

Knowledge, Attitudes, and Practices of Parents in the Use of Antibiotics: A Case Study in a Mexican Indigenous Community
 ,
,
Abstract
:1. Background
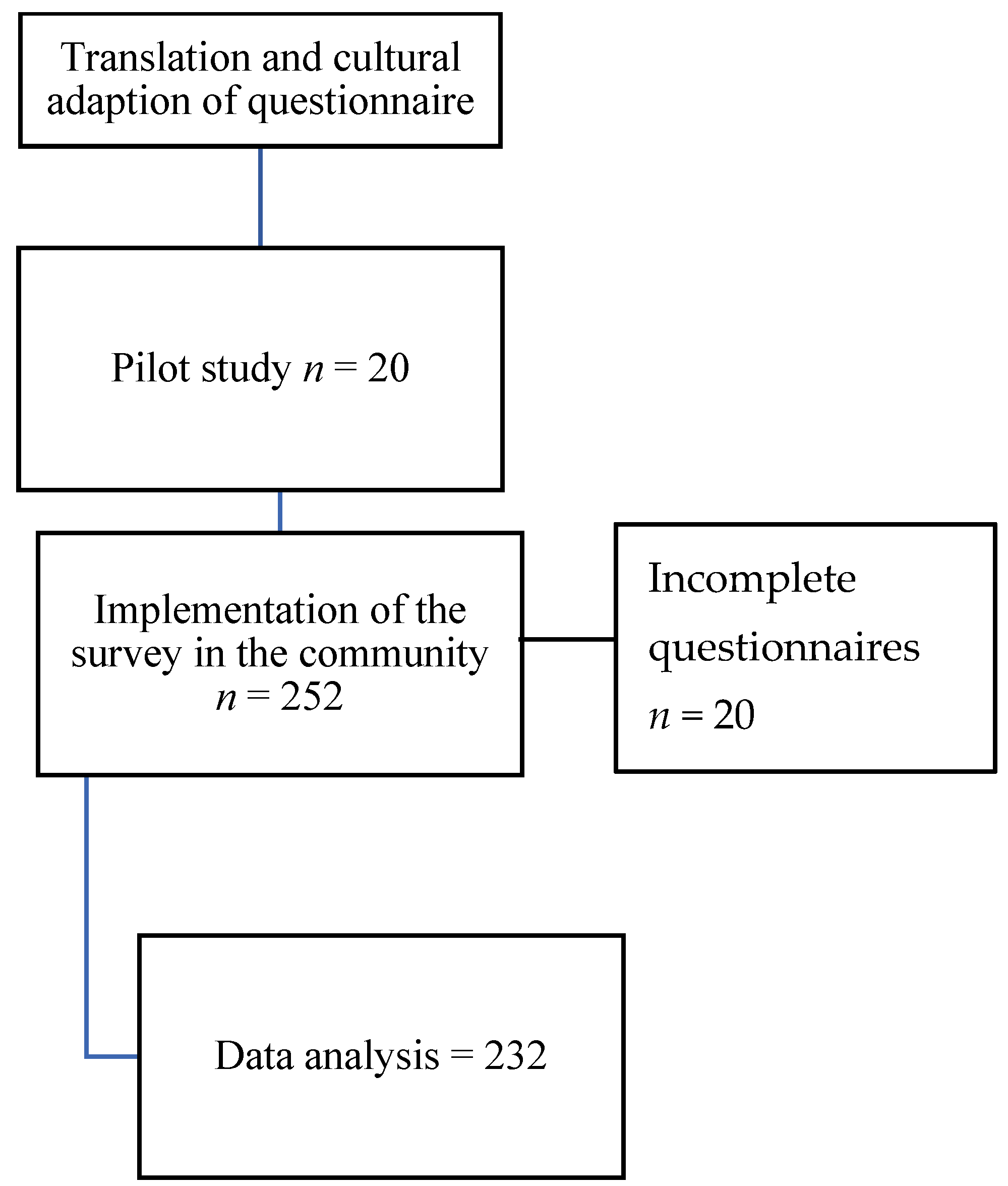
2. Methods
2.1. Description of Population
2.1.1. Knowledge, Attitudes, and Practices Questionnaire
- -
- Totally disagree;
- -
- Disagree;
- -
- Undecided;
- -
- Agree;
- -
- Totally agree.
2.1.2. Statistical Analysis of the Data
3. Results
3.1. Sociodemographic Characteristics
3.2. Knowledge
3.3. Attitudes
3.4. Practices
3.4.1. Use of Antibiotics in the Community
3.4.2. Use of Home Remedies
3.5. Association Analysis
4. Discussion
Social Conditions Related to Bacterial Resistance Increase
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO’s First Global Report on Antibiotic Resistance Reveals Serious, Worldwide Threat to Public Health; WHO: Geneva, Switzerland, 2014; Available online: https://www.who.int/news/item/30-04-2014-who-s-first-global-report-on-antibiotic-resistance-reveals-serious-worldwide-threat-to-public-health#:~:text=30%20April%202014%20%7C%20Geneva%20%2D%20A,anyone%2C%20of%20any%20age%2C%20inDate (accessed on 1 February 2023).
- Thriemer, K.; Katuala, Y.; Batoko, B.; Alworonga, J.-P.; Devlieger, H.; Van Geet, C.; Ngbonda, D.; Jacobs, J. Antibiotic prescribing in DR Congo: A knowledge, attitude and practice survey among medical doctors and students. PLoS ONE 2013, 8, e55495. [Google Scholar] [CrossRef]
- Okeke, I.N.; Lamikanra, A.; Edelman, R. Socioeconomic and behavioral factors leading to acquired bacterial resistance to antibiotics in developing countries. Emerg. Infect. Dis. 1999, 5, 18. [Google Scholar] [CrossRef]
- Harris, A.M.; Hicks, L.A.; Qaseem, A.; High Value Care Task Force of the American College of Physicians and for the Centers for Disease Control and Prevention. Appropriate antibiotic use for acute respiratory tract infection in adults: Advice for high-value care from the American College of Physicians and the Centers for Disease Control and Prevention. Ann. Intern. Med. 2016, 164, 425–434. [Google Scholar] [CrossRef]
- Federal Drug Administration (FDA). Summary Report on Antimicrobials Sold or Distributed for Use in Food-Producing Animals. 2017. Available online: https://www.fda.gov/animal-veterinary/cvm-updates/fda-releases-annual-summary-report-antimicrobials-sold-or-distributed-2021-use-food-producing (accessed on 15 March 2023).
- Bhuyan, G.S.; Hossain, M.A.; Sarker, S.K.; Rahat, A.; Islam, M.T.; Haque, T.N.; Begum, N.; Qadri, S.K.; Muraduzzaman, A.; Islam, N.N. Bacterial and viral pathogen spectra of acute respiratory infections in under-5 children in hospital settings in Dhaka city. PLoS ONE 2017, 12, e0174488. [Google Scholar] [CrossRef]
- Dreser, A.; Wirtz, V.J.; Corbett, K.K.; Echániz, G. Uso de antibióticos en México: Revisión de problemas y políticas. Salud Pública de México 2008, 50, S480–S487. [Google Scholar] [CrossRef]
- Luque, C.Z. La medicina tradicional indígena en el México actual. Arqueología Mexicana 2005, 13, 62–65. [Google Scholar]
- Secretaría de Desarrollo Social. Informe Anual Sobre la Situación de Pobreza y Rezago Social 2018. San Miguel Suchixtepec, Oaxaca; Subsecretaría de Planeación: Oaxaca, Mexico, 2018; p. 3. Available online: http://sisplade.oaxaca.gob.mx/sisplade/FichasFederal/2018/informe_municipal_20001.pdf (accessed on 15 December 2023).
- Malik, B.; Bhattacharyya, S. Antibiotic drug-resistance as a complex system driven by socio-economic growth and antibiotic misuse. Sci. Rep. 2019, 9, 9788. [Google Scholar] [CrossRef] [PubMed]
- Secretaría de Desarrollo Social. Informe Anual Sobre La Situación de Pobreza y Rezago Social. San Mguel Suchixtepec; Subsecretaría de Prospectiva: Oaxaca, México, 2023; Available online: https://www.gob.mx/cms/uploads/attachment/file/794256/20279-SanMiguelSuchixtepec23.pdf (accessed on 15 December 2023).
- Secretaría de Desarrollo Social. Informe Anual sobre la Situación de Pobreza y Rezago Social 2021. San Mateo Río Hondo; Subsecretaría de Planeación: Oaxaca, México, 2018; Available online: https://www.gob.mx/cms/uploads/attachment/file/612238/Informe_anual_2021_mun_20254.pdf (accessed on 15 December 2023).
- Secretaria de Desarrollo Social. Informe Anual Sobre la Situación de Pobreza y Rezago Social. San Mateo Río Hondo; Subsecretaría de Prospectiva: Oaxaca, México, 2023; Available online: https://www.gob.mx/cms/uploads/attachment/file/794231/20254-SanMateoRioHondo23.pdf (accessed on 1 January 2023).
- Ding, L.; Sun, Q.; Sun, W.; Du, Y.; Li, Y.; Bian, X.; He, G.; Bai, H.; Dyar, O.J. Antibiotic use in rural China: A cross-sectional survey of knowledge, attitudes and self-reported practices among caregivers in Shandong province. BMC Infect. Dis. 2015, 15, 576. [Google Scholar] [CrossRef] [PubMed]
- Holman, A. Knowledge, Attitude and Practice Surveys in Child Protection. A Step-by-Step Guide for Child Protection Programmes to the Design and Implementation of KAP Survey Methods. Save Child. 2012. Available online: https://resourcecentre.savethechildren.net/pdf/7245.pdf/ (accessed on 1 January 2023).
- Janzen, J.A.; Silvius, J.; Jacobs, S.; Slaughter, S.; Dalziel, W.; Drummond, N. What is a health expectation? Developing a pragmatic conceptual model from psychological theory. Health Expect. 2006, 9, 37–48. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Adherence to Long-Term Therapies: Evidence for Action; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Instituto Nacional de Estadística y Geografía (INEGI). Presenta INEGI Los Resultados de Una Nueva Serie de la Encuesta Nacional de Ingresos y Gastos de los Hogares; INEGI: Ciudad de México, México, 2016. Available online: https://www.inegi.org.mx/programas/enigh/nc/2016/ (accessed on 10 December 2023).
- Instituto Nacional de Estadística, Geografía e Informática. Escolaridad. México. 2020. Available online: https://www.inegi.org.mx/app/tabulados/interactivos/?pxq=Educacion_Educacion_05_2f6d2a08-babc-442f-b4e0-25f7d324dfe0 (accessed on 1 January 2023).
- Álvarez Castelló, M.; Castro Almarales, R.; Abdo Rodríguez, A.; Orta Hernández, S.D.; Gómez Martínez, M.; Álvarez Castelló, M.d.P. Infecciones respiratorias altas recurrentes: Algunas consideraciones. Rev. Cuba. Med. Gen. Integral 2008, 24. Available online: http://scielo.sld.cu/pdf/mgi/v24n1/mgi11108.pdf (accessed on 15 December 2023).
- Sonego, M.; Pellegrin, M.C.; Becker, G.; Lazzerini, M. Risk factors for mortality from acute lower respiratory infections (ALRI) in children under five years of age in low and middle-income countries: A systematic review and meta-analysis of observational studies. PLoS ONE 2015, 10, e0116380. [Google Scholar] [CrossRef] [PubMed]
- Pérez Sánchez, M.; Fundora Hernández, H.; Notario Rodríguez, M.; Rabaza Pérez, J.; Hernández Sánchez, M.d.l.Á.; Rodríguez Bertheau, A. Factores de riesgo inmunoepidemiológicos en niños con infecciones respiratorias recurrentes. Rev. Cuba. Pediatría 2011, 83, 225–235. [Google Scholar]
- Hernández-Díaz, I.; Ayala-Meléndez, A.; González-González, E.; Rosario-Calderón, I.; Figueroa-Ríos, D.; Melin, K.; Hernández-Muñoz, J.J. Knowledge and beliefs, behaviors, and adherence among Latino parents or legal guardians related to antibiotic use for upper respiratory tract infections in children under 6 years of age. J. Am. Pharm. Assoc. 2019, 59, 506–513. [Google Scholar] [CrossRef]
- Jensen, J.N.; Bjerrum, L.; Boel, J.; Jarløv, J.O.; Arpi, M. Parent´s socioeconomic factors related to high antibiotic prescribing in primary health care among children aged 0–6 years in the Capital Region of Denmark. Scand. J. Prim. Health Care 2016, 34, 274–281. [Google Scholar] [CrossRef]
- World Health Organization. WHO Global Strategy for Containment of Antimicrobial Resistance; World Health Organization: Geneva, Switzerland, 2001; Available online: https://www.who.int/publications/i/item/who-global-strategy-for-containment-of-antimicrobial-resistance (accessed on 5 December 2023).
- Pavydė, E.; Veikutis, V.; Mačiulienė, A.; Mačiulis, V.; Petrikonis, K.; Stankevičius, E. Public knowledge, beliefs and behavior on antibiotic use and self-medication in Lithuania. Int. J. Environ. Res. Public Health 2015, 12, 7002–7016. [Google Scholar] [CrossRef]
- Goberno de México. Acuerdo por el que se declara la obligatoriedad de la Estrategia Nacional de Acción contra la Resistencia a los Antimicrobianos. México. Diario Oficial de la Federación. 2018. Available online: https://www.gob.mx/senasica/documentos/resistencia-a-los-antimicrobianos?state=published (accessed on 10 December 2023).
- Mexico, G.d. Realizó IMSS Primer Taller Para Fortalecer Programas de Optimizacion de Antimicrobianos en Hospitales. 2023. Available online: https://www.imss.gob.mx/prensa/archivo/202306/287 (accessed on 1 January 2024).
- COFEPRIS. ¿Que es la resistencia antimicrobiana? MEXICO Agencia de Protección Sanitaria del Gobierno de la Ciudad de México, Ed.; Gobierno de la Ciudad de Mexico: Mexico City, Mexico, 2022; Available online: https://agepsa.cdmx.gob.mx/comunicacion/nota/que-es-la-resistencia-antimicrobiana (accessed on 1 January 2023).
- Panagakou, S.G.; Spyridis, Ν.; Papaevangelou, V.; Theodoridou, K.M.; Goutziana, G.P.; Theodoridou, M.N.; Syrogiannopoulos, G.A.; Hadjichristodoulou, C.S. Antibiotic use for upper respiratory tract infections in children: A cross-sectional survey of knowledge, attitudes, and practices (KAP) of parents in Greece. BMC Pediatr. 2011, 11, 60. [Google Scholar] [CrossRef]
- Pan, D.S.T.; Huang, J.H.; Lee, M.H.M.; Yu, Y.; Chen, M.I.-C.; Goh, E.H.; Jiang, L.; Chong, J.W.C.; Leo, Y.S.; Lee, T.H.; et al. Knowledge, attitudes and practices towards antibiotic use in upper respiratory tract infections among patients seeking primary health care in Singapore. BMC Fam. Pract. 2016, 17, 148. [Google Scholar] [CrossRef] [PubMed]
- Parimi, N.; Pinto Pereira, L.M.; Prabhakar, P. Caregivers’ practices, knowledge and beliefs of antibiotics in paediatric upper respiratory tract infections in Trinidad and Tobago: A cross-sectional study. BMC Fam Pract. 2004, 5, 28. [Google Scholar] [CrossRef] [PubMed]
- Vallin, M.; Polyzoi, M.; Marrone, G.; Rosales-Klintz, S.; Wisell, K.T.; Lundborg, C.S. Knowledge and attitudes towards antibiotic use and resistance-a latent class analysis of a Swedish population-based sample. PLoS ONE 2016, 11, e0152160. [Google Scholar] [CrossRef] [PubMed]
- Grigoryan, L.; Burgerhof, J.G.; Degener, J.E.; Deschepper, R.; Lundborg, C.S.; Monnet, D.L.; Scicluna, E.A.; Birkin, J.; Haaijer-Ruskamp, F.M. Determinants of self-medication with antibiotics in Europe: The impact of beliefs, country wealth and the healthcare system. J. Antimicrob. Chemother. 2008, 61, 1172–1179. [Google Scholar] [CrossRef] [PubMed]
- Sánchez, A.E.N.; Ishihara, M.I. Las plantas empleadas para el tratamiento de las infecciones respiratorias en los altos de Chiapas (México). Etnobiología 2010, 8, 11–30. [Google Scholar]
- Mendelson, M.; Matsoso, M.P. The World Health Organization global action plan for antimicrobial resistance. South Afr. Med. J. 2015, 105, 325. [Google Scholar] [CrossRef]
- Baars, E.W.; Zoen, E.B.-v.; Breitkreuz, T.; Martin, D.; Matthes, H.; Schoen-Angerer, T.v.; Soldner, G.; Vagedes, J.; Wietmarschen, H.v.; Patijn, O.; et al. The Contribution of Complementary and Alternative Medicine to Reduce Antibiotic Use: A Narrative Review of Health Concepts, Prevention, and Treatment Strategies. Evid.-Based Complement. Altern. Med. 2019, 2019, 5365608. [Google Scholar] [CrossRef]
- Ben-Arye, E.; Dudai, N.; Eini, A.; Torem, M.; Schiff, E.; Rakover, Y. Treatment of upper respiratory tract infections in primary care: A randomized study using aromatic herbs. Evid.-Based Complement. Altern. Med. 2011, 2011, 690346. [Google Scholar] [CrossRef]
- Howell, L.; Kochhar, K.; Saywell, R.; Zollinger, T.; Koehler, J.; Mandzuk, C.; Sutton, B.; Sevilla-Martir, J.; Allen, D. Use of herbal remedies by Hispanic patients: Do they inform their physician? J. Am. Board Fam. Med. 2006, 19, 566–578. [Google Scholar] [CrossRef]
- Lindquist, R.; Tracy, M.F.; Snyder, M. Complementary and Alternative Therapies in Nursing; Springer Publishing Company: Berlin/Heidelberg, Germany, 2018. [Google Scholar]
- Alós, J.-I. Resistencia bacteriana a los antibióticos: Una crisis global. Enfermedades Infecc. Y Microbiol. Clín. 2015, 33, 692–699. [Google Scholar] [CrossRef]
- Langdon, E.; Braune, W. Antropología, salud y enfermedad: Una introducción al concepto de cultura aplicado a las ciencias de la salud. Rev Lat.-Am Enferm. 2010, 18, 177–185. [Google Scholar]
- Ransford, H.E.; Carrillo, F.R.; Rivera, Y. Health care-seeking among Latino immigrants: Blocked access, use of traditional medicine, and the role of religion. J. Health Care Poor Underserved 2010, 21, 862–878. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, S.; Gorski, L. Antimicrobial Resistance and Antimicrobial Stewardship in Home Healthcare. Home Healthc. Now 2021, 39, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Cingolani, M.; Scendoni, R.; Fedeli, P.; Cembrani, F. Artificial intelligence and digital medicine for integrated home care services in Italy: Opportunities and limits. Front. Public Health 2023, 10, 1095001. [Google Scholar] [CrossRef] [PubMed]
- Anahtar, M.N.; Yang, J.H.; Kanjilal, S. Applications of machine learning to the problem of antimicrobial resistance: An emerging model for translational research. J. Clin. Microbiol. 2021, 59, e0126020. [Google Scholar] [CrossRef] [PubMed]
- Saleem, H.; Zengin, G.; Ahmad, I.; Lee, J.T.B.; Htar, T.T.; Mahomoodally, F.M.; Naidu, R.; Ahemad, N. Multidirectional insights into the biochemical and toxicological properties of Bougainvillea glabra (Choisy.) aerial parts: A functional approach for bioactive compounds. J. Pharm. Biomed. Anal. 2019, 170, 132–138. [Google Scholar] [CrossRef]
- Shareef, H.K.; Muhammed, H.J.; Hussein, H.M.; Hameed, I.H. Antibacterial effect of ginger (Zingiber officinale) roscoe and bioactive chemical analysis using gas chromatography mass spectrum. Orient. J. Chem. 2016, 32, 20–40. [Google Scholar] [CrossRef]
- Munekata, P.E.; Alcántara, C.; Žugčić, T.; Abdelkebir, R.; Collado, M.C.; García-Pérez, J.V.; Jambrak, A.R.; Gavahian, M.; Barba, F.J.; Lorenzo, J.M. Impact of ultrasound-assisted extraction and solvent composition on bioactive compounds and in vitro biological activities of thyme and rosemary. Food Res. Int. 2020, 134, 109242. [Google Scholar] [CrossRef]
- Akrayi, H.F.; Salih, R.M.; Hamad, P.A. In vitro screening of antibacterial properties of rhus coriaria and Origanum vulgare against some pathogenic bacteria. Aro-Sci. J. Koya Univ. 2015, 3, 35–41. [Google Scholar]
- Silva, N.; Fernandes Júnior, A. Biological properties of medicinal plants: A review of their antimicrobial activity. J. Venom. Anim. Toxins Incl. Trop. Dis. 2010, 16, 402–413. [Google Scholar] [CrossRef]
- Crosby, R.; Noar, S.M. What is a planning model? An introduction to PRECEDE-PROCEED. J. Public Health Dent. 2011, 71, S7–S15. [Google Scholar] [CrossRef] [PubMed]
- Cometto, M.C.; Zuñiga, R.A.A.; Flores, S.M.; Corona-Romero, A.M.; Hernández-Castellanos, E.; Márquez, N.C.; Restrepo, J.J.M.; Cardona, S.F.V.; del Pilar Gómez-González, M.; Chávez-Díaz, A. Epidemiología en la Era del Desarrollo Sostenible; Analéctica-Facultad de Ciencias Médicas de la Universidad Nacional de Córdoba: Córdoba, Argentina, 2021. [Google Scholar]
- Dávila Lárraga, L.G. ¿Cómo Funciona Prospera? Mejores Prácticas en la Implementación de Programas de Transferencias Monetarias Condicionadas en América Latina y el Caribe. 2016. Available online: https://publications.iadb.org/es/como-funciona-prospera-mejores-practicas-en-la-implementacion-de-programas-de-transferencias (accessed on 1 December 2023).
- Suárez-Herrera, J.C.; Blain, M.-J. La Recherche en Santé Mondiale: Perspectives Socio-Anthropologiques; ACFAS: Chicago, IL, USA, 2012. [Google Scholar]


{kind=link}
| Sociodemographic Characteristics | Expectations% | p | Adherence% | p | |||
|---|---|---|---|---|---|---|---|
| Low | High | Low | High | ||||
| Age of caregiver | ≤35 years | 52.9 | 47.1 | 0.663 | 30.9 | 69.1 | 0.002 * |
| ≥36 years | 48.6 | 51.4 | 52.7 | 47.3 | |||
| Sex of caregiver | Male | 46.2 | 53.8 | 0.615 | 45.5 | 54.5 | 0.459 |
| Female | 53.5 | 46.5 | 37.4 | 62.6 | |||
| Educational level | Basic | 56.1 | 43.9 | 0.309 | 40.3 | 59.7 | 0.308 |
| High school | 46.7 | 53.3 | 32.8 | 67.2 | |||
| Income level | Decile I | 54.2 | 45.8 | 0.785 | 38.6 | 61.4 | 0.436 |
| Decile II | 58.3 | 41.7 | 50.0 | 50.0 | |||
| Relationship to child | Parent | 54.5 | 45.5 | 0.070 | 38.5 | 61.5 | 0.722 |
| Other | 16.7 | 83.3 | 33.3 | 66.7 | |||
| Number of children | 1 | 53.5 | 46.5 | 0.811 | 34.3 | 65.7 | 0.116 |
| ≥2 | 51.2 | 48.8 | 45.0 | 55.0 | |||
| Age of child in this study | 3–5 years | 57.1 | 42.9 | 0.532 | 33.3 | 66.7 | 0.321 |
| 6–8 years | 51.2 | 48.8 | 40.3 | 59.7 | |||
| Sex of child in this study | Male | 50.8 | 49.2 | 0.660 | 38.7 | 61.3 | 0.864 |
| Female | 54.7 | 45.3 | 37.6 | 62.4 | |||
| Overcrowding | Moderate | 54.2 | 45.8 | 0.488 | 37.5 | 62.5 | 0.365 |
| Critical | 44.4 | 55.6 | 29.1 | 70.9 | |||
| Other characteristics | |||||||
| Use of home remedies | Yes | 60.0 | 40.0 | 0.391 | 40.6 | 59.4 | 0.633 |
| No | 51.0 | 49.0 | 37.2 | 62.8 | |||
| Factor when considering antibiotic use | Medical prescription | 54.5 | 45.5 | 0.412 | 35.1 | 64.9 | 0.002 * |
| Other | 42.9 | 57.1 | 72.2 | 27.8 | |||
| Adherence | Low | 33.8 | 66.2 | 0.412 | - | - | - |
| High | 41.1 | 58.9 | - | - | |||
| Sample Characteristics | Knowledge | p | Attitude | p | Practices | p | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Low | Medium | High | Negative | Positive | Negative | Positive | |||||
| Age of caregiver | ≤35 years | 119 | 23 | 1 | 0.703 | 54 | 89 | 0.006 * | 52 | 91 | 0.650 |
| ≥36 years | 77 | 77 | 1 | 50 | 39 | 35 | 54 | ||||
| Educational level | Low than national average | 159 | 23 | 1 | 0.124 | 89 | 94 | 0.02 * | 67 | 116 | 0.589 |
| High than national average | 37 | 11 | 1 | 15 | 34 | 20 | 29 | ||||
| Income level | Decile I | 184 | 32 | 2 | 989 | 100 | 118 | 0.378 | 81 | 137 | 0.431 |
| Decile II | 11 | 2 | 0 | 4 | 9 | 5 | 8 | ||||
| Decile III | 1 | 0 | 0 | 0 | 1 | 1 | 0 | ||||
| Use of home remedies | No | 60 | 9 | 2 | 0.579 | 32 | 37 | 0.758 | 28 | 41 | 0.528 |
| Yes | 136 | 25 | 3 | 72 | 91 | 59 | 104 | ||||
| Knowledge | Low | - | - | - | - | 90 | 106 | 0.149 | 72 | 124 | 0.184 |
| Medium | - | - | - | 12 | 22 | 13 | 21 | ||||
| High | - | - | - | 2 | 0 | 2 | 0 | ||||
| Attitudes | Negative | 90 | 12 | 2 | 0.149 | - | - | - | - | - | - |
| Positive | 106 | 22 | 0 | - | - | - | - | ||||
| Practices | Negative | 72 | 13 | 2 | 0.184 | 50 | 37 | 0.003 * | - | - | - |
| Positive | 124 | 21 | 0 | 54 | 91 | - | - | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
González-Villoria, A.M.; García Quiroz, A.D.; Osorio Guzmán, E.U.; Suarez-Herrera, J.C.; Abeldaño Zuñiga, R.A. Knowledge, Attitudes, and Practices of Parents in the Use of Antibiotics: A Case Study in a Mexican Indigenous Community. Healthcare 2024, 12, 294. https://doi.org/10.3390/healthcare12030294
González-Villoria AM, García Quiroz AD, Osorio Guzmán EU, Suarez-Herrera JC, Abeldaño Zuñiga RA. Knowledge, Attitudes, and Practices of Parents in the Use of Antibiotics: A Case Study in a Mexican Indigenous Community. Healthcare. 2024; 12(3):294. https://doi.org/10.3390/healthcare12030294
Chicago/Turabian StyleGonzález-Villoria, Ana María, Alma Delia García Quiroz, Edgar Ulises Osorio Guzmán, José Carlos Suarez-Herrera, and Roberto Ariel Abeldaño Zuñiga. 2024. "Knowledge, Attitudes, and Practices of Parents in the Use of Antibiotics: A Case Study in a Mexican Indigenous Community" Healthcare 12, no. 3: 294. https://doi.org/10.3390/healthcare12030294