term cancer survivors compared with spouses and healthy controls: A systematic review and meta-analysis. Lancet Oncol. 2013, 14, 721–732. [Google Scholar] [CrossRef]
- Ando, M.; Morita, T.; Okamoto, T.; Ninosaka, Y. One-week short-term Life Review interview can improve spiritual well-being of terminally ill cancer patients. Psychooncology 2008, 17, 885–890. [Google Scholar] [CrossRef] [PubMed]
- Costa, D.S.J.; Mercieca-Bebber, R.; Rutherford, C.; Gabb, L.; King, M.T. The impact of cancer on psychological and social outcomes. Aust. Psychol. 2016, 51, 89–99. [Google Scholar] [CrossRef]
- Bruce, A.; Schreiber, R.; Petrovskaya, O.; Boston, P. Longing for ground in a ground(less) world: A qualitative inquiry of existential suffering. BMC Nurs. 2011, 10, 1–9. [Google Scholar] [CrossRef]
- Sansom-Daly, U.M.; Lobb, E.A.; Evans, H.E.; Breen, L.J.; Ugalde, A.; Best, M.; Zomerdijk, N.; Beasley, E.A.; Taylor, K.L.; Clayton, J.; et al. To be mortal is human: Professional consensus around the need for more psychology in palliative care. BMJ Support. Palliat. Care 2021, 11, 401–403. [Google Scholar] [CrossRef]
- Nagelschmidt, K.; Leppin, N.; Seifart, C.; Rief, W.; von Blanckenburg, P. Systematic mixed-method review of barriers to end-of-life communication in the family context. BMJ Support. Palliat. Care 2021, 11, 253–263. [Google Scholar] [CrossRef]
- Cejudo López, Á.; López López, B.; Duarte Rodríguez, M.; Crespo Serván, M.P.; Coronado Illescas, C.; Fuente Rodríguez, C. El pacto de silencio desde la perspectiva de las personas cuidadoras de pacientes paliativos. Enferm. Clín. 2015, 25, 124–132. [Google Scholar] [CrossRef]
- Bermejo, J.C.; Villacieros, M.; Carabias, R.; Sánchez, E.; Díaz-Albo, B. Conspiración del silencio en familiares y pacientes al final de la vida ingresados en una unidad de cuidados paliativos: Nivel de información y actitudes observadas. Med. Paliat. 2013, 20, 49–59. [Google Scholar] [CrossRef]
- Espinoza-Suárez, N.R.; Zapata del Mar, C.M.; Mejía Pérez, L.A. Conspiración de silencio: Una barrera en la comunicación médico, paciente y familia. Rev. Neuro-Psiquiatr. 2017, 80, 125–136. [Google Scholar] [CrossRef]
- von Blanckenburg, P.; Knorrenschild, J.R.; Hofmann, M.; Fries, H.; Nestoriuc, Y.; Seifart, U.; Rief, W.; Seifart, C. Expectations, end-of-life fears and end-of-life communication among palliative patients with cancer and caregivers: A cross-sectional study. BMJ Open 2022, 12, e058531. [Google Scholar] [CrossRef]
- Grijó, L.; Tojal, C.; Rego, F. Effects of dignity therapy on palliative patients’ family members: A systematic review. Palliat. Support. Care 2021, 19, 605–614. [Google Scholar] [CrossRef] [PubMed]
- Daneault, S.; Lussier, V.; Mongeau, S.; Paillé, P.; Hudon, E.; Dion, D.; Yelle, L. The nature of suffering and its relief in the terminally ill: A qualitative study. J. Palliat. Care 2004, 20, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Bovero, A.; Sedghi, N.A.; Opezzo, M.; Botto, R.; Pinto, M.; Ieraci, V.; Torta, R. Dignity-related existential distress in end-of-life cancer patients: Prevalence, underlying factors, and associated coping strategies. Psychooncology 2018, 27, 2631–2637. [Google Scholar] [CrossRef] [PubMed]
- Chochinov, H.M.; Hassard, T.; McClement, S.; Hack, T.; Kristjanson, L.J.; Harlos, M.; Sinclair, S.; Murray, A. The landscape of distress in the terminally ill. J. Pain Symptom Manag. 2009, 38, 641–649. [Google Scholar] [CrossRef] [PubMed]
- Fitchett, G.; Emanuel, L.; Handzo, G.; Boyken, L.; Wilkie, D.J. Care of the human spirit and the role of dignity therapy: A systematic review of dignity therapy research. BMC Palliat. Care 2015, 14, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Moghaddam, N.; Coxon, H.; Nabarro, S.; Hardy, B.; Cox, K. Unmet care needs in people living with advanced cancer: A systematic review. Support. Care Cancer 2016, 24, 3609–3622. [Google Scholar] [CrossRef] [PubMed]
- Hack, T.F.; McClement, S.E.; Chochinov, H.M.; Cann, B.J.; Hassard, T.H.; Kristjanson, L.J.; Harlos, M. Learning from dying patients during their final days: Life reflections gleaned from dignity therapy. Palliat. Med. 2010, 24, 715–723. [Google Scholar] [CrossRef]
- Onishi, H. Communication at the end of life. J. Hosp. Palliat. Care 2021, 24, 135–143. [Google Scholar] [CrossRef]
- Daneault, S.; Lussier, V.; Mongeau, S.; Yelle, L.; Côté, A.; Sicotte, C.; Paillé, P.; Dion, D.; Coulombe, M. Ultimate journey of the terminal ill: Ways and pathways of hope. Can. Fam. Physician 2016, 62, 648–656. [Google Scholar]
- Vuksanovic, D.; Green, H.; Morrissey, S.; Smith, S. Dignity Therapy and Life Review for palliative care patients: A qualitative study. J. Pain Symptom Manag. 2017, 54, 530–537. [Google Scholar] [CrossRef]
- Iani, L.; De Vincenzo, F.; Maruelli, A.; Chochinov, H.M.; Ragghianti, M.; Durante, S.; Lombardo, L. Dignity Therapy helps terminally ill patients maintain a sense of peace: Early results of a randomized controlled trial. Front. Psychol. 2020, 11, 1468. [Google Scholar] [CrossRef] [PubMed]
- Große, J.; Treml, J.; Kersting, A. Impact of caregiver burden on mental health in bereaved caregivers of cancer patients: A systematic review. Psychooncology 2018, 27, 757–767. [Google Scholar] [CrossRef] [PubMed]
- Stenberg, U.; Ruland, C.M.; Miaskowski, C. Review of the literature on the effects of caring for a patient with cancer. Psychooncology 2010, 19, 1013–1025. [Google Scholar] [CrossRef] [PubMed]
- Coelho, A.; de Brito, M.; Teixeira, P.; Frade, P.; Barros, L.; Barbosa, A. Family caregivers’ anticipatory grief: A conceptual framework for understanding its multiple challenges. Qual. Health Res. 2020, 30, 693–703. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Tang, N.; Yang, L.; Zeng, Q.; Yu, T.; Pu, X.; Wang, J.; Zhang, H. Effect of caregiver burden on anticipatory grief among caregivers of elderly cancer patients: Chain mediation role of family functioning and resilience. Front. Psychol. 2023, 13, 1020517. [Google Scholar] [CrossRef] [PubMed]
- Dumont, I.; Dumont, S.; Mongeau, S. End-of-life care and the grieving process: Family caregivers who have experienced the loss of a terminal-phase cancer patient. Qual. Health Res. 2008, 18, 1049–1061. [Google Scholar] [CrossRef] [PubMed]
- Colosimo, K.; Nissim, R.; Pos, A.E.; Hales, S.; Zimmermann, C.; Rodin, G. “Double awareness” in psychotherapy for patients living with advanced cancer. J. Psychother. Integr. 2018, 28, 125–140. [Google Scholar] [CrossRef]
- Mako, C.; Galek, K.; Poppito, S.R. Spiritual pain among patients with advanced cancer in palliative care. J. Palliat. Med. 2006, 9, 1106–1113. [Google Scholar] [CrossRef]
- Julião, M.; Oliveira, F.; Nunes, B.; Carneiro, A.V.; Barbosa, A. Effect of Dignity Therapy on end-of-life psychological distress in terminally ill Portuguese patients: A randomized controlled trial. Palliat. Support. Care 2017, 15, 628–637. [Google Scholar] [CrossRef]
- von Blanckenburg, P.; Leppin, N. Psychological interventions in palliative care. Curr. Opin. Psychiatry 2018, 31, 389–395. [Google Scholar] [CrossRef]
- Ando, M.; Morita, T.; Akechi, T.; Okamoto, T. Efficacy of short-term Life-Review interviews on the spiritual well-being of terminally ill cancer patients. J. Pain Symptom Manag. 2010, 39, 993–1002. [Google Scholar] [CrossRef]
- Kleijn, G.; Lissenberg-Witte, B.I.; Bohlmeijer, E.T.; Willemsen, V.; Becker-Commissaris, A.; Eeltink, C.M.; Bruynzeel, A.M.E.; van der Vost, M.J.; Cuijpers, P.; Verdonck-de Leeuw, I.M. A randomized controlled trial on the efficacy of Life Review therapy targeting incurably ill cancer patients: Do their informal caregivers benefit? Support. Care Cancer 2021, 29, 1257–1264. [Google Scholar] [CrossRef]
- Zhang, X.; Xiao, H.; Chen, Y. Effects of Life Review on mental health and well-being among cancer patients: A systematic review. Int. J. Nurs. Stud. 2017, 74, 138–148. [Google Scholar] [CrossRef] [PubMed]
- Chochinov, H.M.; Hack, T.; Hassard, T.; Kristjanson, L.J.; McClement, S.; Harlos, M. Dignity and psychotherapeutic considerations in end-of-life care. J. Palliat. Care 2004, 20, 134–142. [Google Scholar] [CrossRef] [PubMed]
- Chochinov, H.M.; Hack, T.; Hassard, T.; Kristjanson, L.J.; McClement, S.; Harlos, M. Dignity Therapy: A novel psychotherapeutic intervention for patients near the end of life. J. Clin. Oncol. 2005, 23, 5520–5525. [Google Scholar] [CrossRef] [PubMed]
- Chochinov, H.M.; Kristjanson, L.J.; Breitbart, W.; McClement, S.; Hack, T.F.; Hassard, T.; Harlos, M. Effect of Dignity Therapy on distress and end-of-life experience in terminally ill patients: A randomised controlled trial. Lancet Oncol. 2011, 12, 753–762. [Google Scholar] [CrossRef] [PubMed]
- Chochinov, H.M.; Cann, B.; Cullihall, K.; Kristjanson, L.; Harlos, M.; McClement, S.E.; Hack, T.F.; Hassard, T. Dignity Therapy: A feasibility study of elders in long-term care. Palliat. Support. Care 2012, 10, 3–15. [Google Scholar] [CrossRef] [PubMed]
- Breitbart, W.; Rosenfeld, B.; Gibson, C.; Pessin, H.; Poppito, S.; Nelson, C.; Tomarken, A.; Timm, A.K.; Berg, A.; Jacobson, C.; et al. Meaning-centered group psychotherapy for patients with advanced cancer: A pilot randomized controlled trial. Psychooncology 2010, 19, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Julião, M.; Sobral, M.A.; Johnston, B.; Lemos, A.R.; Almeida, S.; Antunes, B.; Dönmez, Ç.F.; Chochinov, H.M. A Portuguese trial using Dignity Therapy for adults who have a life-threatening disease: Qualitative analysis of generativity documents. Palliat. Support. Care 2021, 20, 189–195. [Google Scholar] [CrossRef]
- Kasl-Godley, J.E.; King, D.A.; Quill, T.E. Opportunities for psychologists in palliative care: Working with patients and families across the disease continuum. Am. Psychol. 2014, 69, 364–376. [Google Scholar] [CrossRef]
- Warth, M.; Kessler, J.; Koehler, F.; Aguilar-Raab, C.; Bardenheuer, H.J.; Ditzen, B. Brief psychosocial interventions improve quality of life of patients receiving palliative care: A systematic review and meta-analysis. Palliat. Med. 2019, 33, 332–345. [Google Scholar] [CrossRef]
- Cardoso, A.R.; Remondes-Costa, S.; Veiga, E.; Almeida, V.; Rocha, J.; Teixeira, R.J.; Macedo, G.; Leite, M. Meaning of Life Therapy: A pilot study of a novel psycho-existential intervention for Palliative Care in cancer. Omega 2023, 26, 302228231209654. [Google Scholar] [CrossRef]
- Chochinov, H.M. Dying, dignity, and new horizons in palliative end-of-life care. CA Cancer J. Clin. 2006, 56, 84–103. [Google Scholar] [CrossRef] [PubMed]
- Logan, E.L.; Thornton, J.A.; Kane, R.T.; Breen, L.J. Social support following bereavement: The role of beliefs, expectations, and support intentions. Death Stud. 2018, 42, 471–482. [Google Scholar] [CrossRef] [PubMed]
- Shear, M.K. Clinical practice. Complicated Grief. N. Engl. J. Med. 2015, 372, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Stroebe, M.; Schut, H.; Stroebe, W. Health outcomes of bereavement. Lancet 2007, 370, 1960–1973. [Google Scholar] [CrossRef] [PubMed]
- Miles, M.B.; Huberman, A.M.; Saldaña, J. Qualitative Data Analysis A Methods Sourcebook, 3rd ed.; Sage Publications: New York, NY, USA, 2014; pp. 299–300. [Google Scholar]
- Castleberry, A.; Nolen, A. Thematic analysis of qualitative research data: Is it as easy as it sounds? Curr. Pharm. Teach. Learn. 2018, 10, 807–815. [Google Scholar] [CrossRef] [PubMed]
- Creswell, J.W.; Poth, C.N. Qualitative Inquiry & Research Design Choosing Among Five Approaches, 4th ed.; Sage Publications: New York, NY, USA, 2018; pp. 156–160. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Yin, R.K. Qualitative Research from Start to Finish, 2nd ed.; The Guilford Press: New York, NY, USA, 2016; pp. 185–187. [Google Scholar]
- Elo, S.; Kyngäs, H. The qualitative content analysis process. J. Adv. Nurs. 2008, 62, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Guest., G.; MacQueen, K.M.; Namey, E.E. Applied Thematic Analysis; Sage Publications: New York, NY, USA, 2012; p. 10. [Google Scholar]
- Levitt, H.M.; Motulsky, S.L.; Wertz, F.J.; Morrow, S.L.; Ponterotto, J.G. Recommendations for designing and reviewing qualitative research in psychology: Promoting methodological integrity. Qual. Psychol. 2017, 4, 2–22. [Google Scholar] [CrossRef]
- Graneheim, U.H.; Lundman, B. Qualitative content analysis in nursing research: Concepts, procedures and measures to achieve trustworthiness. Nurse Educ. Today 2004, 24, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Yun, Y.H.; Kwon, Y.C.; Lee, M.K.; Lee, W.J.; Jung, K.H.; Do, Y.R.; Kim, S.; Heo, D.S.; Choi, J.S.; Park, S.Y. Experiences and attitudes of patients with terminal cancer and their family caregivers toward the disclosure of terminal illness. J. Clin. Oncol. 2010, 28, 1950–1957. [Google Scholar] [CrossRef] [PubMed]
- Johnston, G.; Abraham, C. Managing awareness: Negotiating and coping with a terminal prognosis. Int. J. Palliat. Nurs. 2000, 6, 485–494. [Google Scholar] [CrossRef] [PubMed]
- Boston, P.; Bruce, A.; Schreiber, R. Existential suffering in the palliative care setting: An integrated literature review. J. Pain Symptom Manag. 2011, 41, 604–618. [Google Scholar] [CrossRef] [PubMed]
- Rainbird, K.; Perkins, J.; Sanson-Fisher, R.; Rolfe, I.; Anseline, P. The needs of patients with advanced, incurable cancer. Br. J. Cancer 2009, 101, 759–764. [Google Scholar] [CrossRef] [PubMed]
- Lemus-Riscanevo, P.; Carreño-Moreno, S.; Arias-Rojas, M. Conspiracy of silence in palliative care: A concept analysis. Indian J. Palliat. Care 2019, 25, 24–29. [Google Scholar]
- Fallowfield, L.J.; Jenkins, V.A.; Beveridge, H.A. Truth may hurt but deceit hurts more: Communication in palliative care. Palliat. Med. 2002, 16, 297–303. [Google Scholar] [CrossRef]
- Neto, I.G. Capítulo 1: Princípios dos cuidados paliativos. In Humanização em Cuidados Paliativos, 1st ed.; Abejas, A.G., Duarte, C., Eds.; Lidel: Lisboa, Portugal, 2021; pp. 3–10. [Google Scholar]
- Cardoso, A.R. “Cartas para a vida: Legado depois da partida” – Estudo misto sobre a experiência subjetiva do doente em fim de vida. Master’s Thesis, Universidade de Trás-os-Montes e Alto Douro–UTAD, Vila Real, Portugal, 2019. [Google Scholar]
- Rocha, N.C. Intervenção em Cuidados Paliativos em Tempos de COVID-19: Estudo Piloto da Terapia do Sentido de Vida por Videoconferência. Master’s Thesis, Instituto Universitário de Ciências da Saúde–IUCS, CESPU, Paredes–Gandra, Gandra, Portugal, 2021. [Google Scholar]
- Field, N.P.; Gao, B.; Paderna, L. Continuing bonds in bereavement: An attachment theory based perspective. Death Stud. 2005, 29, 277–299. [Google Scholar] [CrossRef]
- Williams, A.; McCorkle, R. Cancer family caregivers during the palliative, hospice, and bereavement phases: A review of the descriptive psychosocial literature. Palliat. Support. Care 2011, 9, 315–325. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.; Cottingham, A.H.; Stutz, P.V.; Gruber, R.; Bernat, J.K.; Helft, P.R.; Wilhelm, L.; Schmidt, K.; Stout, M.E.; Willard, C.; et al. Abbreviated Dignity Therapy for adults with advanced-stage cancer and their family caregivers: Qualitative analysis of a pilot study. Palliat. Support. Care 2019, 17, 262–268. [Google Scholar] [CrossRef]
- Goddard, C.; Speck, P.; Martin, P.; Hall, S. Dignity Therapy for older people in care homes: A qualitative study of the views of residents and recipients of ‘generativity’ documents. J. Adv. Nurs. 2013, 69, 122–132. [Google Scholar] [CrossRef]
- Dose, A.M.; Rhudy, L.M. Perspectives of newly diagnosed advanced cancer patients receiving Dignity Therapy during cancer treatment. Support. Care Cancer 2018, 26, 187–195. [Google Scholar] [CrossRef] [PubMed]
- Stroebe, M.; Schut, H.; Boerner, K. Continuing bonds in adaptation to bereavement: Toward theoretical integration. Clin. Psychol. Rev. 2010, 30, 259–268. [Google Scholar] [CrossRef]
- Maciejewski, P.K.; Zhang, B.; Block, S.D.; Prigerson, H.G. An empirical examination of the stage theory of grief. JAMA 2007, 297, 716–723. [Google Scholar] [CrossRef] [PubMed]
- Parkes, C.M.; Prigerson, H.G. Bereavement Studies of Grief in Adult Life, 4th ed.; Routledge: New York, NY, USA, 2010; pp. 113–114, 260. [Google Scholar]
- Stroebe, M.; Schut, H. The Dual Process Model of Coping with bereavement: Rationale and description. Death Stud. 1999, 23, 197–224. [Google Scholar]
- Stroebe, W.; Abakoumkin, G.; Stroebe, M. Beyond depression: Yearning for the loss of a loved one. Omega 2010, 61, 85–101. [Google Scholar] [CrossRef]
- Stroebe, M.; Schut, H. The Dual Process Model of Coping with bereavement: A decade on. Omega 2010, 61, 273–289. [Google Scholar] [CrossRef]
- Pimenta, S.; Capelas, M.L.V. A abordagem do luto em cuidados paliativos. Cadernos de Saúde 2019, 11, 5–18. [Google Scholar]
- Worden, J.W. Grief Counseling and Grief Therapy A Handbook for the Mental Health Practitioner, 5th ed.; Springer Publishing Company: New York, NY, USA, 2018; pp. 73–74. [Google Scholar]
- Boehmer, S.; Luszczynska, A.; Schwarzer, R. Coping and quality of life after tumor surgery: Personal and social resources promote different domains of quality of life. Anxiety Stress Coping 2007, 20, 61–75. [Google Scholar] [CrossRef] [PubMed]
- Hill, J.; Holcombe, C.; Clark, L.; Boothby, M.R.K.; Hincks, A.; Fisher, J.; Tufail, S.; Salmon, P. Predictors of onset of depression and anxiety in the year after diagnosis of breast cancer. Psychol. Med. 2011, 41, 1429–1436. [Google Scholar] [CrossRef] [PubMed]
- Den Oudsten, B.L.; Van Heck, G.L.; Van der Steeg, A.F.W.; Roukema, J.A.; De Vries, J. Predictors of depressive symptoms 12 months after surgical treatment of early-stage breast cancer. Psychooncology 2009, 18, 1230–1237. [Google Scholar] [CrossRef] [PubMed]
- Attig, T. How We Grieve: Relearning the World, Rev. ed.; Oxford University Press: Oxford, NY, USA, 2011; pp. 47–48. [Google Scholar]
- Kübler-Ross, E.; Kessler, D. Grief and Grieving Finding the Meaning of Grief Through the Five Stages of Loss; Scribner: New York, NY, USA, 2005; pp. 7–28. [Google Scholar]
- Duffy, M.; Wild, J. Living with loss: A cognitive approach to prolonged grief disorder–incorporating complicated, enduring and traumatic grief. Behav. Cogn. Psychother. 2023, 56, 645–658. [Google Scholar] [CrossRef]
- Smith, K.V.; Rankin, H.; Ehlers, A. A qualitative analysis of loss-related memories after cancer loss: A comparison of bereaved people with and without prolonged grief disorder. Eur. J. Psychotraumatol. 2020, 11, 1789325. [Google Scholar] [CrossRef]
- Julião, M.; Chochinov, H.; Antunes, B.; Samorinha, C.; Faustino, C.; Lemos Caldas, M.; Bragança, A.; Vaz, M. The European Portuguese Posthumous Dignity Therapy Schedule of Questions: Initial development and validation. Palliat. Support. Care 2023, 21, 74–82. [Google Scholar] [CrossRef]
- Xiao, J.; Ming Chow, K.; Chow Choi, K.; Marques Ng, S.N.; Huang, C.; Ding, J.; Chan, C.W.H. Effects of family-oriented Dignity Therapy on dignity, depression and spiritual well-being of patients with lung cancer undergoing chemotherapy: A randomised controlled trial. Int. J. Nurs. Stud. 2022, 129, 104217. [Google Scholar] [CrossRef]


{kind=link}
| n | % | M | SD | ||
|---|---|---|---|---|---|
| Gender | Female | 7 | 87.50 | ||
| Male | 1 | 12.50 | |||
| Age | 38.38 | 11.86 | |||
| Patient’s degree of kinship | Father/Mother | 6 | 75.00 | ||
| Husband/Wife | 1 | 12.50 | |||
| Granddaughter | 1 | 12.50 | |||
| Time elapsed since death | Less than 1 year | 1 | 12.50 | ||
| 1 to 2 years | 1 | 12.50 | |||
| 2 to 3 years | 3 | 37.50 | |||
| More than 3 years | 3 | 37.50 |
| Categories and Subcategories | P 1 | Ref.es | Excerpt | |
|---|---|---|---|---|
| Promoted adaptation | ||||
| Positive | 6 | 6 | “I… honestly I only see positive points (…)” (P1) | |
| Prognosis acknowledgment | 3 | 4 | “Although he knew, he had the notion that… of what was going on” (P4) | |
| Private space | 2 | 2 | “(…) he even told me that he liked it because he talked about things he didn’t talk about, that he hadn’t talked to anyone ….” (P5) | |
| Partially | 2 | 2 | “In a way, yes, although knowing his personality, I know that he was always going to be like this, that he was always going to react this way” (P2) | |
| Believing so | 1 | 1 | “I believe so… yes, I believe so.” (P1) | |
| Help in difficult times | 1 | 1 | “It always helps in these difficult moments, because a person is very sensitive and a little… desperate, isn’t it?” (P4) | |
| Helped facing | 1 | 1 | “Yes, it always helps a bit, isn’t it? … Because talking… it always helps a bit (…)” (P4) | |
| Cheer/relief | 1 | 1 | “(…) I remember that at least he left a bit more… cheerful (…), relieved, yes….” (P8) | |
| Assurance of psychological well-being | 1 | 1 | “I mean I want to believe that it psychologically helped him keep some sanity … (emotional) until the end.” (P8) | |
| Did not promote adaptation | ||||
| Conspiracy of Silence | 4 | 4 | “My father was never one to show himself to be “weak”, he always wanted to be strong for the family, he always hid this from my mother. He always… every letter, every exam he received he never showed my mother (…)” (P2) | |
| Categories and Subcategories | P 1 | Ref.es | Excerpt |
|---|---|---|---|
| Promoted adaptation | |||
| Helped facing | 5 | 7 | “Yes, of course, it always helped.” (P4) |
| Prognosis acknowledgment | 2 | 2 | “Because actually I have always known what would happen to her.” (P5) |
| Private space | 1 | 1 | “I remember the times when I spoke with the Doctors at the time (…) I had another perspective of looking at the problem, which was (…) very big in my life. (…) and unburden too (…) and maybe think things differently. There were things I didn’t talk about, maybe with my mother or with other people.” (P8) |
| Did not promote adaptation | |||
| Did not help | 2 | 2 | “To me it didn’t (a bit emotional).” (P2) |
| Need for parallel support | 1 | 1 | “I believe at the time me as a daughter… maybe having a session… being with the Psychologist that followed her or… would have helped me.” (P5) |
| Categories e Subcategories | P 1 | Ref.es | Excerpt |
|---|---|---|---|
| For patients | |||
| Revealing of what was being felt | 1 | 2 | “It was important because (…) in that letter he expressed a little more about what he was feeling. Until then he never... I tried talking to him and he never, never expressed much.” (P2) |
| Revealing of future plans | 1 | 2 | “And there in the letter, right, the way he talks… about a lot of things and everything, maybe things that he wasn’t going to tell anyone because, in his future plans, he was meant to live, not to die (…)” (P7) |
| For FCs | |||
| Importance in adaptation | |||
| Yes | 6 | 7 | “Yes… it helped, it did. (…) That letter helped me a little to accept it, sure.” (P2) |
| No | 1 | 1 | “In that regard I won’t say (…) that the letter was important…. (…). It was important, but not in that aspect (…)” (P3) |
| Helped | 1 | 1 | “(…) I believe that… that at the time I didn’t quite understand the meaning of that, but after some time I realized what it meant, that she externalized what she felt, right? In several ways, and that has helped us all.” (P1) |
| Content | |||
| Reinforcement of what was transmitted in life | 1 | 2 | “What he wrote is what he told me every day.” (P7) |
| Mother’s character | 1 | 1 | “Because that was exactly what my mother was, an honest person, of honour…” (P1) |
| Afraid of its content | 1 | 1 | “I wanted to, but I believe I was afraid. (…) of what was in there.” (P5) |
| Feeling towards the family | 1 | 1 | “(…) he explained there how much he cared for us, his family. He cared about family very much.” (P4) |
| Mirrors what was being felt | 1 | 1 | “What he wrote there is what he felt.” (P7) |
| Meaning | |||
| Importance for future generations | 6 | 7 | “It can because he has small grandchildren that are still unable to understand life, right? And they… (…) they know his grandfather but, of course, as the years go by that… that can be lost and I believe it’s a beautiful memory of him (…)” (P2) |
| Importance for the family | 6 | 6 | “(…) my sisters even said “look we have to make copies so that each one gets, each one with the … (…) letter, with what was written in it.”” (P3) |
| Affective relationship | 2 | 4 | “And that she really liked me. I knew it, but… the… seeing it in the letter, having been told to someone else who wrote it...” (P5) |
| Satisfaction | 2 | 3 | “(…) and I was very pleased with it, absolutely…. I was very pleased with the letter.” (P5) |
| Farewell | 1 | 2 | “(…) I see in that letter almost a way for her to say goodbye to me, to…. Because we didn’t actually have that (…).” (P5) |
| Emotion | 2 | 2 | “(…) what I felt. Look, a lot of emotion.” (P3) |
| Importance for the FC | 2 | 2 | “It was, to me.” (P2) |
| Feeling of comfort | 2 | 2 | “(...) when, for example, when it’s been her death or her birthday... or when I feel a bit sadder it comforts a little…” (P1) |
| Tattoo | 1 | 2 | “I even tattooed her, I tattooed a sentence that is there.” (P1) |
| Good relationship | 1 | 1 | “Well… I felt that I actually had… I had a good relationship with her.” (P5) |
| “It allowed proximity” | 1 | 1 | “Actually, for me it was good, it was good because my father wasn’t someone that shared a lot of… his emotions and in that letter he showed a bit more and it was good, (…) it allowed to be a bit closer to him, let’s say.” (P2) |
| Comfort and memory | 1 | 1 | “(...) exactly what my mother was (...) and that comforts me. There are times in which due to the whole process we went through you know, of seeing her degrade day after day, we forget a little bit who she was, before having anything. And that reminds us.” (P1) |
| Remembering and helping with longing | 1 | 1 | “Well, I… I hold on to everything, right? That letter is good for when… (…) I miss her a lot (…)” (P7) |
| Only memory | 1 | 1 | “(…) it’s the only thing I keep from my mother, is that letter.” (P1) |
| Categories and Subcategories | P 1 | Ref.es | Excerpt |
|---|---|---|---|
| Psychological Support | |||
| No | 6 | 6 | “No, no.” (P4) |
| Need for support | 1 | 1 | “(…) maybe I needed it at the time and I have a good family support that helped me a lot, but (…)… a talk would be very important.” (P5) |
| Yes | 2 | 2 | “I had an appointment a month ago (…)” (P7) |
| Made the process easier | 1 | 1 | “Let’s say that (…) it helped me not only in the process of my mother, but also in other problems (...). And me being well resolved with everything else facilitated the grieving process.” (P1) |
| Post-loss difficulties | |||
| Absence | 2 | 3 | “(…) her not being there. And the things that are happening to us, she… not sharing with her. (…) the longing, me wanting to tell her, share something of mine with her, good, bad… and she is not there.” (P5) |
| Only family member | 2 | 3 | “It’s more... I have an uncle who is single and lived with her and, since my grandmother’s passing, he isn’t doing well at all and it is difficult, (...) he continues to live in the house that was my grandmother’s and it is very difficult to be there with him.” (P6) |
| Longing | 2 | 2 | “I feel… I miss him every day, I wish I had him here (…)” (P8) |
| Absence of guidance | 1 | 1 | “I think it’s not having her approval (...) sometimes I feel lost (...)” (P1) |
| Absence of company | 1 | 1 | “The company, the advices when I get home, always having that friendly word… Going home to be with him.” (P7) |
| Difficulty in going to the graveyard | 1 | 1 | “I don’t feel like going to the cemetery, but I never liked cemeteries. And it’s a little difficult for me to go (...). And I think it’s a bit difficult for me to divide his emotional presence that I have at home and... physical that I think he doesn’t even want to be there anymore. But knowing that is where he, where he is.” (P8) |
| Dealing with other family members’ suffering | 1 | 1 | “(…) my mother still doesn’t accept it. And it is very difficult, even living with my mother is very difficult, at this moment.” (P2) |
| How one is feeling | |||
| Longing | 3 | 5 | “Look, right now… I miss her. Missing….” (P5) |
| Mission accomplished | 3 | 4 | “And it really helped me knowing that I always did the best with her. Everything that was, that was possible, that… that… there was nothing left to do with her.” (P5) |
| Acceptance | 1 | 2 | “I think I’m accepting it, I think I’m moving towards acceptance.” (P7) |
| Emotional anesthesia | 1 | 2 | “(...) I believe I’ve handled it well and I think it’s something I’m proud of myself, was to deal with... with all this that wasn’t easy. But I think I had... those 2 years of treatments and everything, I think, I think... they taught me something. (...) I think I... I don’t know, people say they get tougher or... No, but sometimes I’m afraid that I might start to become a cold person (...)” (P8) |
| Good | 2 | 2 | “I feel good, I accepted it well.” (P6) |
| Missing | 1 | 1 | “Because at this moment I miss her a lot (...)” (P1) |
| Did not get over | 1 | 1 | “I did not overcome it very well…. (…) It is difficult for me to talk about him.” (P2) |
| Denial of reality | 1 | 1 | “(…) sometimes I’m waiting for him to be discharged from the hospital.” (P7) |
| “I think about her” | 1 | 1 | “(…) I won’t say that I don’t think about her, I do, of course.” (P3) |
| Feeling calm | 1 | 1 | “(…) I felt calm for the first time.” (P8) |
| Help facing the loss | |||
| Mission accomplished | 2 | 5 | “I think I was... I think I did everything I could have done for him. I was always present, I came to all the treatments, I went to all the appointments. We always talk about this. My father told me, I believe, everything he had to say to me. I told him everything I had to say too. (...) I strongly believe everything has been said, (...) I feel at peace, that’s it.” (P8) |
| Family | 4 | 4 | “What helps me is my family. I have two children, it’s being with my children. I rely a lot on them, on my wife (...)” (P2) |
| Reason and finitude | 1 | 2 | “People like me have an end and like… we all have an end don’t we. The reason turned out to be… we will pass the time and it will, things have to happen.” (P5) |
| Re-encounter | 1 | 2 | “Knowing that one day I will find him.” (P7) |
| Psychology Appointments | 1 | 1 | “Very honestly, appointments with (…) helped me a lot… a lot, without a doubt.” (P1) |
| Space reorganization | 1 | 1 | “When I’m at home, if I’m tidying up the house, I remember him (…). And I already moved all the furniture in the house. (…) It’s not so that I don’t feel… so that his chair isn’t empty.” (P7) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Freitas, M.J.; Remondes-Costa, S.; Veiga, E.; Macedo, G.; Teixeira, R.J.; Leite, M. Life beyond Loss: A Retrospective Analysis of the Impact of Meaning of Life Therapy on the Grieving Process of Cancer Patients’ Family Caregivers. Healthcare 2024, 12, 471. https://doi.org/10.3390/healthcare12040471
Freitas MJ, Remondes-Costa S, Veiga E, Macedo G, Teixeira RJ, Leite M. Life beyond Loss: A Retrospective Analysis of the Impact of Meaning of Life Therapy on the Grieving Process of Cancer Patients’ Family Caregivers. Healthcare. 2024; 12(4):471. https://doi.org/10.3390/healthcare12040471
Chicago/Turabian StyleFreitas, Maria João, Sónia Remondes-Costa, Elisa Veiga, Gerly Macedo, Ricardo João Teixeira, and Manuela Leite. 2024. "Life beyond Loss: A Retrospective Analysis of the Impact of Meaning of Life Therapy on the Grieving Process of Cancer Patients’ Family Caregivers" Healthcare 12, no. 4: 471. https://doi.org/10.3390/healthcare12040471