
A Prospective Multicenter Longitudinal Analysis of Suicidal Ideation among Long-COVID-19 Patients
 ,
,  ,
,  , , , , , ,
, , , , , , {kind=link}
Abstract
:1. Introduction
1.1. Etiology of Suicide
1.2. Suicide Risk in Patients with Psychiatric and Physical Illnesses
1.3. Suicide Risk and COVID-19
1.4. Objective
2. Materials and Methods
2.1. Ethics Approval
2.2. Study Participants
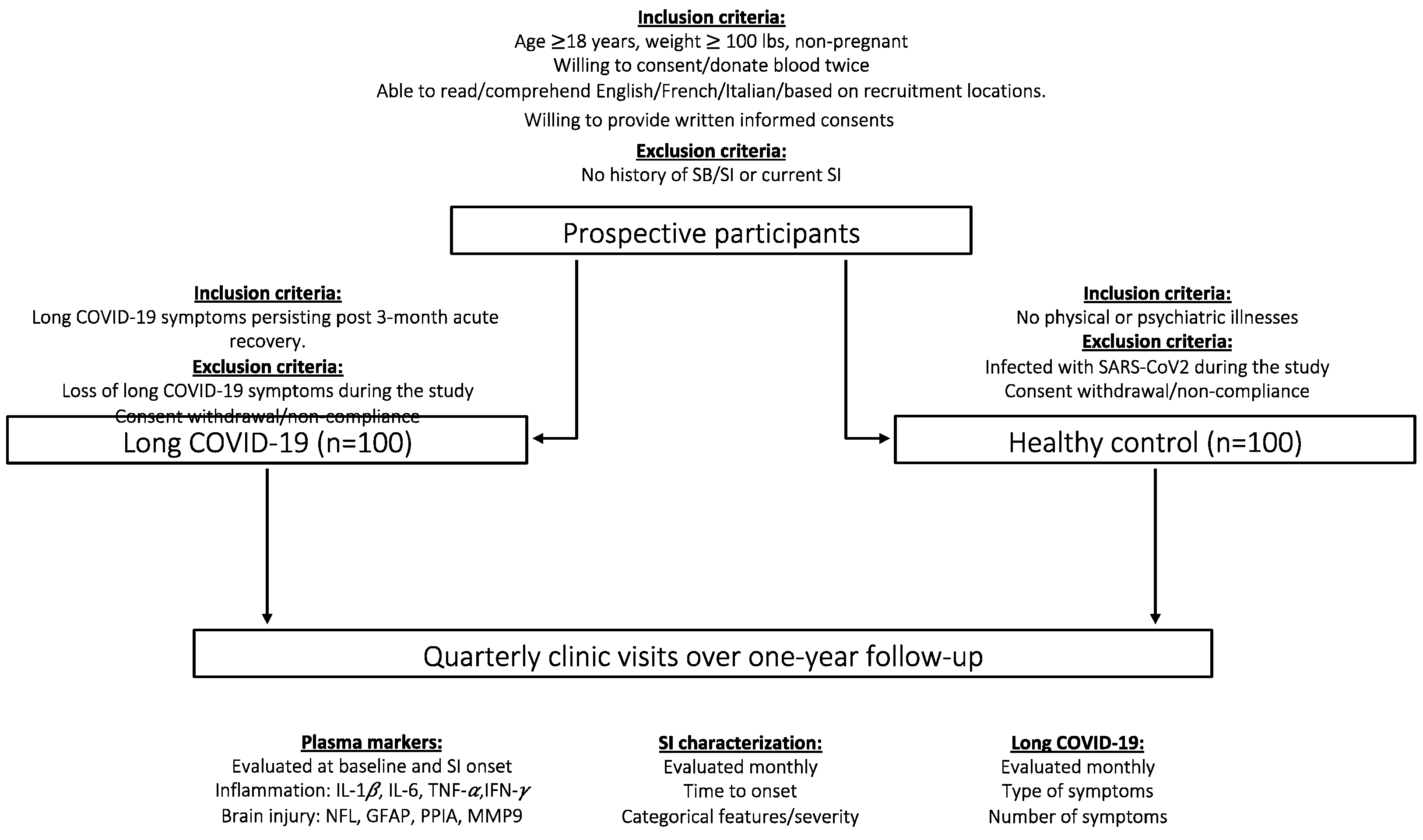
2.3. Study Design
2.4. Anticipated Outcomes
2.5. Diagnosis of Long COVID-19
2.6. Clinical Assessment of Psychiatric Illnesses
2.7. Clinical Assessment of SI
2.8. Blood Sample Collection
2.9. Plasma Inflammatory Mediator Measurement
2.10. Serious Adverse Events
2.11. Data Management
2.12. Data Analysis
3. Discussion
- specific alterations in inflammation markers can predict the development of SI;
- baseline levels of inflammation are correlated with the time it takes for SI to onset;
- SI-onset inflammation level is correlated with specific features/severity of SI.
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- van Heeringen, K.; Mann, J.J. The neurobiology of suicide. Lancet Psychiatry 2014, 1, 63–72. [Google Scholar] [CrossRef]
- Sudol, K.; Mann, J.J. Biomarkers of Suicide Attempt Behavior: Towards a Biological Model of Risk. Curr. Psychiatry Rep. 2017, 19, 31. [Google Scholar] [CrossRef]
- Hawton, K.; van Heeringen, K. Suicide. Lancet 2009, 373, 1372–1381. [Google Scholar] [CrossRef]
- Turecki, G. The molecular bases of the suicidal brain. Nat. Rev. Neurosci. 2014, 15, 802–816. [Google Scholar] [CrossRef] [PubMed]
- Serafini, G.; Costanza, A.; Aguglia, A.; Amerio, A.; Trabucco, A.; Escelsior, A.; Sher, L.; Amore, M. The Role of Inflammation in the Pathophysiology of Depression and Suicidal Behavior: Implications for Treatment. Med. Clin. N. Am. 2023, 107, 1–29. [Google Scholar] [CrossRef] [PubMed]
- Turecki, G.; Brent, D.A. Suicide and suicidal behaviour. Lancet 2016, 387, 1227–1239. [Google Scholar] [CrossRef]
- Hawton, K.; Casañas, I.; Comabella, C.; Haw, C.; Saunders, K. Risk factors for suicide in individuals with depression: A systematic review. J. Affect. Disord. 2013, 147, 17–28. [Google Scholar] [CrossRef] [PubMed]
- Turecki, G.; Ernst, C.; Jollant, F.; Labonté, B.; Mechawar, N. The neurodevelopmental origins of suicidal behavior. Trends Neurosci. 2012, 35, 14–23. [Google Scholar] [CrossRef] [PubMed]
- Rihmer, Z.; Rihmer, A.; Beltezcki, Z. Psycho-social correlates of suicidal behaviour. Neuropsychopharmacol. Hung. 2022, 24, 162–169. [Google Scholar]
- Costanza, A.; Chytas, V.; Piguet, V.; Luthy, C.; Mazzola, V.; Bondolfi, G.; Cedraschi, C. Meaning in Life Among Patients with Chronic Pain and Suicidal Ideation: Mixed Methods Study. JMIR Form. Res. 2021, 5, e29365. [Google Scholar] [CrossRef]
- Nafilyan, V.; Morgan, J.; Mais, D.; Sleeman, K.E.; Butt, A.; Ward, I.; Tucker, J.; Appleby, L.; Glickman, M. Risk of suicide after diagnosis of severe physical health conditions: A retrospective cohort study of 47 million people. Lancet Reg. Health Eur. 2022, 25, 100562. [Google Scholar] [CrossRef]
- Xiong, Q.; Tang, F.; Li, Y.; Xie, F.; Yuan, L.; Yao, C.; Wu, R.; Wang, J.; Wang, Q.; Feng, P. Association of inflammatory bowel disease with suicidalideation, suicide attempts, and suicide: A systematic review and meta-analysis. J. Psychosom. Res. 2022, 160, 110983. [Google Scholar] [CrossRef] [PubMed]
- Soleymani, E.; Faizi, F.; Heidarimoghadam, R.; Davoodi, L.; Mohammadi, Y. Association of T. gondii infection with suicide: A systematic review and meta-analysis. BMC Public Health 2020, 20, 766. [Google Scholar] [CrossRef] [PubMed]
- Burgdorf, K.S.; Trabjerg, B.B.; Pedersen, M.G.; Nissen, J.; Banasik, K.; Pedersen, O.B.; Sørensen, E.; Nielsen, K.R.; Larsen, M.H.; Erikstrup, C.; et al. Large-scale study of Toxoplasma and Cytomegalovirus shows an association between infection and serious psychiatric disorders. Brain Behav. Immun. 2019, 79, 152–158. [Google Scholar] [CrossRef]
- Costanza, A.; Amerio, A.; Aguglia, A.; Serafini, G.; Amore, M.; Hasler, R.; Ambrosetti, J.; Bondolfi, G.; Sampogna, G.; Berardelli, I.; et al. Hyper/neuroinflammation in COVID-19 and suicide etiopathogenesis: Hypothesis for a nefarious collision? Neurosci. Biobehav. Rev. 2022, 136, 104606. [Google Scholar] [CrossRef] [PubMed]
- Sher, L. Long COVID and the risk of suicide. Gen. Hosp. Psychiatry 2023, 80, 66–67. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, T.; Krammer, F.; Iwasaki, A. The first 12 months of COVID-19: A timeline of immunological insights. Nat. Rev. Immunol. 2021, 21, 245–256. [Google Scholar] [CrossRef] [PubMed]
- Russell, C.D.; Lone, N.I.; Baillie, J.K. Comorbidities, multimorbidity and COVID-19. Nat. Med. 2023, 29, 334–343. [Google Scholar] [CrossRef] [PubMed]
- Mehandru, S.; Merad, M. Pathological sequelae of long-haul COVID. Nat. Immunol. 2022, 23, 194–202. [Google Scholar] [CrossRef]
- Hartung, T.J.; Neumann, C.; Bahmer, T.; Chaplinskaya-Sobol, I.; Endres, M.; Geritz, J.; Haeusler, K.G.; Heuschmann, P.U.; Hildesheim, H.; Hinz, A.; et al. Fatigue and cognitive impairment after COVID-19: A prospective multicenter study. EClinicalMedicine 2022, 53, 101651. [Google Scholar] [CrossRef]
- Sher, L. The impact of the COVID-19 pandemic on suicide rates. QJM 2020, 113, 707–712. [Google Scholar] [CrossRef]
- Taquet, M.; Skorniewska, Z.; Hampshire, A.; Chalmers, J.D.; Ho, L.P.; Horsley, A.; Marks, M.; Poinasamy, K.; Raman, B.; Leavy, O.C.; et al. Acute blood biomarker profiles predict cognitive deficits 6 and 12 months after COVID-19 hospitalization. Nat. Med. 2023, 29, 2498–2508. [Google Scholar] [CrossRef]
- Reger, M.A.; Stanley, I.H.; Joiner, T.E. Suicide Mortality and Coronavirus Disease 2019-A Perfect Storm? JAMA Psychiatry 2020, 77, 1093–1094. [Google Scholar] [CrossRef]
- Gunnell, D.; Appleby, L.; Arensman, E.; Hawton, K.; John, A.; Kapur, N.; Khan, M.; O’Connor, R.C.; Pirkis, J. COVID-19 Suicide Prevention Research Collaboration. Suicide risk and prevention during the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 468–471. [Google Scholar] [CrossRef] [PubMed]
- Niederkrotenthaler, T.; Gunnell, D.; Arensman, E.; Pirkis, J.; Appleby, L.; Hawton, K.; John, A.; Kapur, N.; Khan, M.; O’Connor, R.C.; et al. International COVID-19 Suicide Prevention Research Collaboration. Suicide Research, Prevention, and COVID-19. Crisis 2020, 41, 321–330. [Google Scholar] [CrossRef] [PubMed]
- Costanza, A.; Amerio, A.; Aguglia, A.; Serafini, G.; Amore, M. Meaning in Life and Demoralization Constructs in Light of the Interpersonal Theory of Suicide: A Trans-Theoretical Hypothesis for a Cross-Sectional Study. Psychol. Res. Behav. Manag. 2020, 13, 855–858. [Google Scholar] [CrossRef] [PubMed]
- Aguglia, A.; Amerio, A.; Costanza, A.; Parodi, N.; Copello, F.; Serafini, G.; Amore, M. Hopelessness and Post-Traumatic Stress Symptoms among Healthcare Workers during the COVID-19 Pandemic: Any Role for Mediating Variables? Int. J. Environ. Res. Public Health 2021, 18, 6579. [Google Scholar] [CrossRef] [PubMed]
- Amerio, A.; Bertuccio, P.; Santi, F.; Bianchi, D.; Brambilla, A.; Morganti, A.; Odone, A.; Costanza, A.; Signorelli, C.; Aguglia, A.; et al. Gender Differences in COVID-19 Lockdown Impact on Mental Health of Undergraduate Students. Front. Psychiatry 2022, 12, 813130. [Google Scholar] [CrossRef]
- Aguglia, A.; Giacomini, G.; Montagna, E.; Amerio, A.; Escelsior, A.; Capello, M.; Cutroneo, L.; Ferretti, G.; Scafidi, D.; Costanza, A.; et al. Meteorological Variables and Suicidal Behavior: Air Pollution and Apparent Temperature Are Associated With High-Lethality Suicide Attempts and Male Gender. Front. Psychiatry 2021, 12, 653390. [Google Scholar] [CrossRef]
- Boldrini, T.; Girardi, P.; Clerici, M.; Conca, A.; Creati, C.; Di Cicilia, G.; Ducci, G.; Durbano, F.; Maci, C.; Maone, A.; et al. Italian Network for Research on Mental Health during COVID-19 Pandemic. Consequences of the COVID-19 pandemic on admissions to general hospital psychiatric wards in Italy: Reduced psychiatric hospitalizations and increased suicidality. Prog. Neuropsychopharmacol. Biol. Psychiatry 2021, 110, 110304. [Google Scholar] [CrossRef]
- Montalbani, B.; Bargagna, P.; Mastrangelo, M.; Sarubbi, S.; Imbastaro, B.; De Luca, G.P.; Anibaldi, G.; Erbuto, D.; Pompili, M.; Comparelli, A. The COVID-19 Outbreak and Subjects with Mental Disorders Who Presented to an Italian Psychiatric Emergency Department. J. Nerv. Ment. Dis. 2021, 209, 246–250. [Google Scholar] [CrossRef] [PubMed]
- Kavukcu, E.; Akdeniz, M. Tsunami after the novel coronavirus (COVID-19) pandemic: A global wave of suicide? Int. J. Soc. Psychiatry 2021, 67, 197–199. [Google Scholar] [CrossRef] [PubMed]
- Thakur, V.; Jain, A. COVID 2019-suicides: A global psychologicalpandemic. Brain Behav. Immun. 2020, 88, 952–953. [Google Scholar] [CrossRef] [PubMed]
- Pirkis, J.; John, A.; Shin, S.; DelPozo-Banos, M.; Arya, V.; Analuisa-Aguilar, P.; Appleby, L.; Arensman, E.; Bantjes, J.; Baran, A.; et al. Suicide trends in the early months of the COVID-19 pandemic: An interrupted time-series analysis of preliminary data from 21 countries. Lancet Psychiatry 2021, 8, 579–588. [Google Scholar] [CrossRef] [PubMed]
- Phiri, P.; Ramakrishnan, R.; Rathod, S.; Elliot, K.; Thayanandan, T.; Sandle, N.; Haque, N.; Chau, S.W.; Wong, O.W.; Chan, S.S.; et al. An evaluation of the mental health impact of SARS-CoV-2 on patients, general public and healthcare professionals: A systematic review and meta-analysis. EClinicalMedicine 2021, 34, 100806. [Google Scholar] [CrossRef]
- Leske, S.; Kõlves, K.; Crompton, D.; Arensman, E.; de Leo, D. Real-time suicide mortality data from police reports in Queensland, Australia, during the COVID-19 pandemic: An interrupted time-series analysis. Lancet Psychiatry 2021, 8, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Dubé, J.P.; Smith, M.M.; Sherry, S.B.; Hewitt, P.L.; Stewart, S.H. Suicide behaviors during the COVID-19 pandemic: A meta-analysis of 54 studies. Psychiatry Res. 2021, 301, 113998. [Google Scholar] [CrossRef] [PubMed]
- Merad, M.; Blish, C.A.; Sallusto, F.; Iwasaki, A. The immunology and immunopathology of COVID-19. Science 2022, 375, 1122–1127. [Google Scholar] [CrossRef]
- Steardo, L., Jr.; Steardo, L.; Scuderi, C. Astrocytes and the Psychiatric Sequelae of COVID-19: What We Learned from the Pandemic. Neurochem. Res. 2023, 48, 1015–1025. [Google Scholar] [CrossRef]
- Costanza, A.; Placenti, V.; Amerio, A.; Aguglia, A.; Serafini, G.; Amore, M.; Macchiarulo, E.; Branca, F.; Merli, R.; Bondolfi, G.; et al. Chloroquine/Hydroxychloroquine Use and Suicide Risk: Hypotheses for Confluent Etiopathogenetic Mechanisms. Behav. Sci. 2021, 11, 154. [Google Scholar] [CrossRef]
- Premraj, L.; Kannapadi, N.V.; Briggs, J.; Seal, S.M.; Battaglini, D.; Fanning, J.; Suen, J.; Robba, C.; Fraser, J.; Cho, S.M. Mid and long-term neurological and neuropsychiatric manifestations of post-COVID-19 syndrome: A meta-analysis. J. Neurol. Sci. 2022, 434, 120162. [Google Scholar] [CrossRef] [PubMed]
- Magdy, R.; Elmazny, A.; Soliman, S.H.; Elsebaie, E.H.; Ali, S.H.; Abdel Fattah, A.M.; Hassan, M.; Yassien, A.; Mahfouz, N.A.; Elsayed, R.M.; et al. Post-COVID-19 neuropsychiatric manifestations among COVID-19 survivors suffering from migraine: A case-control study. J. Headache Pain. 2022, 23, 101. [Google Scholar] [CrossRef] [PubMed]
- Tirozzi, A.; Santonastaso, F.; de Gaetano, G.; Iacoviello, L.; Gialluisi, A. Does COVID-19 increase the risk of neuropsychiatric sequelae? Evidence from a mendelian randomization approach. World J. Psychiatry 2022, 12, 536–540. [Google Scholar] [CrossRef] [PubMed]
- Bagheri, M.; Ghaneialvar, H.; Oshnokhah, M.; Salari, S. GFAP and Neuron Specific Enolase (NSE) in the Serum of Suicide Attempters. Med. J. Islam. Repub. Iran. 2022, 36, 103. [Google Scholar] [CrossRef] [PubMed]
- Ramezani, M.; Simani, L.; Fard, M.G.; Abbaszadeh, F.; Shadnia, S. Increased levels of neurofilament light chain in suicide attempters’ serum. Transl. Neurosci. 2022, 13, 218–223. [Google Scholar] [CrossRef] [PubMed]
- Schultheiß, C.; Willscher, E.; Paschold, L.; Gottschick, C.; Klee, B.; Henkes, S.S.; Bosurgi, L.; Dutzmann, J.; Sedding, D.; Frese, T.; et al. The IL-1β, IL-6, and TNF cytokine triad is associated with post-acute sequelae of COVID-19. Cell Rep. Med. 2022, 3, 100663. [Google Scholar] [CrossRef] [PubMed]
- Woodward, S.F.; Bari, S.; Vike, N.; Lalvani, S.; Stetsiv, K.; Kim, B.W.; Stefanopoulos, L.; Maglaveras, N.; Breiter, H.; Katsaggelos, A.K. Anxiety, Post-COVID-19 Syndrome-Related Depression, and Suicidal Thoughts and Behaviors in COVID-19 Survivors: Cross-sectional Study. JMIR Form. Res. 2022, 6, e36656. [Google Scholar] [CrossRef]
- Xie, Y.; Xu, E.; Al-Aly, Z. Risks of mental health outcomes in people with COVID-19: Cohort study. BMJ 2022, 376, e068993. [Google Scholar] [CrossRef]
- Thaweethai, T.; Jolley, S.E.; Karlson, E.W.; Levitan, E.B.; Levy, B.; McComsey, G.A.; McCorkell, L.; Nadkarni, G.N.; Parthasarathy, S.; Singh, U.; et al. Development of a Definition of Postacute Sequelae of SARS-CoV-2 Infection. JAMA 2023, 329, 1934–1946. [Google Scholar] [CrossRef]
- Cano-Montalbán, I.; Quevedo-Blasco, R. Sociodemographic variables most associated with suicidal behaviour and suicide methods in Europe and America. A systematic review. Eur. J. Psychol. Appl. Leg. Context. 2018, 10, 15–25. [Google Scholar] [CrossRef]
- Bastien, C.H.; Vallières, A.; Morin, C.M. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep. Med. 2001, 2, 297–307. [Google Scholar] [CrossRef]
- Spinhoven, P.; Ormel, J.; Sloekers, P.P.; Kempen, G.I.; Speckens, A.E.; Van Hemert, A.M. A validation study of the Hospital Anxiety and Depression Scale (HADS) in different groups of Dutch subjects. Psychol. Med. 1997, 27, 363–370. [Google Scholar] [CrossRef]
- Aalto, A.M.; Elovainio, M.; Kivimäki, M.; Uutela, A.; Pirkola, S. The Beck Depression Inventory and General Health Questionnaire as measures of depression in the general population: A validation study using the Composite International Diagnostic Interview as the gold standard. Psychiatry Res. 2012, 197, 163–171. [Google Scholar] [CrossRef]
- Blevins, C.A.; Weathers, F.W.; Davis, M.T.; Witte, T.K.; Domino, J.L. The Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5): Development and Initial Psychometric Evaluation. J. Trauma. Stress. 2015, 28, 489–498. [Google Scholar] [CrossRef] [PubMed]
- Bourque, P.; Beaudette, D. Étude psychometrique du questionnaire de dépression de Beck auprès d’un échantillon d’étudiants universitaires francophones. Can. J. Behav. Sci. 1982, 14, 211–218. [Google Scholar] [CrossRef]
- Beck, A.T.; Kovacs, M.; Weissman, A. Assessment of suicidal intention: The Scale for Suicide Ideation. J. Consult. Clin. Psychol. 1979, 47, 343–352. [Google Scholar] [CrossRef] [PubMed]
- Bonetto, V.; Pasetto, L.; Lisi, I.; Carbonara, M.; Zangari, R.; Ferrari, E.; Punzi, V.; Luotti, S.; Bottino, N.; Biagianti, B.; et al. Markers of blood-brain barrier disruption increase early and persistently in COVID-19 patients with neurological manifestations. Front. Immunol. 2022, 13, 1070379. [Google Scholar] [CrossRef] [PubMed]
- Gasnier, M.; Choucha, W.; Radiguer, F.; Faulet, T.; Chappell, K.; Bougarel, A.; Kondarjian, C.; Thorey, P.; Baldacci, A.; Ballerini, M.; et al. COMEBAC study group. Comorbidity of longCOVID and psychiatric disorders after a hospitalisation for COVID-19: A cross-sectional study. J. Neurol. Neurosurg. Psychiatry 2022, 93, 1091–1098. [Google Scholar] [CrossRef] [PubMed]
- Brønnum-Hansen, H.; Davidsen, M.; Thorvaldsen, P.; Danish MONICA Study Group. Long-term survival and causes of death after stroke. Stroke 2001, 32, 2131–2136. [Google Scholar] [CrossRef]
- Pompili, M.; Venturini, P.; Campi, S.; Seretti, M.E.; Montebovi, F.; Lamis, D.A.; Serafini, G.; Amore, M.; Girardi, P. Do stroke patients have an increased risk of developing suicidal ideation or dying by suicide? An overview of the current literature. CNS Neurosci. Ther. 2012, 18, 711–721. [Google Scholar] [CrossRef]
- Teasdale, T.W.; Engberg, A.W. Suicide after a stroke: A population study. J. Epidemiol. Community Health 2001, 55, 86386. [Google Scholar] [CrossRef] [PubMed]
- Keiser, O.; Spoerri, A.; Brinkhof, M.W.; Hasse, B.; Gayet-Ageron, A.; Tissot, F.; Christen, A.; Battegay, M.; Schmid, P.; Bernasconi, E.; et al. Suicide in HIV-infected individuals and the general population in Switzerland, 1988-2008. Am. J. Psychiatry 2010, 167, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Marzuk, P.M.; Tardiff, K.; Leon, A.C.; Hirsch, C.S.; Hartwell, N.; Portera, L.; Iqbal, M.I. HIV seroprevalence among suicide victims in New York City, 1991-1993. Am. J. Psychiatry 1997, 154, 1720–1725. [Google Scholar] [CrossRef] [PubMed]
- Roy, A. Characteristics of HIV patients who attempt suicide. Acta Psychiatr. Scand. 2003, 107, 41–44. [Google Scholar] [CrossRef] [PubMed]
- Kurella, M.; Kimmel, P.L.; Young, B.S.; Chertow, G.M. Suicide in the United States end-stage renal disease program. J. Am. Soc. Nephrol. 2005, 16, 774–781. [Google Scholar] [CrossRef] [PubMed]
- Brønnum-Hansen, H.; Stenager, E.; Nylev Stenager, E.; Koch-Henriksen, N. Suicide among Danes with multiple sclerosis. J. Neurol. Neurosurg. Psychiatry 2005, 76, 1457–1459. [Google Scholar] [CrossRef] [PubMed]
- Fredrikson, S.; Cheng, Q.; Jiang, G.X.; Wasserman, D. Elevated suicide risk among patients with multiple sclerosis in Sweden. Neuroepidemiology 2003, 22, 146–152. [Google Scholar] [CrossRef]
- Pompili, M.; Forte, A.; Palermo, M.; Stefani, H.; Lamis, D.A.; Serafini, G.; Amore, M.; Girardi, P. Suicide risk in multiple sclerosis: A systematic review of current literature. J. Psychosom. Res. 2012, 73, 411–417. [Google Scholar] [CrossRef]
- Ásgeirsdóttir, H.G.; Valdimarsdóttir, U.A.; Þorsteinsdóttir, Þ.K.; Lund, S.H.; Tomasson, G.; Nyberg, U.; Ásgeirsdóttir, T.L.; Hauksdóttir, A. The association between different traumatic life events and suicidality. Eur. J. Psychotraumatol. 2018, 9, 1510279. [Google Scholar] [CrossRef]
- Biswas, T.; Scott, J.G.; Munir, K.; Renzaho, A.M.N.; Rawal, L.B.; Baxter, J.; Mamun, A.A. Global variation in the prevalence of suicidal ideation, anxiety and their correlates among adolescents: A population based study of 82 countries. EClinicalMedicine 2020, 24, 100395. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costanza, A.; Amerio, A.; Aguglia, A.; Magnani, L.; Alexander, J.; Maiorano, A.; Richard-Lepouriel, H.; Portacolone, E.; Berardelli, I.; Pompili, M.; et al. A Prospective Multicenter Longitudinal Analysis of Suicidal Ideation among Long-COVID-19 Patients. Healthcare 2024, 12, 290. https://doi.org/10.3390/healthcare12030290
Costanza A, Amerio A, Aguglia A, Magnani L, Alexander J, Maiorano A, Richard-Lepouriel H, Portacolone E, Berardelli I, Pompili M, et al. A Prospective Multicenter Longitudinal Analysis of Suicidal Ideation among Long-COVID-19 Patients. Healthcare. 2024; 12(3):290. https://doi.org/10.3390/healthcare12030290
Chicago/Turabian StyleCostanza, Alessandra, Andrea Amerio, Andrea Aguglia, Luca Magnani, Jacques Alexander, Alessandra Maiorano, Hélène Richard-Lepouriel, Elena Portacolone, Isabella Berardelli, Maurizio Pompili, and et al. 2024. "A Prospective Multicenter Longitudinal Analysis of Suicidal Ideation among Long-COVID-19 Patients" Healthcare 12, no. 3: 290. https://doi.org/10.3390/healthcare12030290